A 48 years old female with a history of knee pain originating from below knee, radiating to the lateral aspect of the lower limb, with pain during flexion of knee with Difficulty climbing stairs
Reading File
Finding Sources
Finding Sources
Searching the Web
lateral knee pain below knee radiating lateral limb pain on flexion difficulty climbing stairs diagnosis 48 year old female
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Searching Images
iliotibial band syndrome lateral knee anatomy diagram
Loading Image
Loading Image
Based on the comprehensive information gathered from multiple authoritative textbooks, here is a full clinical analysis:
Clinical Assessment: 48-Year-Old Female with Lateral Knee Pain
Most Likely Diagnosis: Iliotibial Band Syndrome (ITBS)
The clinical triad of:
- Pain originating below the knee (at Gerdy's tubercle / lateral tibial condyle)
- Radiating along the lateral aspect of the lower limb
- Pain on flexion of the knee and difficulty climbing stairs
...is the hallmark presentation of Iliotibial Band Syndrome (ITBS), also called IT band friction syndrome.
Anatomy & Pathomechanism
The iliotibial band (ITB) is a thick lateral condensation of the fascia lata running from the iliac crest → tensor fasciae latae and gluteus maximus → Gerdy's tubercle on the lateral tibial condyle.
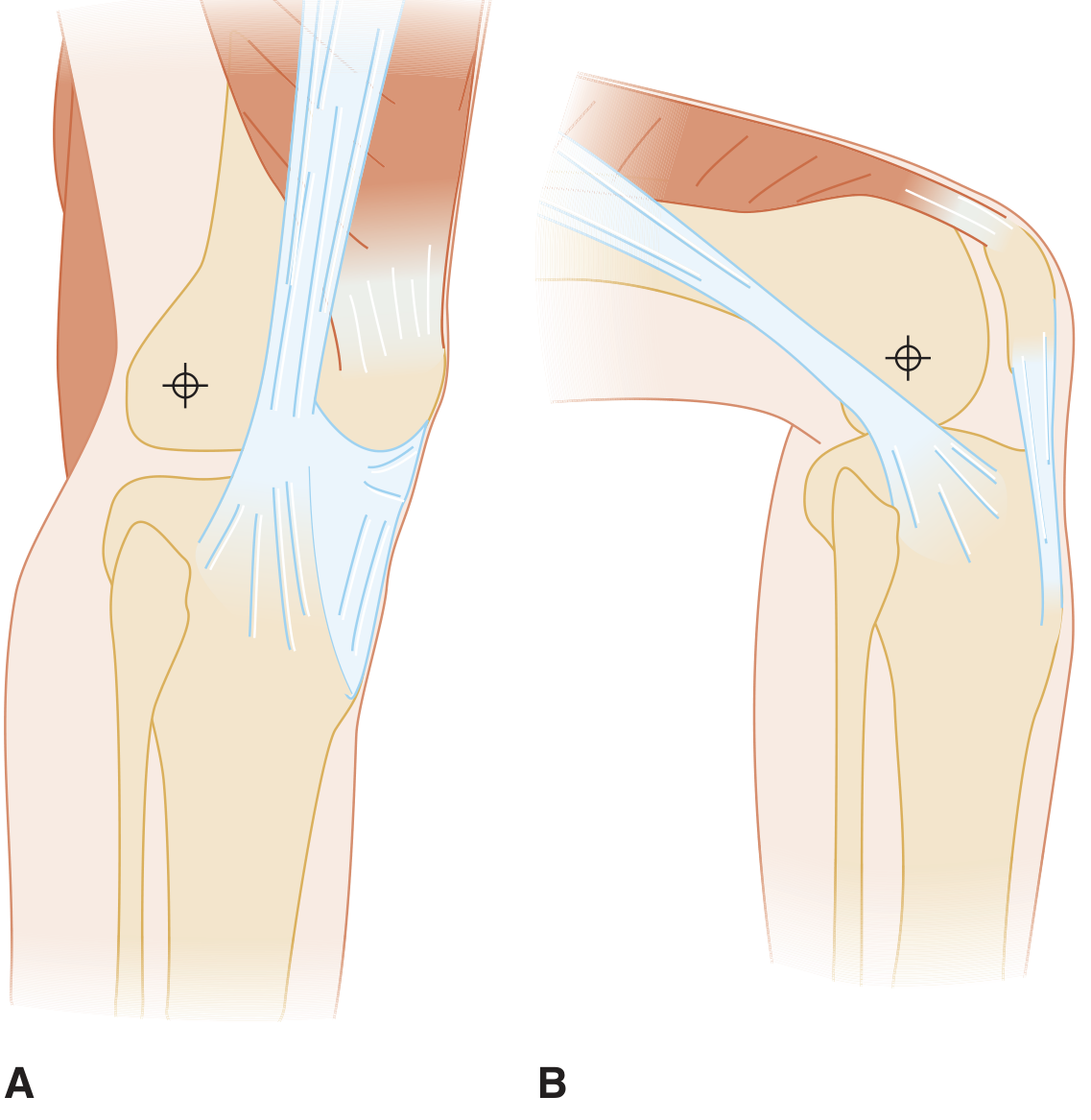
Fig: A. ITB lies anterior to the lateral femoral epicondyle in extension. B. With knee flexion, it slides posterior — repetitive friction causes ITBS. (Tintinalli's Emergency Medicine)
- In extension: ITB lies anterior to the lateral femoral condyle
- At ~30° flexion: ITB snaps posterior over the condyle, causing friction and irritation of the underlying bursa
- Stair climbing, which requires repetitive flexion at this range, is a classic aggravating activity
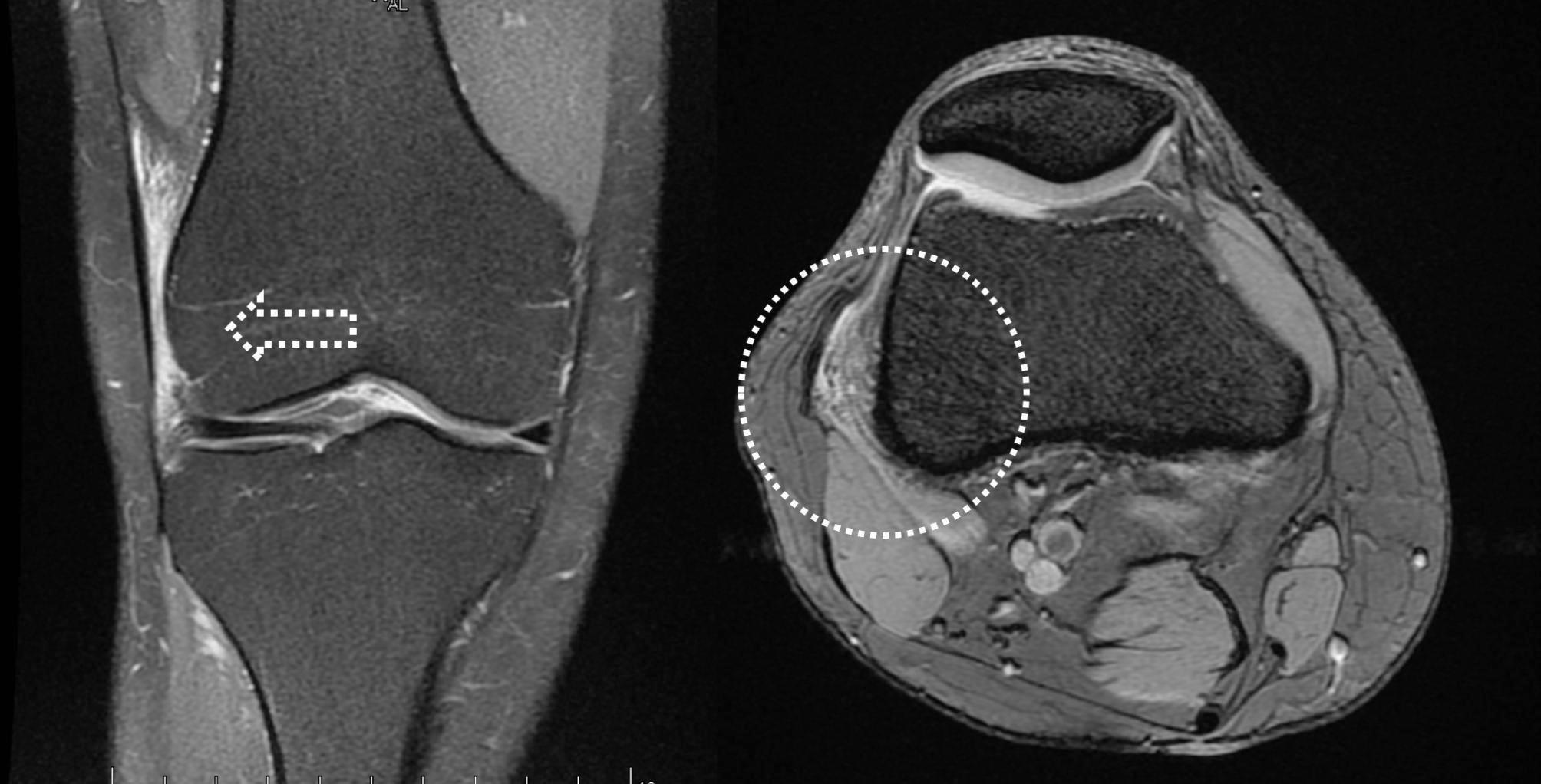
MRI findings in ITBS: T2 fat-suppressed images showing inflammatory edema at the ITB-lateral femoral condyle interface.
Why This Patient is at Risk
Women are anatomically predisposed to ITBS due to (Gray's Anatomy for Students):
- Genu varum — increases ITB tension across the lateral femoral condyle
- Internal tibial rotation — applies additional tension on the band during knee movements
- Age 48 — increased tissue stiffness, reduced recovery capacity
- Activities requiring repeated stair use load the IT band at the critical 20–30° flexion zone
Clinical Features
| Feature | In This Patient |
|---|---|
| Pain site | Below knee (Gerdy's tubercle) → radiates proximally up lateral thigh |
| Aggravating factor | Knee flexion, climbing stairs |
| Character | Aching or burning |
| Tenderness | Point tenderness over lateral femoral condyle |
| Positive test | Ober test (tightness of ITB); Noble compression test (pressure over lateral femoral condyle at 30° flexion reproduces pain) |
Harrison's 22E: "Iliotibial band syndrome most commonly presents with aching or burning pain where the band courses over the lateral femoral condyle of the knee; pain may also radiate up the thigh, toward the hip."
Differential Diagnoses to Consider
| Condition | Distinguishing Features |
|---|---|
| Lateral collateral ligament injury | Traumatic onset, varus stress test positive, instability |
| Popliteus tendinitis | Pain at posterolateral knee, worse running downhill, positive Webb test |
| Common peroneal nerve entrapment | Numbness/tingling along lateral leg, foot drop, positive Tinel's at fibular head |
| Lateral meniscus tear | Joint line tenderness, McMurray test positive, locking/clicking |
| Knee osteoarthritis | Crepitus, joint space narrowing on X-ray, morning stiffness |
| Biceps femoris tendinopathy | Posterolateral pain, tenderness at fibular head |
Investigations
- Clinical diagnosis — thorough physical exam (Ober test, Noble compression test) usually sufficient
- X-ray knee — to exclude OA, bony pathology
- MRI knee — gold standard if diagnosis uncertain; shows T2 hyperintensity at ITB–lateral femoral condyle interface (as seen above)
- Ultrasound — cost-effective; shows thickening of ITB and bursal fluid
Management
Conservative (First Line)
- Activity modification — avoid stair climbing, running, cycling during the acute phase
- Ice — 15–20 minutes after aggravating activities
- NSAIDs — ibuprofen/naproxen for pain and inflammation
- Physical therapy:
- ITB stretching (standing cross-leg stretch, foam rolling)
- Hip abductor and gluteal strengthening (side planks, single-leg bridges, resisted hip abduction)
- Biomechanical correction of genu varum/tibial rotation
Interventional
- Corticosteroid injection — into the point of maximal tenderness over the lateral femoral condyle; running must be avoided for ≥2 weeks post-injection (Harrison's 22E)
Surgical (Rare, Refractory Cases)
- Arthroscopic release/debridement of the ITB at the lateral femoral condyle
- Z-plasty ITB lengthening for refractory cases
Goldman-Cecil Medicine: "For iliotibial band syndrome, treatment focuses on limiting activities that exacerbate pain, icing, and NSAIDs, followed by physical therapy. Corticosteroid injections can be used if needed."
Summary
This 48-year-old woman almost certainly has Iliotibial Band Syndrome. The pain originating at the lateral tibial condyle (below the knee at Gerdy's tubercle), radiating proximally along the lateral limb, aggravated by knee flexion and stair climbing, fits perfectly with ITB friction over the lateral femoral condyle at ~30° flexion. She should be managed conservatively with activity modification, NSAIDs, and a structured physical therapy program targeting ITB flexibility and hip abductor strength.
Sources: Harrison's Principles of Internal Medicine 22E, Tintinalli's Emergency Medicine, Goldman-Cecil Medicine, Gray's Anatomy for Students, Imaging Anatomy Vol. 3
There is no pain in the thigh region
Finding Sources
Finding Sources
Searching the Web
pain below lateral knee radiating down lateral lower leg pain with knee flexion no thigh pain diagnosis
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching Images
common peroneal nerve anatomy fibular head lateral lower leg pain
Loading Image
Thank you for that critical clarification. The absence of thigh pain significantly refines the diagnosis. Here is the updated analysis:
Revised Clinical Assessment: Pain Below Knee → Lateral Lower Leg (No Thigh Pain)
Revised Most Likely Diagnosis: Common Peroneal Nerve Entrapment (Fibular Tunnel Syndrome)
The refined symptom pattern:
- Originates below the knee (at the fibular head / proximal lateral leg)
- Radiates down the lateral aspect of the lower leg only — NOT up into the thigh
- Worsened by knee flexion (flexion compresses the nerve at the fibular head)
- Difficulty climbing stairs (requiring repeated knee flexion)
This is the classic presentation of common peroneal nerve entrapment at the fibular head.
Anatomy of the Common Peroneal Nerve
The common peroneal nerve:
- Branches from the sciatic nerve at the distal femur
- Winds posteriorly and laterally around the fibular head
- Passes under the fibular tunnel (fibular tunnel syndrome)
- Divides into:
- Superficial peroneal nerve → ankle eversion + sensation over anterolateral leg and dorsum of foot
- Deep peroneal nerve → ankle dorsiflexion + toe extension + first web space sensation

Sensory distribution of the common peroneal nerve: lateral shin → dorsum of foot — exactly matching this patient's radiation pattern.
Why Knee Flexion Causes Pain Here
At the fibular head, the common peroneal nerve is:
- Superficial — directly exposed to compression
- Tethered against the fibular neck
- During knee flexion, the nerve is stretched and compressed at this point → pain and/or paraesthesia radiate down the lateral leg in the peroneal distribution
Complete Differential Diagnosis (Revised)
| Diagnosis | Key Features Matching This Patient | Distinguishing Test |
|---|---|---|
| Common peroneal nerve entrapment ⭐ | Pain at/below lateral knee, radiates down lateral leg, worsened by flexion | Tinel's at fibular head; nerve conduction study (NCS) |
| Proximal tibiofibular joint instability | Pain below lateral knee, worsened by flexion and twisting | Instability on stress X-ray; MRI |
| Biceps femoris tendinopathy | Insertion pain at fibular head, worsened with loading | Tenderness localised to fibular head only; no radiation |
| LCL / posterolateral corner injury | Lateral knee pain with varus stress; instability | Varus stress test, MRI |
| Lateral compartment syndrome | Leg tightness, pain after exertion | Compartment pressure measurement |
| Intraneural ganglion (synovial cyst) | Peroneal distribution pain + neurological deficit; from superior tibiofibular joint | MRI — cystic lesion tracking along articular branch |
Localization in Clinical Neurology 8e: "Intraneural ganglia of the peroneal nerve develop from the superior tibiofibular joint when disruption of the capsule allows dissection of synovial fluid along the articular branch of the peroneal nerve — presenting with more pain at the knee or in the peroneal distribution, and a palpable mass at the fibular head."
Key Distinguishing Points from ITB Syndrome
| ITB Syndrome | Peroneal Nerve Entrapment | |
|---|---|---|
| Pain origin | Lateral femoral condyle (over the knee) | Below the knee at fibular head |
| Radiation | UP the thigh ± | DOWN the lateral leg |
| Neurological symptoms | None | May have numbness, tingling on lateral leg |
| Flexion | Painful (band snaps at 30°) | Painful (nerve compressed/stretched) |
| Tinel's sign | Negative | Positive at fibular head |
Clinical Examination
- Tinel's sign at the fibular head — reproduces lateral leg pain/tingling
- Passive knee flexion — reproduces symptoms
- Ober test — negative (distinguishes from ITBS)
- Check for: foot drop, weakness of ankle eversion/dorsiflexion, numbness lateral leg/dorsum foot
Investigations
- Nerve Conduction Study (NCS) + EMG — gold standard; shows slowing/amplitude drop across the fibular head
- MRI knee/proximal fibula — to exclude intraneural ganglion, cyst, or mass from the superior tibiofibular joint
- Ultrasound — can visualise nerve thickening, ganglion cyst
- X-ray — to exclude bony abnormality at fibular head
Harrison's 22E: "Peroneal motor conduction velocity shows slowing and amplitude drop across the fibular head." Bradley and Daroff's Neurology: "Slowed nerve conduction velocity across region of entrapment, usually at fibular neck. EMG may show denervation in peroneal-innervated muscles."
Management
Conservative
- Avoid leg crossing and prolonged knee flexion
- NSAIDs for pain
- Knee pad over lateral knee to reduce compression
- Physiotherapy — avoid positions that compress the nerve, stretching
- Weight loss if applicable (reduces nerve compression)
Interventional
- Corticosteroid injection at the fibular tunnel
Surgical
- Neurolysis / decompression of the fibular tunnel
- Excision of ganglion cyst if intraneural ganglion is identified on MRI
- Most cases spontaneously resolve over weeks to months with conservative care (Harrison's 22E)
Bottom Line
With pain starting below the knee radiating down (not up) the lateral leg, aggravated by knee flexion and stair climbing, the leading diagnosis is common peroneal nerve entrapment at the fibular head. The next critical step is NCS/EMG to confirm and localise the lesion, paired with MRI to exclude a compressive structural cause (ganglion cyst from the superior tibiofibular joint being the most important treatable lesion to identify).
Sources: Harrison's Principles of Internal Medicine 22E, Localization in Clinical Neurology 8e, Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.