Explain me sleep physiology with diagram for my university exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have everything I need - rich textbook content and four excellent diagrams. Let me compose the comprehensive answer.
Sleep Physiology - Complete University Exam Guide
Sources: Harrison's Principles of Internal Medicine 22E (2025), Adams and Victor's Principles of Neurology 12E, Bradley and Daroff's Neurology in Clinical Practice
1. Introduction & Measurement
Sleep is a reversible, periodically recurring state of reduced consciousness, responsiveness, and motor activity. Most adults require 7-9 hours per night. Sleep is studied using polysomnography (PSG), which continuously records three parameters:
| Parameter | What it measures |
|---|---|
| EEG (electroencephalogram) | Brain electrical activity / cortical rhythm |
| EOG (electrooculogram) | Eye movement activity |
| EMG (electromyogram) | Chin + limb muscle tone |
2. Sleep Stages (AASM 2007 Classification)
PSG defines two fundamental sleep states: NREM and REM sleep.
Stage W - Wakefulness
- EEG: Alpha waves (8-13 Hz) when eyes closed; desynchronized low-voltage when eyes open
- EMG: High muscle tone
- EOG: Normal waking eye movements
NREM Sleep (75-80% of total sleep time)
NREM is subdivided into three stages based on EEG:
Stage N1 (3-8% of total sleep)
- Transition from wake to sleep
- EEG: Alpha waves diminish (<50% of epoch); replaced by theta waves (4-7 Hz) and beta waves
- EOG: Slow, rolling eye movements
- EMG: Slightly reduced
- Vertex sharp waves appear toward end of N1
Stage N2 (50-60% of total sleep)
- "Light sleep" - lasts ~30-60 min per cycle
- EEG hallmarks: Sleep spindles (12-18 Hz, typically 14 Hz) and K complexes (biphasic high-amplitude sharp slow-wave complexes)
- EOG: Minimal eye movements
- EMG: Normally active
Stage N3 - Slow Wave Sleep / Deep Sleep (15-25% in young adults)
- "Deep sleep" - highest arousal threshold
- EEG: Delta waves (0.5-2 Hz, >75 µV) occupy >20% of epoch
- Predominates in the first third of the night
- Growth hormone secretion peaks during this stage
- Most important for physical restoration
Polysomnographic recordings showing EEG patterns across wake and NREM stages:
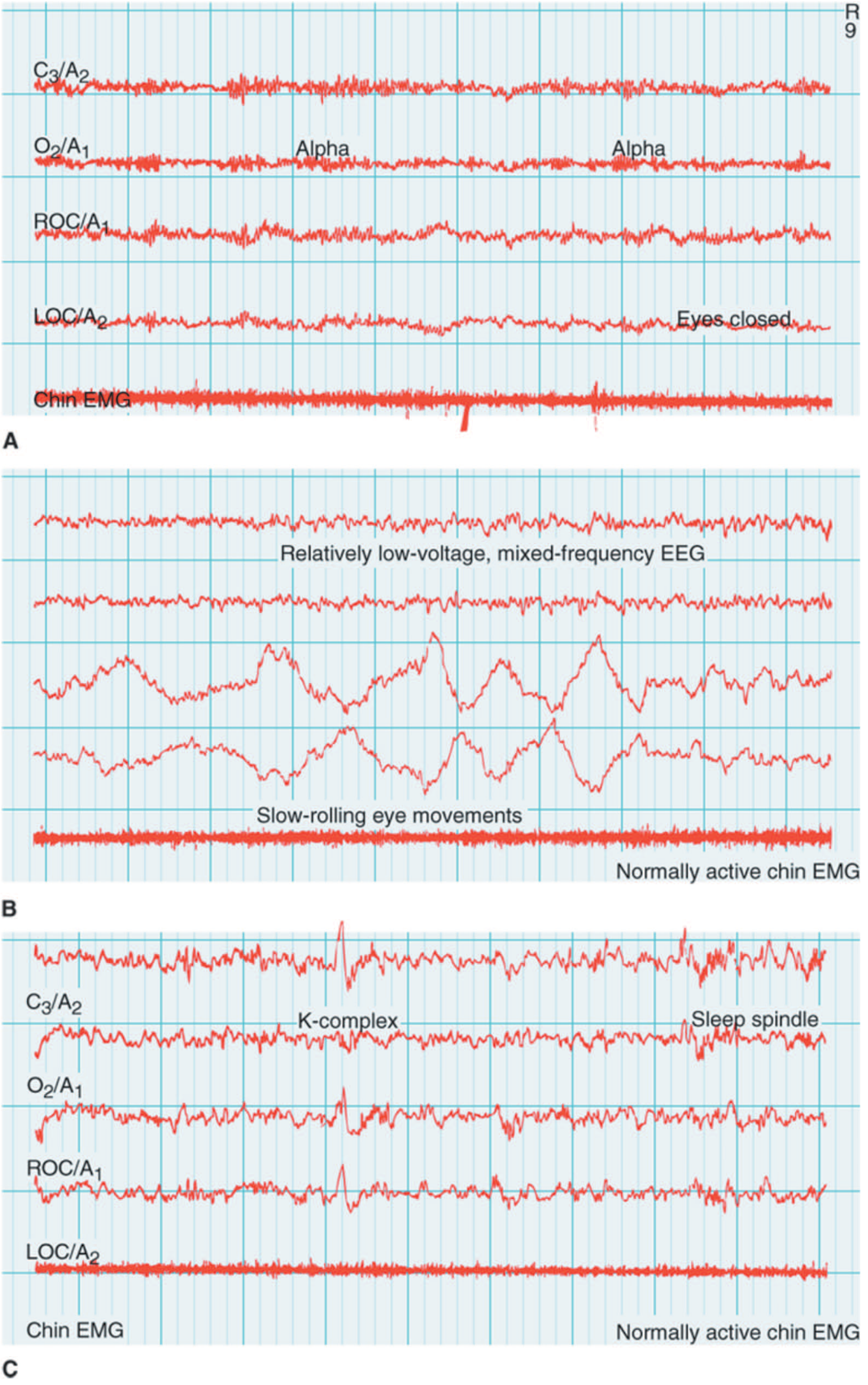
Panel A = Awake (alpha waves, active EMG); Panel B = N1 (slow rolling eye movements, reduced alpha); Panel C = N2 (K-complex + sleep spindle clearly labeled)
REM Sleep (20-25% of total sleep)
Also called paradoxical sleep or fast-wave sleep:
- EEG: Low-amplitude, mixed-frequency, desynchronized - paradoxically similar to wakefulness
- EOG: Rapid eye movements in bursts/flurries
- EMG: Atonia - nearly complete muscle paralysis (except respiratory muscles and extraocular muscles)
- Dreams occur predominantly during REM
- Autonomic instability: variable heart rate, blood pressure, and breathing pattern
- REM cycles lengthen as the night progresses - last REM episode can last ~1 hour
Key paradox of REM: The brain is highly active (EEG resembles wakefulness) but the body is paralyzed.
3. Sleep Architecture (The Hypnogram)
A hypnogram is a graphical representation of sleep stages over the night. Key features:
- After sleep onset, progression is N1 → N2 → N3 within 45-60 minutes
- First REM episode occurs ~90-100 minutes after sleep onset
- NREM-REM cycles repeat every ~90-100 min (4-6 cycles per night)
- Early night: dominated by slow-wave sleep (N3)
- Late night: dominated by longer REM episodes
- After sleep deprivation, NREM recovers first, then REM
Sleep hypnogram comparing architecture across age groups:
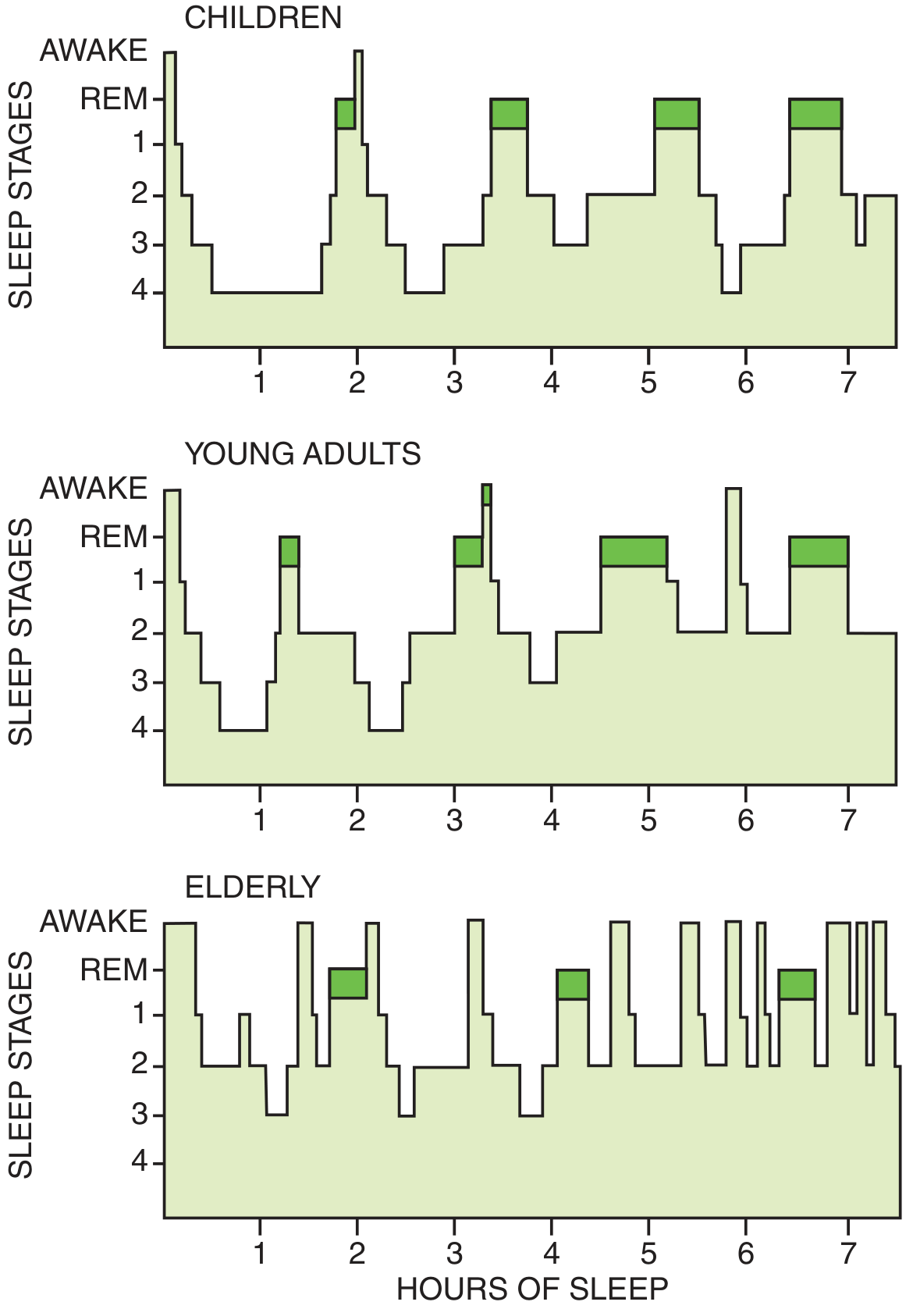
Note: Children have abundant deep sleep (stages 3-4). Young adults show classic architecture. Elderly show fragmented sleep with loss of N3 and more awakenings.
Age-related changes in sleep:
| Parameter | Infants | Young Adults | Elderly |
|---|---|---|---|
| Total sleep | 16-20 h | 7-8 h | ~6.5 h |
| REM % | ~50% | 20-25% | Reduced |
| N3 sleep | Prominent | 15-25% | Often absent |
| Sleep fragmentation | Polyphasic | Minimal | Increased |
4. Neural Control of Sleep and Wakefulness
The Flip-Flop Switch Model
Two opposing systems govern sleep-wake transitions:
Ascending Arousal System (promotes WAKEFULNESS)
Clusters of neurons extending from the upper pons to hypothalamus and basal forebrain that activate the cortex, thalamus, and forebrain using:
- Norepinephrine (locus coeruleus)
- Serotonin (raphe nuclei)
- Histamine (tuberomammillary nucleus)
- Acetylcholine (pedunculopontine and laterodorsal tegmental nuclei)
- Dopamine (ventral periaqueductal grey)
- Glutamate
- GABA (basal forebrain - inhibits cortical inhibitory interneurons, paradoxically promoting arousal)
Orexin (Hypocretin) System
- Neurons in the lateral hypothalamus
- Use the peptide orexin (hypocretin) to reinforce and stabilize arousal by activating other arousal-promoting cell groups
- Loss of orexin neurons causes narcolepsy
Sleep-Promoting System
- GABAergic neurons in the ventrolateral preoptic nucleus (VLPO) and pons
- GABA inhibits all components of the arousal system, allowing sleep to occur
- Additional melanin-concentrating hormone (MCH) neurons in lateral hypothalamus promote REM sleep
These two systems engage in mutual inhibition - like an electrical "flip-flop switch" - producing rapid, stable transitions between wake and sleep, avoiding prolonged intermediate states.
Brain circuit diagram - arousal system vs. sleep-promoting system:
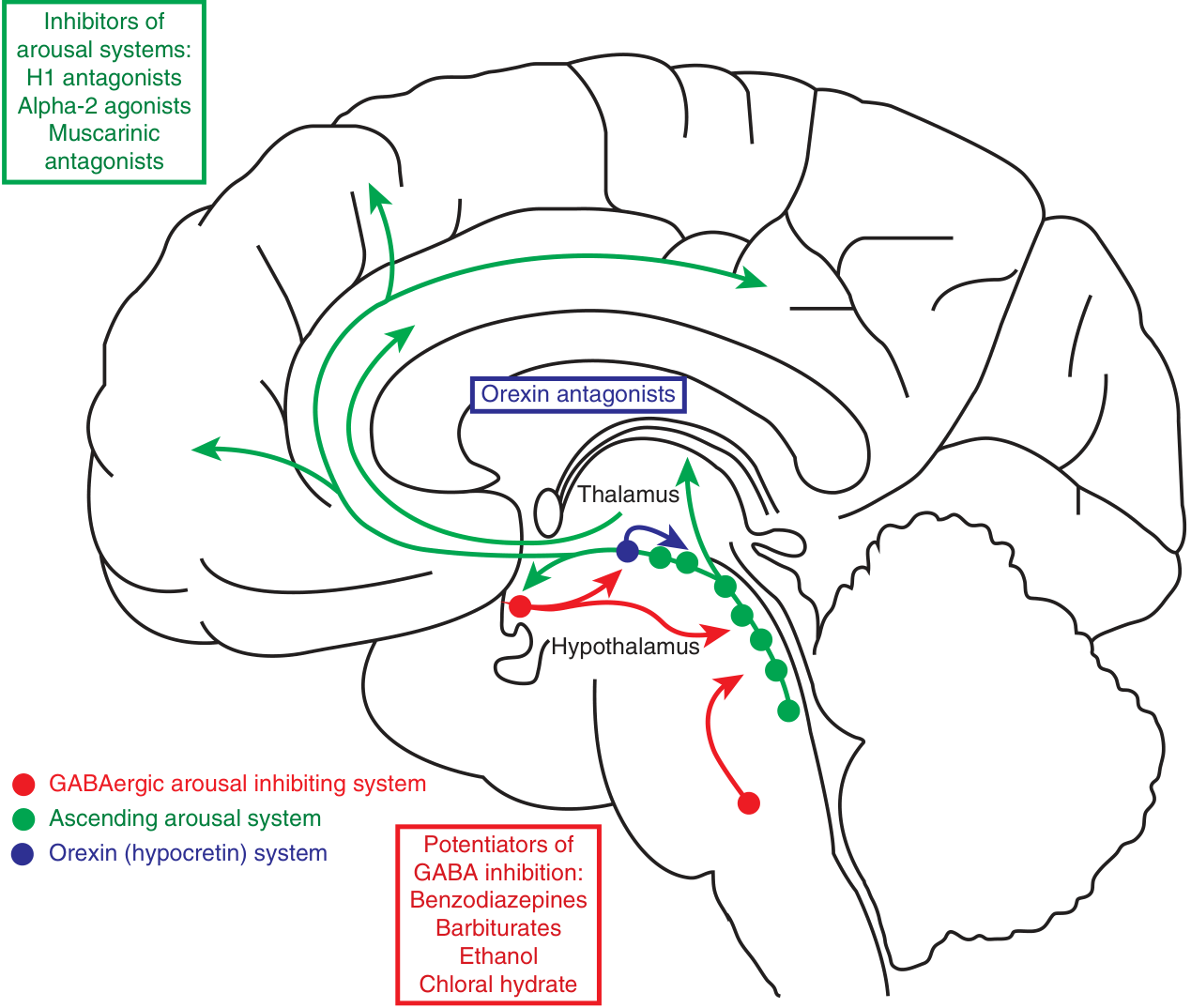
Green = Ascending arousal system (monoaminergic + cholinergic) | Blue = Orexin system (stabilizes arousal) | Red = GABAergic sleep-promoting system (VLPO)
REM Sleep Switch
A separate brainstem flip-flop switch governs NREM-REM transitions:
- REM-Off neurons (lower midbrain, GABAergic) inhibit REM
- REM-On neurons (upper pons): GABAergic (inhibit REM-Off) + glutamatergic (produce REM phenomena)
- REM-On neurons projecting to medulla/spinal cord activate GABA/glycine interneurons → hyperpolarize motor neurons → REM atonia
- REM-On neurons projecting to forebrain → dreams
- Cholinergic input favors REM; monoaminergic (NE + 5-HT) input prevents REM
- Damage to REM atonia neurons → REM Sleep Behavior Disorder
5. Regulation of Sleep - Two-Process Model
Sleep-wake timing is governed by three interacting processes:
Process S - Homeostatic Sleep Drive
- Sleep pressure builds with prolonged wakefulness
- Mediator: Adenosine accumulates during wakefulness
- Acts on A1 receptors to directly inhibit arousal regions
- Acts on A2a receptors to activate VLPO (sleep neurons)
- Caffeine works by blocking A2a receptors (blocking sleepiness)
- Other mediators: Prostaglandin D2
- After sleep deprivation, N3 recovers first ("slow-wave sleep rebound")
Process C - Circadian Drive
- Controlled by the suprachiasmatic nuclei (SCN) of the hypothalamus
- Intrinsic period: ~25 hours, entrained to 24-h cycle by light (via retinohypothalamic tract)
- SCN lesions cause complete disorganization of sleep-wake cycles
- SCN regulates melatonin secretion by the pineal gland (darkness → melatonin rise → promotes sleep onset)
Process A - Allostatic (Stress) Inputs
- Psychological stress, anxiety, and psychiatric disorders activate the ascending arousal system
- Chronic insomnia involves hyperactivation of arousal pathways
- Common cause of insomnia in anxiety disorders
6. Neurotransmitter Summary Table
| Neurotransmitter | During Wake | During NREM | During REM |
|---|---|---|---|
| Acetylcholine | ↑ | ↓ | ↑ (high) |
| Norepinephrine | ↑ | ↓ | ↓↓ (silent) |
| Serotonin | ↑ | ↓ | ↓↓ (silent) |
| Histamine | ↑ | ↓ | ↓↓ |
| Orexin/Hypocretin | ↑ | ↓ | ↓↓ |
| Dopamine | ↑ | ~ | ~ (minimal change) |
| GABA (VLPO) | ↓ | ↑ | ↑ |
| Adenosine | Accumulates | ↓ | ↓ |
Source: Bradley and Daroff's Neurology in Clinical Practice
7. Physiological Changes During Sleep
| System | NREM | REM |
|---|---|---|
| Muscle tone | Mildly reduced | Atonia (paralysis) |
| Heart rate | Regular, slowed | Variable, irregular |
| Blood pressure | Reduced | Variable |
| Breathing | Regular | Irregular |
| Temperature regulation | Maintained | Impaired (poikilothermy) |
| Growth hormone | Peak secretion (N3) | Minimal |
| Penile/clitoral tumescence | Absent | Present |
| Dreams | Rare/vague | Vivid, narrative |
8. Functions of Sleep (Important for Exams)
- Memory consolidation: REM sleep consolidates procedural and emotional memories; N3 consolidates declarative memory
- Metabolic restoration: N3 is associated with growth hormone secretion and anabolic processes
- Immune function: Sleep deprivation impairs immune responses
- Cognitive function: Sleep deprivation causes reaction time slowing and vigilance deficits
- Metabolic regulation: Chronic sleep deficiency → glucose intolerance, obesity risk, metabolic syndrome
- Cardiovascular health: Sleep deficiency linked to accelerated atherosclerosis and cardiac disease
- CNS clearance: Glymphatic system flushes metabolic waste (including amyloid-beta) during sleep
Quick Exam Summary
NREM stages:
N1 → Theta waves, slow rolling eye movements, vertex waves
N2 → Sleep spindles + K complexes
N3 → Delta waves (slow-wave sleep, deep sleep)
REM:
Low-voltage mixed EEG, rapid eye movements, atonia
Cholinergic; monoamines SILENT
Sleep cycle:
N1 → N2 → N3 → N2 → REM (90-100 min/cycle, x4-6 per night)
First third = N3 dominant
Last third = REM dominant
Key structures:
SCN → circadian pacemaker
VLPO → GABAergic, promotes sleep
Lateral hypothalamus → orexin (wake) + MCH (REM)
Locus coeruleus → NE (wake-promoting)
Adenosine → sleep pressure; caffeine blocks it
- Harrison's Principles of Internal Medicine 22E (2025), pp. 253-254
- Adams and Victor's Principles of Neurology 12E, pp. 411-414
- Bradley and Daroff's Neurology in Clinical Practice, pp. 2305-2308
This is a shared conversation. Sign in to Orris to start your own chat.