Stages of healing
Reading File
Finding Sources
Searching PubMed
"wound healing"[MeSH Terms] AND "phases"
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough breakdown of the stages of wound healing, drawn from Schwartz's Principles of Surgery (11th ed.).
Stages of Wound Healing
Wound healing is a complex, overlapping cascade divided into three major phases. All tissues heal by similar mechanisms, progressing through inflammation, proliferation, and remodeling.
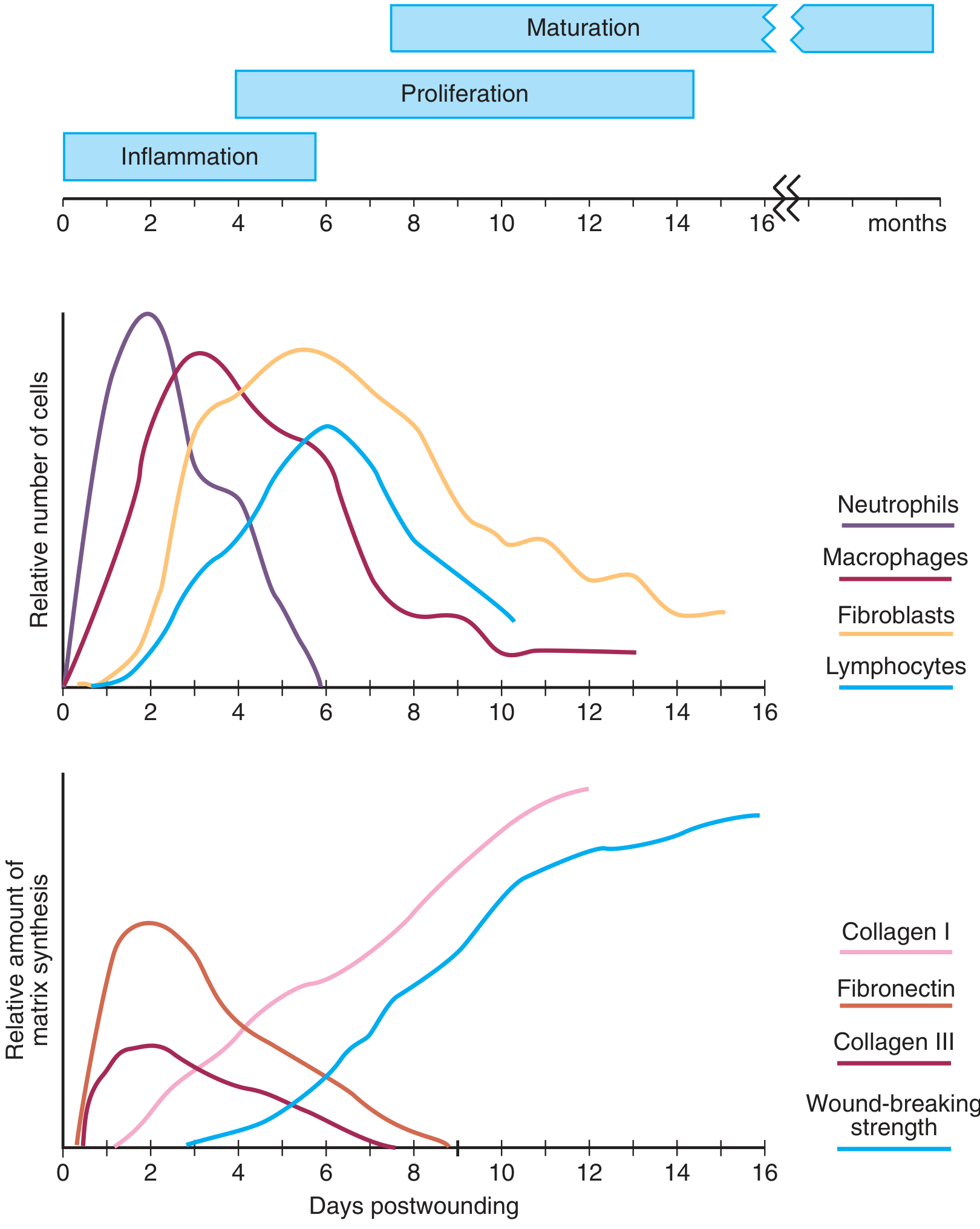
Phase 1: Hemostasis and Inflammation (Day 0 to ~Day 6)
These two events are tightly linked - hemostasis initiates inflammation.
Hemostasis (minutes to hours)
- Tissue injury disrupts blood vessels, exposing subendothelial collagen to platelets
- Platelets aggregate, degranulate, and activate the coagulation cascade
- Platelet alpha granules release key mediators:
- PDGF (platelet-derived growth factor)
- TGF-beta (transforming growth factor-beta)
- PAF (platelet-activating factor)
- Fibronectin and serotonin
- The resulting fibrin clot stops bleeding and serves as a scaffold for incoming inflammatory cells
Inflammation
Neutrophils (PMNs) - first responders:
- Enter the wound within hours, peak at 24-48 hours
- Recruited by complement factors, IL-1, TNF-alpha, TGF-beta, and bacterial products
- Primary role: phagocytosis of bacteria and tissue debris
- Release cytokines (especially TNF-alpha) that influence angiogenesis and collagen synthesis
- Release proteases (collagenases) for matrix degradation
- Not required for collagen deposition or wound strength
Macrophages - the orchestrators:
- Derived from circulating monocytes
- Reach significant numbers at 48-96 hours, persist until healing is complete
- Phagocytose debris, generate reactive oxygen species and nitric oxide
- Release TGF-beta, VEGF, IGF, EGF, and lactate to regulate cell proliferation and migration
- Essential to successful healing - macrophage depletion severely impairs wound repair
T-Lymphocytes - the bridge:
- Peak at approximately 1 week post-injury
- Bridge the transition from inflammation to proliferation
- CD8+ suppressor subset: depletion enhances healing
- CD4+ helper subset: depletion has no effect
- Regulate fibroblast collagen synthesis via IFN-gamma, TNF-alpha, and IL-1 through direct cell-cell contact
Phase 2: Proliferation (Days 4-12)
Tissue continuity is reestablished during this phase. Key players are fibroblasts and endothelial cells.
Fibroblast Activity and Matrix Synthesis
- Fibroblasts are recruited primarily by PDGF (the strongest chemotactic factor for them)
- Once in the wound, they first proliferate, then become activated by macrophage-derived cytokines
- Wound fibroblasts synthesize more collagen than normal fibroblasts
- Lactate accumulating in the wound (~10 mmol) is a potent regulator of collagen synthesis via ADP-ribosylation
Collagen synthesis steps:
- mRNA is translated into protocollagen (~1000 amino acids; glycine at every 3rd position)
- Proline and lysine are hydroxylated (requires oxygen, iron, alpha-ketoglutarate, and vitamin C as electron donor)
- Glycosylation occurs in the endoplasmic reticulum
- Three alpha-helical chains coil into a procollagen triple helix
- Registration peptides are cleaved extracellularly by procollagen peptidase
- Collagen monomers polymerize and cross-link
Matrix deposition sequence:
- Early: fibronectin + collagen type III
- Mid: glycosaminoglycans and proteoglycans (dermatan/chondroitin sulfate peak ~3 weeks)
- Late: collagen type I (final, dominant matrix)
Angiogenesis
- Endothelial cells migrate from intact venules near the wound
- Stimulated by TNF-alpha, TGF-beta, and VEGF
- Form new capillary tubules - essential for nutrient and oxygen delivery
- The combination of new capillaries + fibroblasts + connective tissue = granulation tissue
Epithelialization
- Epidermal cells at wound margins begin migrating and proliferating
- Stimulated by EGF, KGF (keratinocyte growth factor), and other mediators
Wound Contraction
- Begins almost immediately after injury
- Mediated largely by myofibroblasts (fibroblasts with alpha-smooth muscle actin stress fibers)
- Alpha-smooth muscle actin is undetectable until day 6, peaks around day 15, then fades by week 4 as cells undergo apoptosis
- Significant in healing by secondary intention
Phase 3: Maturation and Remodeling (Weeks to Months - up to 1-2 years)
- Begins during the proliferative phase and continues for 6-12 months post-injury
- Characterized by reorganization of previously synthesized collagen
- Matrix metalloproteinases (MMPs) break down old collagen; net collagen content reflects the balance between collagenolysis and synthesis
- Collagen type III is progressively replaced by collagen type I
- Fibril cross-linking increases tensile strength and enzymatic degradation resistance
- The wound becomes progressively avascular and acellular
- Tensile strength increases for months after collagen reaches its plateau level, but the scar never fully recovers the strength of uninjured tissue (maximum ~80% of normal)
| Time point | Tensile strength |
|---|---|
| 1 week | ~3% |
| 3 weeks | ~20% |
| 3 months | ~80% (maximum) |
Summary Table
| Phase | Timing | Key Cells | Key Events |
|---|---|---|---|
| Hemostasis | Minutes-hours | Platelets | Clot formation, scaffold, growth factor release |
| Inflammation | Days 0-6 | Neutrophils, macrophages, lymphocytes | Debridement, bacterial clearance, cell recruitment |
| Proliferation | Days 4-12 | Fibroblasts, endothelial cells | Collagen synthesis, angiogenesis, granulation tissue, epithelialization |
| Maturation/Remodeling | Weeks-months | Myofibroblasts, fibroblasts | Collagen remodeling, scar maturation, tensile strength gain |
Key Factors That Impair Healing
-
Hypoxia / poor blood supply
-
Infection
-
Nutritional deficiencies (especially vitamin C, zinc, protein)
-
Diabetes mellitus
-
Corticosteroids
-
Excess wound tension
-
Age
-
Schwartz's Principles of Surgery, 11th Edition, Chapter 9
This is a shared conversation. Sign in to Orris to start your own chat.