Seasmoid fracture etiology mechanism of injury associated injury signs and symptoms and investigations and evaluation treatment explain in detail with appropriate illustrative diagrams and images
Reading File
Finding Sources
Finding Sources
Searching the Web
sesamoid fracture etiology mechanism injury associated injuries signs symptoms treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Finding Sources
Searching PubMed
sesamoid fracture treatment outcome
I now have rich textbook content and multiple high-quality images. Let me compile the comprehensive answer.
Sesamoid Fracture - Comprehensive Review
1. Anatomy and Background
Sesamoid bones are small, ovoid bones embedded within tendons that pass over bony prominences. In the foot, the two hallucal sesamoids (tibial/medial and fibular/lateral) sit within the two heads of the flexor hallucis brevis (FHB) tendon on the plantar surface of the first metatarsal head. They are analogous to the patella in function - increasing the mechanical advantage (fulcrum effect) of the FHB by approximately 50%, which is critical during push-off in gait.
Key anatomy:
- The tibial (medial) sesamoid is larger, sits more directly beneath the first metatarsal head, and is the more commonly injured of the two
- The fibular (lateral) sesamoid is smaller and rarely bipartite
- Both bones are contained within a fibrocartilaginous plantar plate complex, along with the flexor tendon sheath and intersesamoid ligament
- They bear 300-400% of body weight during push-off activities
- Blood supply enters from the plantar aspect, making avascular necrosis a known complication of injury
2. Etiology and Predisposing Factors
Sesamoid fractures can be acute (traumatic) or chronic (stress/fatigue). They account for approximately 9% of all ankle-foot complex injuries.
Acute Fractures
- Falls from height with axial loading on the forefoot
- Direct trauma to the plantar foot
- Sudden, forceful push-off
Stress (Fatigue) Fractures
- Long-distance running, ballet dancing (especially the demi-pointe/relevé position)
- Soccer, basketball, tennis
- Military recruits (repetitive marching)
- Rapid escalation of training load
Risk Factors
| Factor | Mechanism |
|---|---|
| High-arched foot (pes cavus) | Increased pressure concentration under 1st metatarsal head |
| Prominent first metatarsal head | Direct plantar pressure |
| Hypermobile first ray | Altered sesamoid mechanics |
| High-heeled footwear | Forced forefoot loading |
| Female gender | Hormonal factors, lower bone density |
| Osteoporosis/low bone density | Reduced resistance to fatigue loading |
| Previous turf toe or hallux rigidus | Altered biomechanics at 1st MTP joint |
| Excessive foot pronation | Abnormal loading distribution |
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 5221-5222
- Rockwood and Green's Fractures in Adults 10th Ed 2025, p. 868
3. Mechanism of Injury
Two distinct biomechanical mechanisms apply:
Direct Mechanism (Axial Loading)
A direct compressive force is applied to the sesamoid - e.g., landing hard on the ball of the foot after a jump. This typically produces a comminuted, multifragmented fracture pattern. The energy is transmitted vertically through the metatarsal head onto the sesamoid against the hard ground.
Indirect Mechanism (Hyperextension)
Violent hyperextension/dorsiflexion of the first metatarsophalangeal (MTP) joint causes a traction/tensile force through the FHB tendon, avulsing or fracturing the sesamoid. This is most commonly seen in football and soccer players - e.g., a player's toe being dorsiflexed while planted on a firm surface (the classic "turf toe" force vector).
DIRECT MECHANISM:
Ground → Sesamoid ← First Metatarsal Head
(Axial compression → comminuted fracture)
INDIRECT MECHANISM (Hyperextension):
FHB tension → Sesamoid → avulsion/transverse fracture
(e.g., foot planted, body moves forward = forced dorsiflexion)
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 5222
4. Associated Injuries
Sesamoid fractures frequently occur alongside or as part of a spectrum of first MTP joint injuries:
| Associated Injury | Relationship |
|---|---|
| Turf toe | Hyperextension injury to the plantar plate complex; sesamoid fracture may be part of the grade 3 injury |
| MTP joint dislocation | High-energy sesamoid fractures often occur with MTP dislocation or subluxation |
| Plantar plate tear | Disruption of the capsuloligamentous complex plantar to the 1st MTP joint |
| Flexor hallucis brevis injury | Musculotendinous unit disruption with wide sesamoid displacement |
| Hallux valgus | Acute traumatic hallux valgus involving the medial capsule and medial sesamoid |
| Intersesamoid ligament disruption | Separation of the two sesamoids; affects stability |
| Avascular necrosis (AVN) | Complication of any sesamoid injury due to disruption of plantar blood supply |
Turf Toe Grading (Anderson Classification):
| Grade | Pathology | Signs | Treatment |
|---|---|---|---|
| 1 | Capsular strain | Normal ROM, full weight-bearing, normal X-rays | Stiff insole, taping; immediate return to play |
| 2 | Partial capsular tear | Painful ROM, limited weight-bearing, normal X-rays | No athletics 2 weeks; stiff insole |
| 3 | Complete plantar plate tear | Severe pain, limited/painful ROM, abnormal X-rays (fracture or proximal sesamoid migration) | Operative repair of plantar plate |
- Miller's Review of Orthopaedics 9th Ed, p. 564
5. Signs and Symptoms
Acute Fracture
- Immediate, sharp, localized pain on the plantar aspect of the first metatarsal head (ball of foot)
- Point tenderness directly over the involved sesamoid (tibial or fibular)
- Swelling and ecchymosis/bruising plantar to the first MTP joint
- Antalgic gait - shortened stance phase on the affected foot
- Patient descends stairs with injured foot leading (to avoid push-off)
- Limited extension of the great toe (hallux)
- Pain on passive dorsiflexion of the great toe
Stress Fracture (Insidious Onset)
- Gradual onset of pain beneath the great toe with activity
- Initially pain only with vigorous activity; progresses to pain with walking
- Tenderness localized to the sesamoid (may need careful palpation to distinguish from diffuse MTP tenderness)
- Minimal swelling, usually no ecchymosis
- Pain relief with rest early in the course
Physical Examination Findings
- Diffuse MTP joint tenderness initially; careful palpation isolates to one sesamoid
- Plantar palpation test: direct pressure over the individual sesamoid reproduces pain
- Hyperextension test (dorsiflexion stress test): passive dorsiflexion of the hallux reproduces pain (stresses both FHB and sesamoid)
- Compare range of motion bilaterally
- Assess for hallux valgus or varus deformity
6. Investigations and Evaluation
6.1 Plain Radiographs (First-Line)
Multiple views are required:
| View | Purpose |
|---|---|
| Weight-bearing AP (bilateral comparison) | Compare both sesamoids; identify fracture or bipartite sesamoid |
| Lateral (foot in slight pronation) | Profiles sesamoids; shows displacement |
| Medial oblique (sesamoid view) | Best view for the tibial sesamoid |
| Lateral oblique view | Best view for the fibular sesamoid |
| Axial sesamoid view | Shows sclerosis, joint space narrowing, osteochondritis |
Bilateral standing AP is the most important comparison view, as bipartite sesamoids are present in ~10-14% of the population (bilateral in 25% of those).
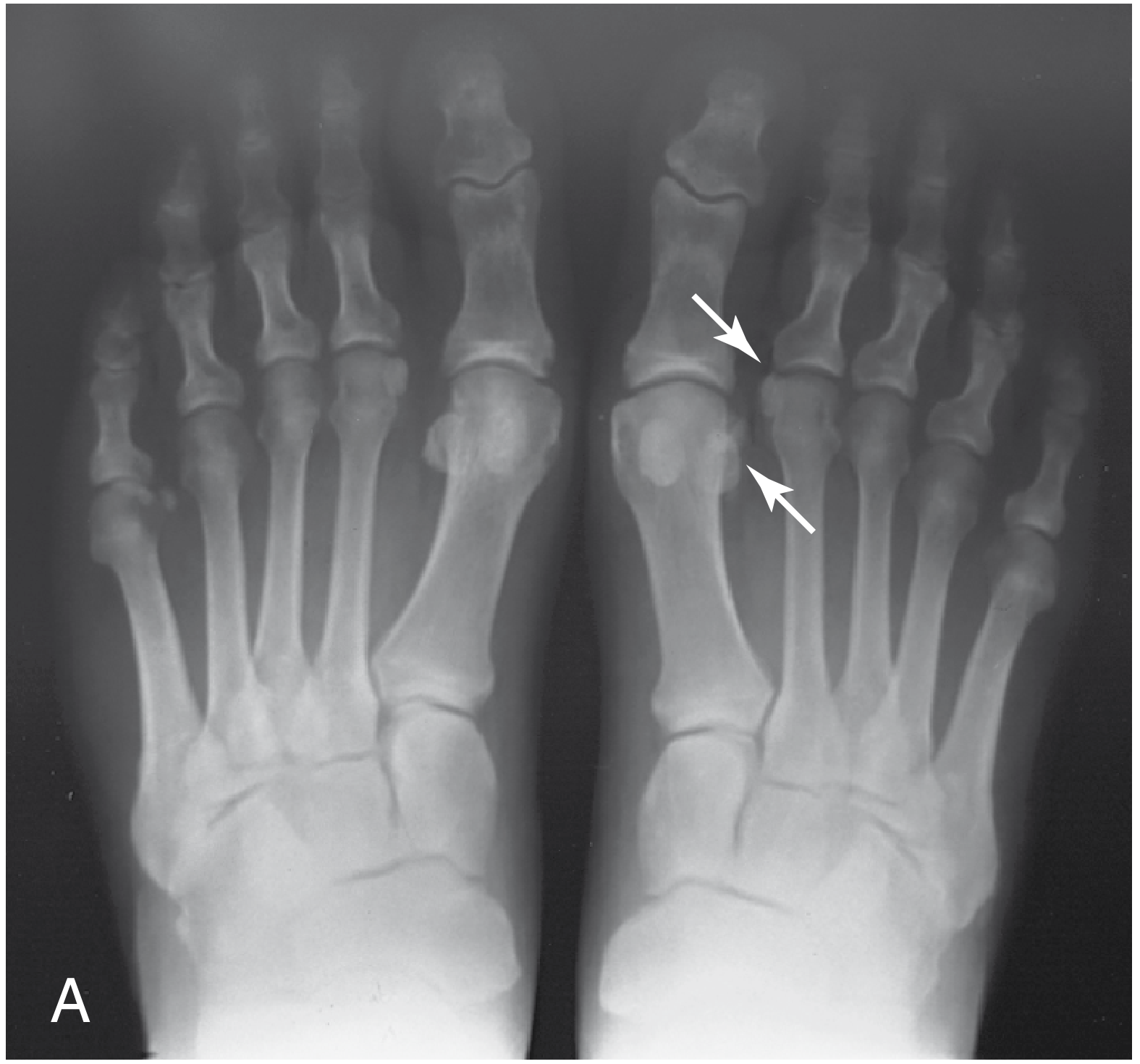
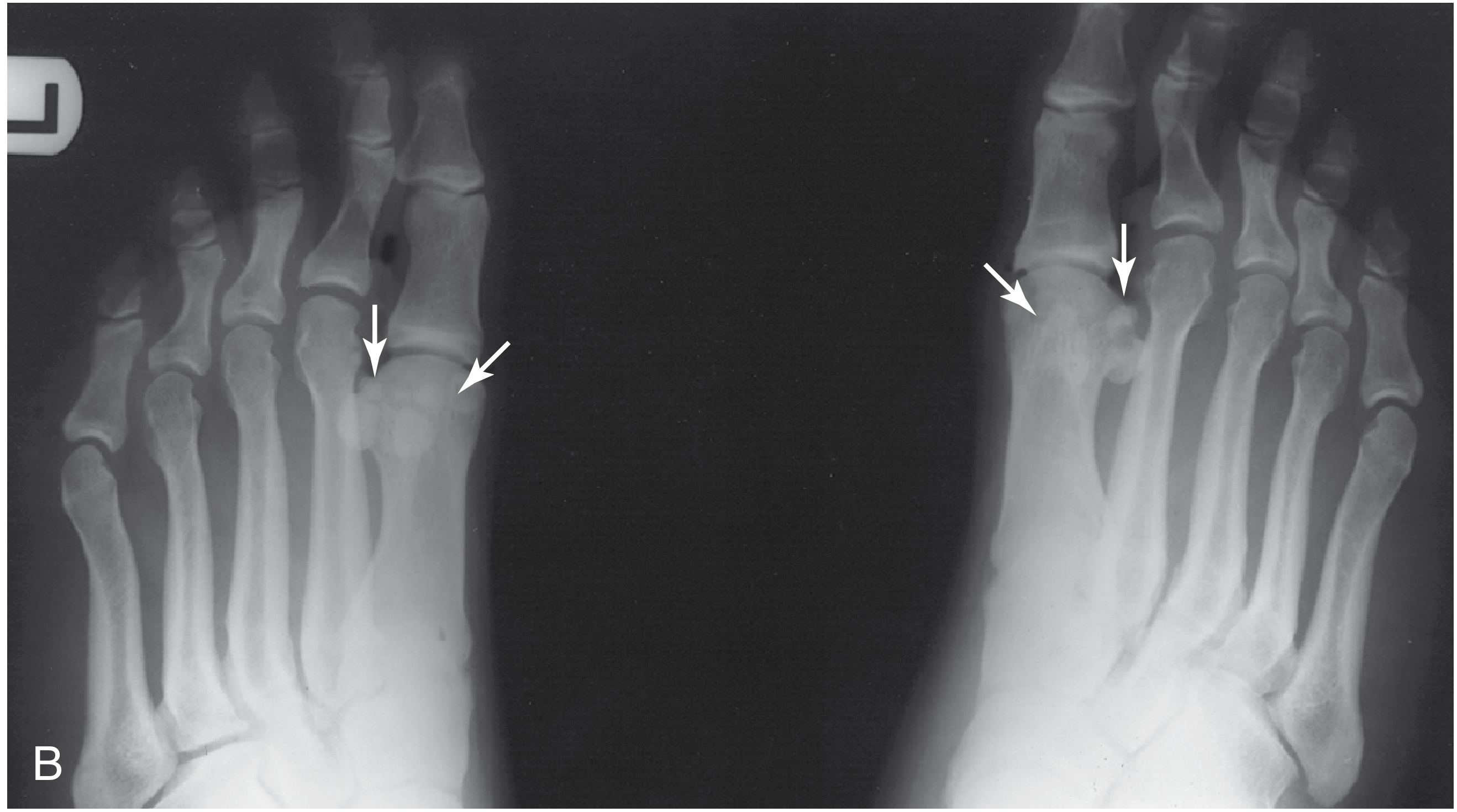
Distinguishing Fracture from Bipartite Sesamoid
This is the most common diagnostic challenge:
| Feature | Fracture | Bipartite Sesamoid |
|---|---|---|
| Fragment edge morphology | Irregular, jagged | Smooth, rounded |
| Fragment sizes | Roughly equal halves | One larger + one smaller fragment |
| Laterality | Usually unilateral | Often bilateral (25%) |
| Overall size | Same size or slightly larger than contralateral | Larger than a single sesamoid |
| Clinical history | Acute trauma or overuse | Often incidental/asymptomatic |
| Contralateral foot | Normal singular sesamoid | May be bipartite bilaterally |
Note: A singular sesamoid on the contralateral foot does NOT absolutely confirm a fracture, as symptomatic synchondrosis of a bipartite sesamoid can present similarly.
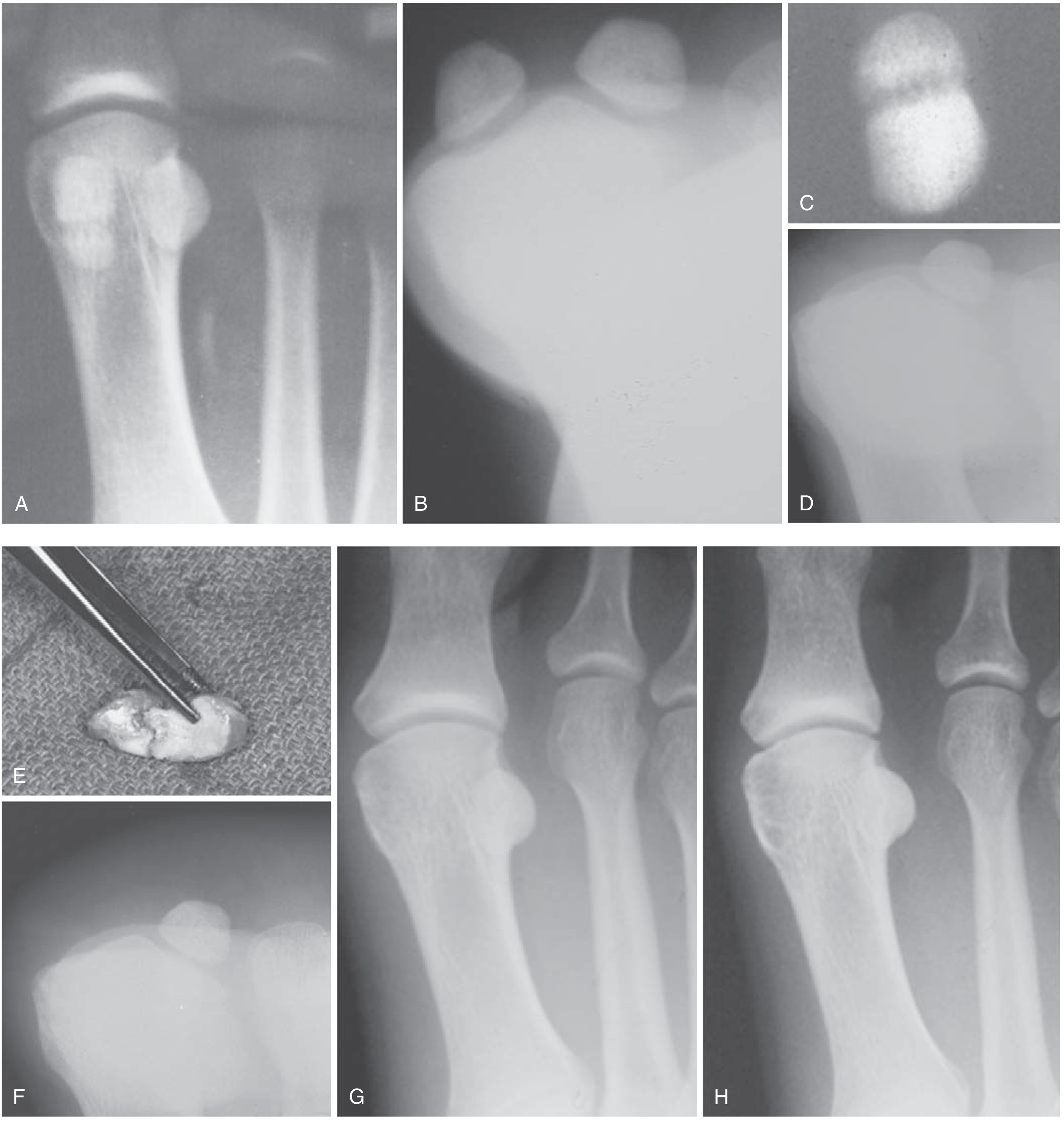
6.2 CT Scan
- Best modality to fully characterize fracture pattern (comminution, displacement, fragment number)
- Guides surgical planning for ORIF vs. sesamoidectomy
- Useful when plain X-rays are equivocal
6.3 MRI
- Best for soft tissue assessment: plantar plate integrity, FHB tendon, intersesamoid ligament
- Depicts avascular necrosis, stress fracture, osteochondritis dissecans, osteonecrosis
- Particularly useful when fibular sesamoid fracture is suspected (fibular sesamoid is rarely bipartite, so if clinical suspicion is high, MRI confirms fracture)
- Best for evaluating associated turf toe soft tissue injuries
6.4 Radionuclide Bone Scan
- Can confirm diagnosis of stress fracture with increased uptake
- However, use with caution: 26-29% of asymptomatic individuals show increased bone scan activity in the sesamoid region
- Largely superseded by MRI in clinical practice
6.5 Diagnostic Algorithm
Plantar 1st MTP pain
|
Weight-bearing X-rays (AP, lateral, oblique, axial)
|
┌───┴───┐
Fracture Bipartite?
confirmed |
| Compare: fragment edges, sizes, bilaterality
| |
| Still unclear?
| |
| MRI / CT scan
|
Assess displacement
|
┌─────┴─────┐
Non/minimally Displaced
displaced (>5 mm) or MTP
| dislocation
Conservative Surgical evaluation
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 4821-4822
- Roberts and Hedges' Clinical Procedures in Emergency, p. 1213
7. Treatment
Treatment depends on fracture type (acute vs. stress), degree of displacement, and whether associated injuries are present.
7.1 Conservative (Non-Operative) Treatment
Indications: Nondisplaced or minimally displaced fractures; stress fractures; most acute fractures without MTP dislocation.
Step-by-step approach:
Phase 1 - Acute immobilization (0-6 weeks):
- Short leg walking cast incorporating a toe plate, or a fracture boot to limit stress across the sesamoid - for 3 to 4 weeks initially
- Non-weight-bearing or protected weight-bearing with crutches
- NSAIDs for pain and inflammation
- Ice application to the plantar foot
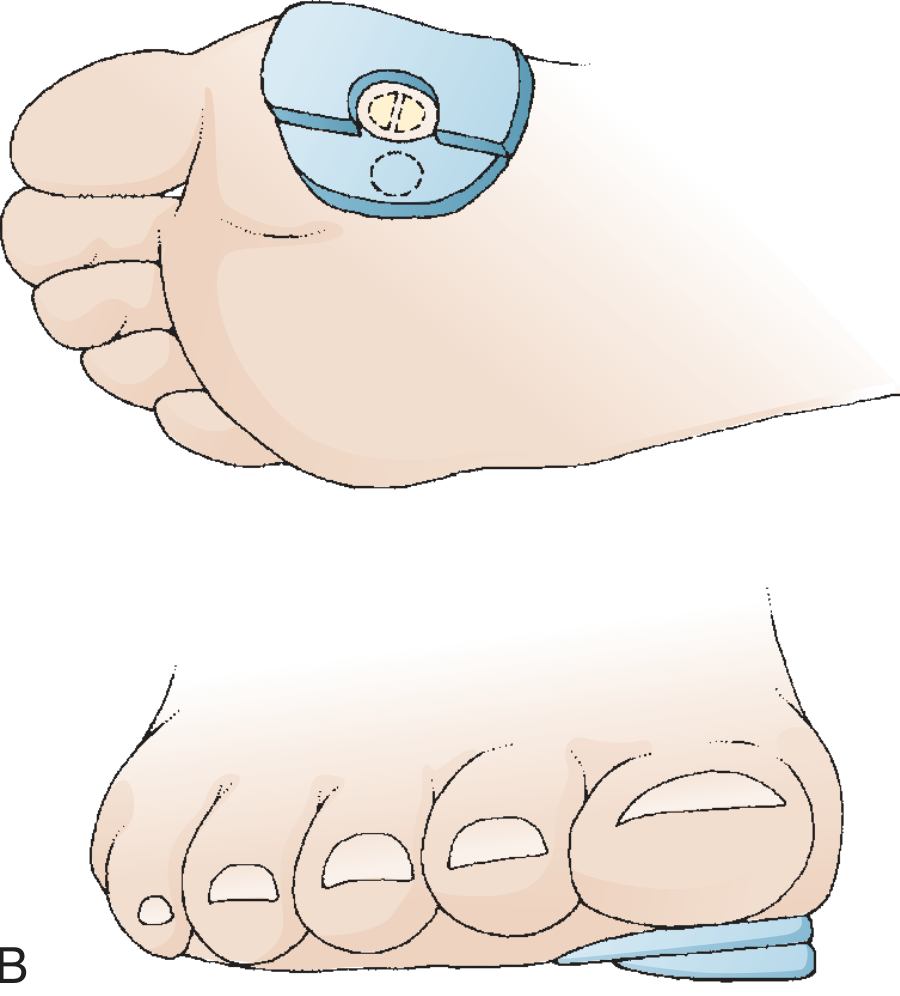
Phase 2 - Protected mobilization (6-12 weeks):
- Transition to a stiff-soled shoe or rigid carbon fiber insole
- Dancer's pad (sesamoid relief orthotic): a full-length orthotic with a cutout or relief beneath the sesamoid to offload pressure; weight-bearing redistributed to surrounding metatarsals
- A bunion-type aperture pad (hole placed over the sesamoid, felt reinforced medially) achieves the same goal for tibial sesamoid injuries
- Gradual resumption of activity
Phase 3 - Return to activity:
- Full-length rigid carbon plate + orthotic with dancer's pad inside athletic shoe
- Gradual reconditioning: pool running → cycling → land running
- Athletes: cardiovascular fitness maintained during healing
Note on radiographic follow-up: Subsequent X-rays rarely show bony consolidation in sesamoid fractures, but the fracture interface progressively appears smoother - do not judge healing by radiographs alone.
7.2 Operative Treatment
Indications for Surgery:
- Displaced fracture (>5 mm) - especially with MTP dislocation or subluxation
- Widely displaced fracture with disruption of FHB musculotendinous unit
- Symptomatic nonunion after adequate conservative management (typically 6 months)
- Comminuted fracture with loss of articular cartilage
- Cases refractory to conservative care
Surgical Options:
A. Open Reduction and Internal Fixation (ORIF)
- For fragments of roughly equal size with significant displacement (>5 mm)
- Mini-fragment screw fixation (most common)
- Figure-of-8 wire loop around proximal and distal poles over the sesamoid
- Bone grafting from the calcaneus or supramalleolar distal tibia may be added to achieve union
- Repair of the FHB mechanism is mandatory regardless of fixation method chosen


B. Sesamoidectomy (Partial or Complete)
- Partial sesamoidectomy (pole excision): excision of proximal or distal pole - preferred when the fracture pattern allows; achieves best results
- Complete sesamoidectomy: for comminuted fractures with no large fragments, loss of articular cartilage on sesamoid or on the overlying metatarsal head surface
- A 6-month (lengthy) trial of conservative treatment should precede sesamoidectomy in non-athletes
- May be performed earlier in athletically active patients seeking faster return to sport
Sesamoidectomy Technique (Technique 93.18 - Campbell's):
- Medial longitudinal incision, plantar to midline; capsule incised longitudinally
- Evaluate tibial sesamoid cartilage quality and fragment mobility intraoperatively
- Inspect plantar surface of metatarsal head for cartilage damage
- Extracapsular approach; protect the proper medial plantar nerve to the hallux (emerges plantarly at the abductor hallucis musculotendinous junction - retract plantarly)
- Perform complete or partial sesamoidectomy
- Repair the FHB defect with 2-0 nonabsorbable polyethylene suture; use suture anchor for partial excision
7.3 Outcomes
| Treatment | Outcome |
|---|---|
| Conservative - stress fractures | Most heal with 6-12 weeks immobilization + orthotic |
| Sesamoidectomy in athletes | Return to sport at mean 7.5 weeks |
| Sesamoidectomy in non-athletes | Return to activity at ~12 weeks |
| 90% of tibial sesamoidectomies | Return to preoperative activity level |
Complications of sesamoidectomy:
-
Hallux valgus deformity after tibial sesamoidectomy (if soft tissue repair is inadequate)
-
Hallux varus deformity after fibular sesamoidectomy
-
Postoperative scarring / neuroma-like symptoms after fibular sesamoidectomy
-
Cock-up toe deformity if both sesamoids are excised
-
Inability to stand on tiptoes (does not typically affect ADLs)
-
Campbell's Operative Orthopaedics 15th Ed 2026, p. 5222-5223
-
Miller's Review of Orthopaedics 9th Ed, p. 565
8. Summary Diagram
SESAMOID FRACTURE - CLINICAL PATHWAY
ETIOLOGY
├── Direct: axial load (fall, jump) → comminuted fracture
└── Indirect: FHB traction / MTP hyperextension → transverse fracture
RISK FACTORS
├── High-arched foot, prominent 1st MT head
├── Athletes: dancers, runners, footballers
└── Female, osteoporosis, high heels
ASSOCIATED INJURIES
├── Turf toe (Grade 1/2/3)
├── MTP dislocation
├── Plantar plate tear
└── AVN of sesamoid
SIGNS & SYMPTOMS
├── Plantar 1st MTP pain (immediate in acute fracture)
├── Point tenderness over involved sesamoid
├── Swelling ± ecchymosis
├── Limited / painful great toe dorsiflexion
└── Shortened stance phase, toe-lead on stairs
INVESTIGATIONS
├── X-rays (AP bilateral, oblique, axial) - FIRST
├── CT - fracture characterization
└── MRI - soft tissue, AVN, stress fracture
TREATMENT
├── Conservative (nondisplaced / stress fractures)
│ ├── Cast/boot 3-6 weeks + toe plate
│ ├── NSAIDs, ice
│ └── Dancer's pad orthotic + gradual RTA
└── Operative (displaced >5mm, nonunion, comminuted)
├── ORIF (mini-screw / figure-8 wire + bone graft)
└── Sesamoidectomy (partial pole or complete)
+ FHB repair (mandatory)
References (Authoritative Textbooks):
- Campbell's Operative Orthopaedics 15th Ed 2026, pp. 4821-4823, 5221-5223
- Rockwood and Green's Fractures in Adults 10th Ed 2025, p. 868
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, pp. 1213-1214
- Miller's Review of Orthopaedics 9th Ed, pp. 564-565
- Imaging Anatomy Text and Atlas Vol. 3
This is a shared conversation. Sign in to Orris to start your own chat.