Bells palsy
Reading File
Finding Sources
Searching PubMed
"Bell palsy" treatment
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative sources. Here is a thorough summary:
Bell's Palsy
Definition & Epidemiology
Bell's palsy is the most common cause of acute unilateral facial paralysis. It is an idiopathic peripheral (lower motor neuron) palsy of CN VII (facial nerve). The annual incidence is approximately 23-25 per 100,000 (roughly 1 in 60 people over a lifetime). It affects men and women equally across all ages. Risk factors include:
- Pregnancy (especially the 3rd trimester and first 2 weeks postpartum - up to 3x increased risk)
- Diabetes mellitus
- Possibly hypertension
- Recurrences occur in ~7% of cases
Aetiology / Pathophysiology
The cause is now understood with reasonable certainty: reactivation of Herpes Simplex Virus type 1 (HSV-1) in the geniculate ganglion is responsible for the majority of cases. Evidence includes:
- HSV-1 DNA found by PCR in endoneurial fluid of the facial nerve in 11/14 Bell's palsy cases at surgery (Murakami et al., 1996)
- HSV-1 found in the geniculate ganglion at autopsy
- Mouse models reproduced facial palsy by inoculating HSV into ears and tongues
Varicella-Zoster Virus (VZV) may account for up to one-third of cases and is the second most frequent cause. SARS-CoV-2 and HIV seroconversion have also been implicated.
The inflammation causes swelling of the nerve within the rigid facial canal in the temporal bone, leading to ischemia and demyelination. Pathologically, there is mononuclear inflammatory cell infiltrate with varying degrees of nerve fiber degeneration.
Clinical Features
| Feature | Detail |
|---|---|
| Onset | Acute; 50% reach maximal weakness within 48 h; nearly all within 3-4 days |
| Weakness | Complete unilateral facial paralysis - upper AND lower face (distinguishes from UMN lesion) |
| Pain | Retroauricular (behind the ear) pain, often preceding paralysis by 1-2 days |
| Taste | Impaired taste (hypogeusia) unilaterally in most patients - chorda tympani involvement |
| Hyperacusis | Ipsilateral - due to stapedius muscle paralysis |
| Eye | Inability to close eye (lagophthalmos), Bell's phenomenon (eye rolls upward on attempted closure) |
| Sensory | Facial numbness/fullness (not true sensory loss in most) |
Key: both upper and lower face are involved - this is what distinguishes a lower motor neuron (peripheral) lesion from an upper motor neuron (central/cortical) lesion, where the forehead is spared (because upper facial muscles receive bilateral cortical input).
MRI Findings
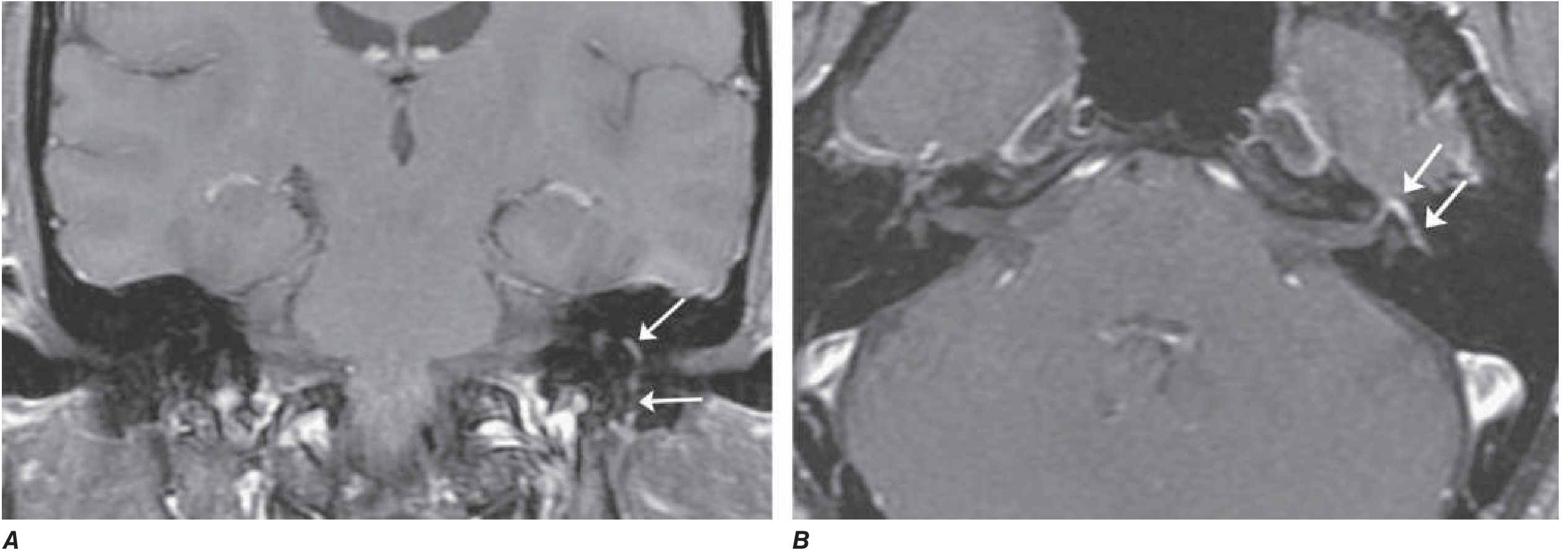
Axial and coronal T1-weighted MRI with gadolinium (fat suppression) showing diffuse smooth linear enhancement of the left facial nerve - involving the genu, tympanic, and mastoid segments within the temporal bone (arrows). Note: similar enhancement can be seen in Lyme disease, sarcoidosis, and perineural malignant spread. - Harrison's Principles of Internal Medicine 22E
MRI findings: swelling and uniform gadolinium enhancement of the geniculate ganglion and facial nerve. More pronounced enhancement correlates with worse prognosis.
Differential Diagnosis
The diagnosis of Bell's palsy is one of exclusion. Other causes of facial palsy to consider:
| Condition | Key Distinguishing Feature |
|---|---|
| Ramsay Hunt syndrome | VZV reactivation; vesicular rash in external ear canal, palate; CN VIII also affected; worse prognosis |
| Lyme disease | Endemic area; can be bilateral; positive Borrelia serology; >10% of facial palsy in endemic areas |
| Sarcoidosis | Often bilateral; ACE level, chest imaging |
| Guillain-Barré syndrome | Bilateral facial palsy; ascending weakness |
| Stroke / MS | UMN pattern - forehead spared; other neurological signs |
| Parotid tumor / acoustic neuroma | Progressive, slow onset; mass on imaging |
| HIV | Early seroconversion; HIV serology |
| Leprosy | Endemic areas |
| Melkersson-Rosenthal syndrome | Recurrent palsy + facial edema + fissured tongue |
| Carcinomatous meningitis | Signs of malignancy |
Diagnosis
Clinical diagnosis can be made when:
- Typical acute-onset unilateral facial palsy (upper + lower face)
- No risk factors or symptoms pointing to another cause
- No herpetic vesicles in the external ear canal (would suggest Ramsay Hunt)
- Normal neurological exam otherwise
In atypical/uncertain cases, consider: ESR/CRP, fasting glucose, Lyme titer, HIV serology, ACE level + chest imaging (sarcoidosis), lumbar puncture (GBS), or MRI.
EMG after 10 days: evidence of denervation indicates axonal degeneration, predicting a prolonged recovery (~3 months delay) that may be incomplete.
Treatment
First-Line: Corticosteroids (start early - within 72 hours)
- Prednisolone 25 mg twice daily x 10 days (Goldman-Cecil protocol)
- Or Prednisone 60-80 mg daily for 5 days, then tapered over 5 days (Harrison's protocol)
- Increases return of facial function from 63% to 83% at 3 months
Antivirals: Role is adjunctive, not standalone
- Large RCTs found no independent benefit of valacyclovir or acyclovir over steroids alone
- However, adding antivirals (valacyclovir 1000 mg/day x 5-7 days, or acyclovir 400 mg 5x/day x 10 days) is indicated if:
- Vesicular lesions are seen (suspicion of Ramsay Hunt)
- Severe cases
- If VZV is suspected, double the acyclovir dose
Supportive / Eye Care (essential)
- Artificial tears during the day
- Paper tape to close eyelid during sleep (prevent corneal exposure/drying)
- Lubricating eye ointment at night
- Massage of weakened muscles
Surgery
- Facial nerve surgical decompression: reserved for severe/refractory cases
- Cosmetic procedures (e.g., temporalis muscle transposition, static slings) for permanent paralysis
Prognosis
- 70% recover completely within 1-2 months
- 85% achieve near-normal function
- ~10% have little or no recovery
- Favorable prognostic signs:
- Incomplete paralysis in the first week (most favorable)
- Return of taste in the first week
- Early motor function recovery within 5-7 days
- More pronounced nerve enhancement on MRI = worse prognosis
Complications of incomplete recovery:
- Synkinesis - aberrant nerve regeneration causing involuntary co-movements (e.g., "jaw winking" - eye closure when mouth moves)
- Crocodile tears - lacrimation during eating (aberrant reinnervation of lacrimal gland by salivatory fibers)
- Hemifacial spasm
Recent Evidence (2024-2026)
Recent systematic reviews have examined adjunctive therapies:
- Laser therapy for Bell's palsy (Lin et al., 2024, Lasers Med Sci): meta-analysis of RCTs shows photobiomodulation may have a role in accelerating recovery
- Physical therapy for idiopathic facial paralysis (Varelas et al., 2025, Am J Otolaryngol): systematic review supports physiotherapy as adjunctive management
- These do not overturn the primary steroid-based treatment but suggest adjunctive rehabilitation modalities have emerging evidence
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 452
- Adams and Victor's Principles of Neurology, 12th Ed., Chapter 16
- Goldman-Cecil Medicine, Chapter 388
This is a shared conversation. Sign in to Orris to start your own chat.