Hairfall
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
alopecia hair loss treatment
Searching the Web
hair loss causes types diagnosis treatment 2025
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, textbook-sourced information to give a thorough answer. Here it is:
Hair Loss (Alopecia) - Complete Overview
1. Types & Causes
Hair loss broadly falls into non-scarring (reversible) and scarring (permanent follicle destruction) categories. The major types are:
Androgenetic Alopecia (AGA) - Most Common
- Affects up to 80% of men and 50% of women over their lifetime.
- Caused by progressive miniaturization of terminal hair follicles driven by dihydrotestosterone (DHT), a testosterone metabolite converted by 5α-reductase enzymes.
- Genetically determined - polygenic, with the androgen receptor gene (AR) on chromosome Xq11-12 being the major determinant in men.
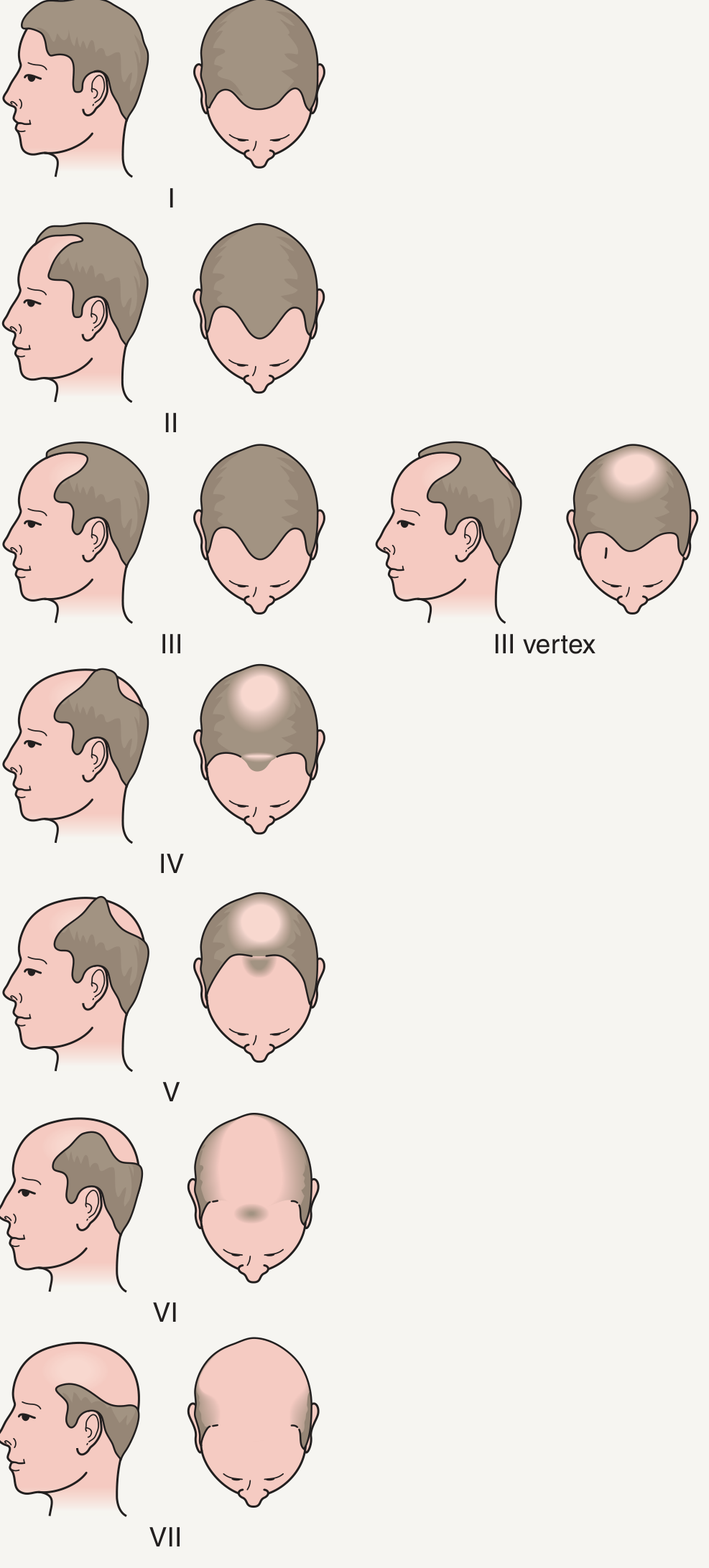
- In men: frontotemporal recession and vertex thinning (Hamilton-Norwood scale, Types I-VII).
- In women: diffuse crown thinning with preserved frontal hairline (Ludwig pattern). In premenopausal women it can signal hyperandrogenism (check for hirsutism, acne).
Norwood Scale for Male Pattern Hair Loss:
Telogen Effluvium (TE) - Diffuse Shedding
- Acute TE: A large number of follicles enter the resting (telogen) phase simultaneously due to a trigger. Hair shedding begins ~3 months after the triggering event.
- Common triggers include: surgery, childbirth, high fever, severe physical/emotional stress, crash dieting, iron deficiency, thyroid disorders, and many drugs (see list below).
- COVID-19: Severe TE is well-documented 2-3 months after SARS-CoV-2 infection.
- Acute TE: shedding >100-200 hairs/day. Typically self-resolves once the trigger is removed.
- Chronic TE: mostly middle-aged women, mild shedding (<100/day), temporal thinning, often unexplained. No consistently effective treatment.
Alopecia Areata (AA) - Autoimmune Patchy Loss
- Round or oval patches of complete hair loss, typically 1-5 cm in diameter, on scalp, beard, eyebrows, eyelashes.
- Autoimmune - autoreactive CD8+ T cells target follicular melanocytes; the hair bulb's immune privilege collapses.
- Key clues: "exclamation point" hairs (tapered at base), yellow/black dots on dermoscopy, nail pitting in ~10% of cases.
- Variants: Alopecia totalis (complete scalp), Alopecia universalis (all body hair), Ophiasis (band-like temporal/occipital loss).
- Associated with atopic dermatitis, thyroiditis, SLE, vitiligo, Down syndrome.
- ~25% have a positive family history.
Anagen Effluvium
- Acute diffuse loss starting 4-6 weeks after chemotherapy or scalp radiation, up to 1000 hairs/day.
- Usually regrows after therapy ends; permanent alopecia possible with high-dose radiation or busulfan/docetaxel regimens.
- Scalp hypothermia (cooling cap) can prevent or reduce loss during chemo.
Drugs That Cause Hair Loss
From Goldman-Cecil Medicine, notable culprits include:
- Anticoagulants (warfarin, heparin, apixaban, rivaroxaban)
- Antiepileptics (valproic acid, carbamazepine)
- Antithyroid drugs, beta-blockers, ACE inhibitors
- Oral contraceptives, androgens, aromatase inhibitors
- Retinoids, lithium, interferons
2. Diagnosis & Investigations
| Test | What it shows |
|---|---|
| Pull test | Grasp 40 hairs, slow pull - >4-6 club hairs = abnormal (TE); >6 anagen hairs = anagen effluvium |
| Blood tests | CBC, TSH, ferritin/iron, vitamin D, B12, zinc, androgens (DHEAS, testosterone, LH/FSH in women), ANA |
| Dermoscopy (trichoscopy) | Yellow dots, exclamation-point hairs (AA); miniaturized vellus hairs (AGA) |
| Scalp biopsy | Definitive for scarring alopecias; distinguishes AA from other types histologically |
| Light microscopy | Assesses hair shaft disorders |
| Trichogram | 50 hairs plucked - ratio of anagen:telogen:dystrophic hairs |
Key principle: Diffuse hair loss without visible alopecia is common in TE because 50% of hairs must be lost before density reduction is visible.
3. Treatment
Androgenetic Alopecia
| Treatment | Details |
|---|---|
| Topical minoxidil | 2% or 5% solution/foam applied daily; increases anagen duration and follicle size; first-line for both sexes |
| Low-dose oral minoxidil | 0.625-2.5 mg/day (women), 2.5-5 mg/day (men); growing evidence of safety and efficacy |
| Finasteride (oral, 1 mg/day) | FDA-approved for men; inhibits type II 5α-reductase; hair growth peaks at 1-2 years; must continue indefinitely or AGA returns; not for women of childbearing age |
| Dutasteride | Inhibits both type I and II 5α-reductase; more potent than finasteride |
| Spironolactone | Anti-androgen for women; especially useful in women also getting facial hypertrichosis from oral minoxidil |
| PRP (Platelet-Rich Plasma) | Autologous injections of growth factors; evidence mixed - some RCTs show no benefit over saline |
| Low-level laser therapy (LLLT) | FDA-cleared device; modest improvement in hair density in small studies |
| Hair transplantation | Gold standard surgical option; follicular unit transplantation (FUT/FUE) - natural-appearing results; patients should continue minoxidil/finasteride post-op to preserve results |
Minoxidil side effects: Hypertrichosis of cheeks/forehead (more with oral), headache, ankle edema, contact dermatitis (topical), hypotension, tachycardia (oral - rare at low doses).
Finasteride side effects (<2%): Decreased libido, erectile dysfunction. Rare: gynecomastia, depression. Lowers PSA by ~50% (inform patient and physician). "Post-finasteride syndrome" (persistent sexual dysfunction, brain fog) is controversial but FDA has added suicidal ideation warning to the label (2025 update).
Alopecia Areata
| Treatment | Details |
|---|---|
| Intralesional corticosteroids | Triamcinolone acetonide injected intradermally; first-line for limited patchy AA |
| Topical/systemic corticosteroids | Used for more extensive disease |
| JAK inhibitors | Ritlecitinib (FDA-approved 2023) and baricitinib (FDA-approved) are now standard for moderate-to-severe AA; ritlecitinib vs baricitinib indirect comparison shows similar efficacy (PMID: 39445776, 2025 network meta-analysis) |
| Contact immunotherapy (DPCP/SADBE) | Chemical sensitizers applied to scalp; >60% of patients with widespread patchy AA respond |
| Spontaneous remission | Common in limited AA - high self-remission rate within 12 months |
Telogen Effluvium
- Remove the precipitating cause (treat underlying thyroid/iron deficiency, stop offending drug, address nutritional deficit).
- Acute TE resolves spontaneously in months. Chronic TE has no reliably effective treatment.
- May unmask or worsen underlying AGA.
Anagen Effluvium
- Scalp hypothermia (cooling cap) during chemotherapy - can prevent or reduce loss, including permanent loss from docetaxel regimens.
- Topical minoxidil accelerates regrowth but does not prevent loss.
4. Prevention & Hair Care
- Address nutritional gaps: iron, ferritin, zinc, vitamin D, biotin, protein are the most important. A 2024 systematic review (Wang R et al., Mol Nutr Food Res) confirmed micronutrient deficiencies are common in androgenetic alopecia.
- Avoid tight hairstyles (traction alopecia), excessive heat, and harsh chemical treatments.
- Manage stress (major trigger for TE).
- Maintain scalp hygiene - seborrheic dermatitis worsens hair loss.
- If on medications known to cause TE (valproate, heparin, etc.), proactively monitor hair status.
- Postpartum shedding is physiologic and self-resolving by 9 months - no treatment needed, only reassurance.
Sources: Dermatology 2-Volume Set 5e; Goldman-Cecil Medicine 22e; Andrews' Diseases of the Skin; Fitzpatrick's Dermatology; Harrison's Principles of Internal Medicine 22e (2025).
This is a shared conversation. Sign in to Orris to start your own chat.