Otospongiosis, its classifications, etiopathogenesis and management
Reading File
Finding Sources
Searching PubMed
otosclerosis otospongiosis management
Searching the Web
otospongiosis classification etiopathogenesis management 2024 2025
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
I now have all the material needed. Let me compile the comprehensive answer.
Otospongiosis (Otosclerosis)
Terminology
The terms otospongiosis and otosclerosis refer to two histological phases of the same disease. "Otospongiosis" (coined by Siebenmann, 1912) describes the active, spongiotic, highly vascular phase; "otosclerosis" (Politzer, 1893) describes the inactive, sclerotic, hardened phase. The preferred histopathological term is otospongiosis; clinically, "otosclerosis" is still widely used.
The disease is unique to the otic capsule. The normal otic capsule is the most stable bone in the body - it undergoes virtually no remodeling after ossification - making otospongiosis a striking exception to normal bone biology.
- Cummings Otolaryngology Head and Neck Surgery, p. 2779
- Shambaugh Surgery of the Ear
Epidemiology
| Parameter | Data |
|---|---|
| Histological prevalence (Whites) | ~8-10% |
| Clinical prevalence (Whites) | 0.3-0.4% |
| Female : Male | 2:1 (up to 3:1 for severe disease) |
| Bilaterality | ~75% |
| Age of onset | 3rd decade (teens to early 30s) |
| Positive family history | ~60% |
| Race | Most common in Caucasians; rare in Blacks (~0.9% histological), Asians (1.48% histological), Native Americans |
Only ~12% of temporal bones with histological otosclerosis have stapes ankylosis, so most histological disease never becomes clinical.
- Cummings Otolaryngology, p. 2779; Scott-Brown's Vol 2
Classification
1. Anatomical / Topographical Classification
Fenestral (stapedial) otosclerosis
- Most common form (~85%)
- Lesion at the fissula ante fenestram (the embryologic remnant just anterior to the oval window)
- Causes fixation of the stapes footplate → conductive hearing loss (CHL)
- Can progress to partially or completely obliterate the oval window niche
Retrofenestral (cochlear) otosclerosis
- Lesion extends into the cochlear capsule, round window, or elsewhere in the labyrinthine capsule
- Produces sensorineural hearing loss (SNHL) via:
- Collagen deposition in the spiral ligament with hyalinization of the stria vascularis
- Toxic enzymes released by active lesions into perilymph
- CT sign: "double-ring effect" (band of demineralization surrounding the cochlear canal); "fourth ring of Valvassori" (low density ring around otic capsule)
- Often a continuum of fenestral disease spreading medially
Mixed / Combined
- Both fenestral and cochlear involvement → mixed CHL + SNHL
2. Footplate Classification (Operative Appearance)
| Type | Description |
|---|---|
| Type 1 (Anterior fixation) | Lesion at anterior footplate / fissula ante fenestram; footplate mobile posteriorly |
| Type 2 (Total obliteration) | Entire footplate replaced - "biscuit" or "obliterative" footplate |
| Type 3 (Bipolar fixation) | Both anterior and posterior annular ligament involved |
| Floating footplate | Footplate inadvertently mobilized during surgery |
3. Histological Classification
- Active (otospongiotic) phase: Osteoclast-rich, highly vascular, basophilic lesions with widened marrow spaces (blue mantles of Manasse)
- Inactive (sclerotic) phase: Dense, disorganized, hypocellular sclerotic bone; sparse vascularity
4. Clinical Stage (Audiological)
-
Early: Small air-bone gap, mainly low-frequency; intact reflexes may show diphasic (on-off) pattern
-
Moderate: Air-bone gap >30 dB; absent acoustic reflex; Carhart notch at 2000 Hz on bone conduction
-
Severe / Far Advanced Otosclerosis (FAO): Combined CHL + SNHL; cochlear implantation territory
-
Cummings Otolaryngology, p. 2778-2780; Scott-Brown's Vol 2, p. 836-887; Shambaugh Surgery of the Ear
Histopathology
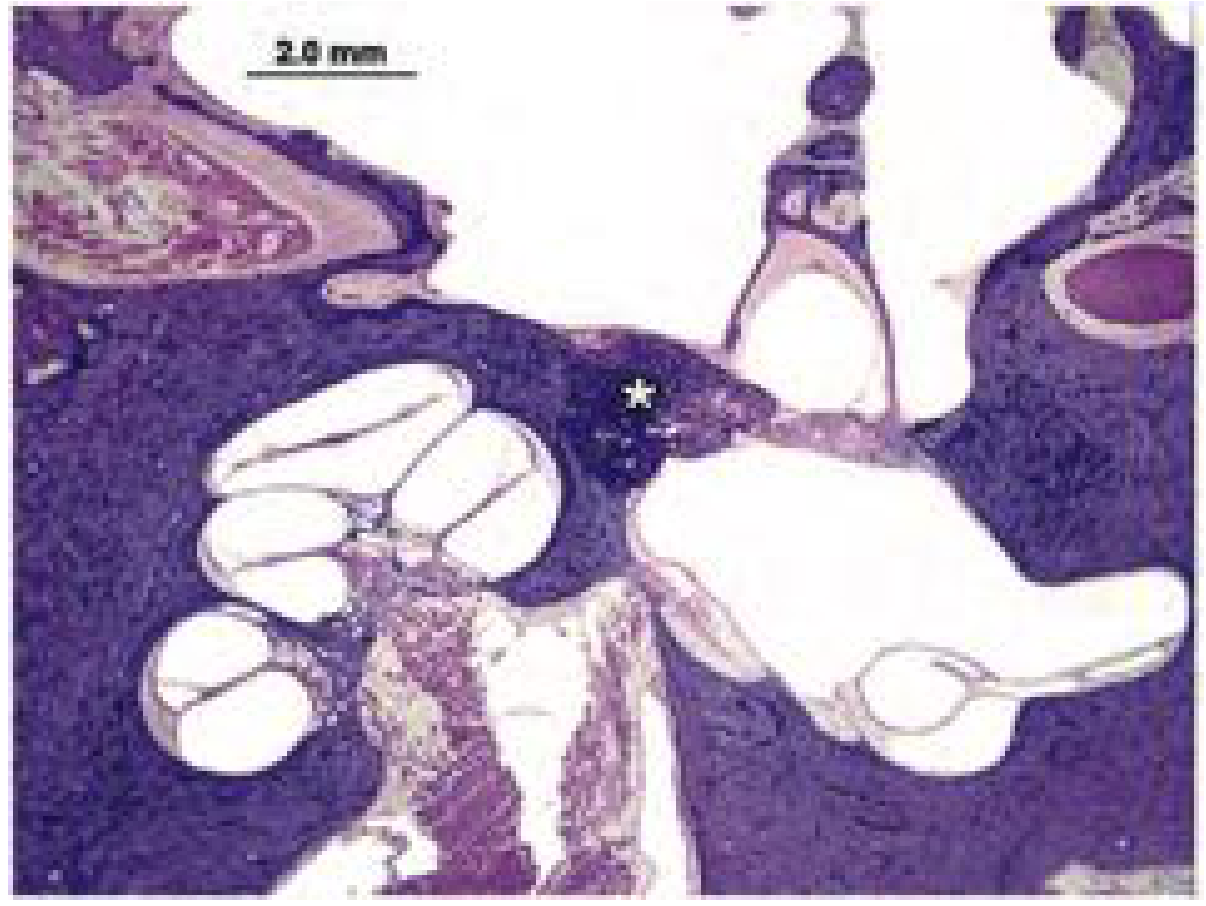
H&E stained section: stapes footplate and anterior oval window with adjacent otosclerotic process (asterisk). Stapes footplate bone is replaced by otosclerotic bone causing fixation. - Cummings Otolaryngology
The initial osteoclastic (spongiotic) phase shows:
- Resorption of normal lamellar otic capsule bone
- Pseudovascular spaces with connective tissue
- Multinucleated osteoclasts at the advancing lesion edge
- Lesions extend in finger-like projections and show affinity for hematoxylin (appear darker)
- Adjacent to the fissula ante fenestram initially
The subsequent osteoblastic (sclerotic) phase:
-
Dense, disorganized sclerotic bone replaces the resorbed areas
-
Widened marrow spaces later replaced by hypocellular sclerotic bone
-
Results in fixation of the stapes via the annular ligament
-
Cummings Otolaryngology, p. 2779
Etiopathogenesis
The etiopathogenesis is multifactorial and not fully understood. The key contributing factors are:
1. Genetic Factors
- Autosomal dominant inheritance with variable (incomplete) penetrance of 25-40%
- Up to 60% have a positive family history
- Sporadic cases account for 40-50%
- Nine chromosomal loci identified: OTSC1 through OTSC8, plus COL1A1 (type I collagen)
- COL1A1 mutations are the best characterized - otosclerotic bone shows abnormal collagen I, similar to osteogenesis imperfecta
- Disease more common in Whites (10x vs. Blacks), suggesting strong genetic component
2. Viral (Measles / Paramyxovirus) Hypothesis
- Measles RNA sequences (from paramyxovirus nucleoprotein and receptor-binding protein genes) have been detected within otosclerotic lesions by PCR
- Proposed mechanism: persistent measles virus infection drives local inflammatory bone remodeling in genetically susceptible individuals
- The decline in otosclerosis prevalence in fluoride-supplemented water areas and post-MMR vaccination populations provides indirect support
- This remains a hypothesis, not proven
3. Hormonal Factors
- Female predominance (2:1), and pregnancy accelerates progression in many patients
- Estrogen receptors have been identified in otosclerotic bone
- Oral contraceptives were historically thought to worsen otosclerosis (now less certain)
- Many women first report hearing loss during or shortly after first pregnancy
4. Autoimmune / Inflammatory Factors
- Elevated levels of TGF-β1 (transforming growth factor beta-1) in perilymph of otosclerotic ears
- TGF-β1 promotes osteoclast differentiation and bone resorption
- Some role for interleukin-1 and other cytokines in active lesions
5. Bone Metabolism
-
The otic capsule normally undergoes NO remodeling after ossification (in contrast to all other bones in the body)
-
The fissula ante fenestram is a narrow fibrocartilaginous zone rich in persistence embryonic cartilage - this site is metabolically unique and predisposed to the otospongiotic process
-
Fluoride in drinking water appears protective: communities with >1 ppm fluoride have lower prevalence, and the global decline in otosclerosis has been partly attributed to water fluoridation
-
Cummings Otolaryngology, pp. 2779-2780; Scott-Brown's Vol 2
Clinical Presentation
Symptoms:
- Slowly progressive bilateral CHL (75%) - asymmetric in onset
- Paracusis Willisii: paradoxically hearing better in noisy environments (because others raise their voice; masked by their own cochlear noise at quiet)
- Tinnitus (low-frequency)
- Vestibular symptoms in cochlear otosclerosis or with perifenestral involvement
Signs:
- Tympanic membrane: normal in appearance
- Schwartz sign (Schwartze sign): reddish/pinkish blush visible through the tympanic membrane over the promontory in active otospongiosis - indicates hypervascular active lesion. Requires a clear eardrum and occurs in ~10% of cases.
- Classic description: "The doctor sees nothing, and the patient hears nothing"
Tuning fork tests:
- Weber: lateralizes to worse ear (more conductive loss)
- Rinne: BC > AC (negative Rinne) - 512 Hz reversal indicates >20-25 dB CHL
Investigations
Audiometry
- Air-bone gap predominantly in low frequencies initially
- Carhart notch: dip in bone conduction at 2000 Hz - a mechanical artifact of stapes fixation (not true SNHL), disappears after successful stapes surgery
- Speech discrimination preserved until SNHL supervenes
Impedance Audiometry
- Tympanogram: Type As (reduced compliance, normal peak pressure) - indicates stapes fixation
- Acoustic reflexes: absent (early disease may show diphasic/on-off reflex)
- Normal middle ear pressure (type A or As tympanogram)
Imaging (HRCT Temporal Bone)
-
Not required for typical fenestral otosclerosis
-
Fissula ante fenestram: radiolucency anterior to oval window (earliest sign)
-
Narrowing or obliteration of oval window niche in advanced disease
-
"Double-ring effect" in cochlear otosclerosis
-
"Halo sign": hypodense ring around cochlea indicating retrofenestral involvement - predicts SNHL component
-
"Fourth ring of Valvassori": low-density band around otic capsule on axial CT
-
CT is >95% sensitive for detecting otosclerosis
-
Shambaugh Surgery of the Ear; Cummings Otolaryngology, p. 2780; Scott-Brown's Vol 2, p. 861-872
Management
Management options are: (1) surveillance/no treatment, (2) hearing aids, (3) medical therapy, (4) stapes surgery, and rarely (5) cochlear implantation.
A. Hearing Aids
- Effective for CHL and valid first-line option, particularly for patients who decline surgery
- Conventional air-conduction hearing aids work well for pure CHL
- Bone-anchored hearing aids (BAHA): useful for mixed loss or failed surgery
- Patient should be counselled that hearing aids are a fully acceptable and reversible alternative to surgery
B. Medical Management (Sodium Fluoride)
Sodium fluoride is an enzyme inhibitor that reduces osteoclastic bone resorption, thus slowing or arresting the progression of sensorineural loss in active cochlear otospongiosis.
Indications:
- Active cochlear (retrofenestral) otosclerosis with progressive SNHL (especially with positive Schwartz sign)
- After stapedectomy if SNHL continues to progress
- Poor surgical candidates
Dose: 25-40 mg/day of sodium fluoride, usually combined with calcium gluconate 500 mg and vitamin D 400 IU
Evidence: A Danish double-blind RCT (43 treated vs. 52 controls) showed significantly less air-conduction deterioration in the treated group over 12-24 months. Benefit seen in ~50% of patients.
Side effects: Dyspepsia (70%), gastrointestinal pain, synovitis, plantar fasciitis, anaemia - dose-dependent
Bisphosphonates: Early studies showed little benefit; newer third-generation bisphosphonates show some reduction in rate of progressive SNHL in cochlear otosclerosis. Under investigation.
- Scott-Brown's Vol 1 (sodium fluoride chapter); Scott-Brown's Vol 2, pp. 9238-9277
C. Surgical Management - Stapes Surgery
Stapes surgery is the definitive treatment for fenestral otosclerosis with CHL. It is the most effective intervention, restoring hearing in the vast majority of patients.
Indications for Surgery
- Conductive or mixed hearing loss due to otosclerosis
- Air-bone gap generally >25-30 dB
- 512-Hz tuning fork must reverse (BC > AC) - if it does not reverse, surgery carries higher risk of mobilizing a fixed stapes without improvement
- Good speech discrimination
- Patient preference after full counselling regarding risks vs. hearing aids
Contraindications
- Only hearing ear (relative - consider hearing aids first)
- Active middle ear infection
- Poor general health/anaesthetic risk
- Patients unable to comply with post-operative instructions
Types of Surgery
1. Stapedotomy (preferred - since the 1980s)
- A small fenestra (0.6-0.8 mm) is created in the footplate with a microdrill, laser (CO2, KTP, or argon), or micropick
- A piston prosthesis (Teflon/PTFE piston with wire or nitinol clip, typically 4.0-4.5 mm) is placed from the long process of the incus through the fenestra into the vestibule
- Advantages: less inner ear trauma, lower risk of SNHL, outpatient procedure
- Both vein-graft-covered and direct-placement techniques are acceptable
2. Partial Stapedectomy
- Removal of the posterior half of the footplate with tissue seal
3. Total Stapedectomy
- Complete removal of the footplate
- Covered by a fat, vein, or perichondrium graft
- Used for obliterative footplate or revision cases
Surgical steps (stapedotomy):
- Local or general anaesthesia; patient supine
- Transcanal approach via speculum under operating microscope
- Postero-superior tympanomeatal flap elevated
- Bony canal wall overhang removed to expose footplate, facial nerve, and pyramidal process
- Ossicular chain palpated to confirm stapes fixation
- Incus-to-footplate distance measured (typically 4.5 mm lateral, 4.0 mm medial surface)
- Laser or microdrill used to create 0.7-0.8 mm fenestra in center of footplate
- Posterior crus weakened and down-fractured
- Piston prosthesis placed through fenestra and crimped to incus
- Tissue seal (blood, fat, or vein graft) placed around prosthesis
- Tympanomeatal flap replaced
Prosthesis options: Teflon-platinum, stainless steel, nitinol (self-crimping, MRI-compatible), titanium
Hearing Outcomes
- Air-bone gap closure to within 10 dB: ~80-90% of cases
- Success rate (closure to within 20 dB): ~90-95%
Complications
| Complication | Frequency | Notes |
|---|---|---|
| Sensorineural hearing loss (SNHL) | <1% (0.2%) | Most devastating; risk higher in revision/obliterative cases |
| Chorda tympani injury | ~30% | Taste disturbance; usually resolves |
| Vertigo | Common transiently; persistent rare | Long prosthesis; positive fistula test |
| Tympanic membrane perforation | Rare | Usually heals spontaneously |
| Perilymph gusher | 0.03-0.2% | CSF flow; associated with X-linked stapes fixation |
| Floating footplate | Rare | Avoid removal; use short wire or close with vein graft |
| Reparative granuloma | Rare (1%) | Due to foreign body reaction; presents 1-2 weeks post-op |
| Incus necrosis | Long-term revision cause (26%) | Wire-loop prostheses at higher risk |
Far Advanced Otosclerosis
- When SNHL is severe to profound and surgery cannot restore serviceable hearing
- Cochlear implantation is indicated
- Results of CI in otosclerosis are generally good; obliterative cochlear otosclerosis may require modified electrode insertion (shorter electrode, drill-out of basal turn)
Revision Stapedectomy
-
More challenging than primary surgery; ~71-96% achieve air-bone gap closure within 20 dB
-
Risk of profound SNHL: 0-2%
-
Most common failure causes: displaced prosthesis (53%), incus erosion (26%), bony regrowth (14%)
-
Best performed under local anaesthesia for intraoperative monitoring
-
Cummings Otolaryngology, pp. 2780-2788; Scott-Brown's Vol 1, pp. 552-611
Recent Evidence (2023-2026)
Two relevant systematic reviews have been published:
-
General vs. Local Anaesthesia in Stapes Surgery (2026) - Bahrami et al., Laryngoscope 2026. A meta-analysis comparing anaesthetic approaches for stapedotomy. [PMID: 41165060]
-
Umbrella Review of Interventions for Otosclerosis (2026) - Chau et al., Otolaryngol Head Neck Surg 2026. A comprehensive umbrella review synthesizing evidence on diagnosis and management of otosclerosis. This is the most current high-level evidence summary available. [PMID: 41696966]
Summary Table
| Feature | Fenestral Otosclerosis | Cochlear Otosclerosis |
|---|---|---|
| Location | Fissula ante fenestram, oval window | Cochlear capsule, round window |
| Hearing loss | Conductive | Sensorineural |
| Schwartz sign | May be present | Usually present |
| Audiogram | Air-bone gap, Carhart notch | Flat SNHL |
| CT | Radiolucency at oval window | Double-ring effect, halo sign |
| Management | Stapedotomy / hearing aid | Sodium fluoride / CI |
Key point for exams: Otospongiosis is the active phase; otosclerosis is the sclerotic phase. The disease starts at the fissula ante fenestram. Inheritance is autosomal dominant with 25-40% penetrance. The Carhart notch (dip in bone conduction at 2000 Hz) is a mechanical artifact - not true SNHL - and resolves after stapedectomy. Stapedotomy is the surgery of choice over total stapedectomy.
This is a shared conversation. Sign in to Orris to start your own chat.