Total Abdominal Hysterectomym
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Finding Sources
I now have comprehensive textbook content. Let me compile a thorough, well-organized answer.
Total Abdominal Hysterectomy (TAH)
Definition
A total hysterectomy is surgical removal of both the uterine corpus and the cervix. When performed through an abdominal incision, it is called a Total Abdominal Hysterectomy (TAH). It is one of the most commonly performed major surgical procedures - the abdominal approach accounts for approximately 60% of all hysterectomies (vs. 14% laparoscopic and 26% vaginal) in the United States.
A subtotal (supracervical) hysterectomy removes only the corpus, leaving the cervix behind. TAH removes both.
Types of Hysterectomy (by extent)
| Type | Structures Removed |
|---|---|
| Subtotal / Supracervical | Uterine corpus only (cervix left in) |
| Total (TAH) | Uterine corpus + cervix |
| TAH + BSO | Uterus + cervix + bilateral salpingo-oophorectomy (tubes + ovaries) |
| Radical (Wertheim's) | Uterus + cervix + parametria + upper vagina + pelvic nodes (for cervical cancer) |
Indications
- Uterine leiomyomas (fibroids) - most common benign indication
- Abnormal uterine bleeding refractory to conservative management
- Endometriosis / adenomyosis (especially with bilateral oophorectomy if severe)
- Uterine prolapse (often via vaginal route, but TAH if added pathology)
- Endometrial carcinoma (TAH + BSO is standard surgical staging)
- Ovarian carcinoma staging (TAH + BSO + omentectomy + lymph node dissection)
- Uterine leiomyosarcoma (TAH + bilateral oophorectomy)
- Intractable postpartum hemorrhage / placenta accreta (emergency cesarean hysterectomy)
- Cervical carcinoma (early stages)
Preoperative Preparation
- Informed consent including risks of bleeding, infection, urinary tract injury, bowel injury, and loss of fertility
- Urine culture, CBC, coagulation profile, blood typing
- Bowel preparation (individualized)
- Prophylactic antibiotics (cephalosporin) within 60 minutes of incision
- DVT prophylaxis (compression stockings ± LMWH)
- Foley catheter placement
Patient Positioning & Incision
The patient is placed in the dorsal supine position (modified lithotomy if combined vaginal access is needed). The incision is either:
- Pfannenstiel (low transverse) - preferred for benign disease; better cosmesis, lower wound complications
- Vertical midline - chosen for malignancy, large pathology, need for full abdominal exploration, or re-operative cases
Choice of incision depends on indication, body habitus, prior surgical history, and size of uterus/pathology.
Step-by-Step Surgical Technique
(Based on Sabiston Textbook of Surgery and Schwartz's Principles of Surgery)
1. Abdominal Entry & Exploration
- Enter the abdomen through the chosen incision
- Inspect the upper abdomen for evidence of extrapelvic disease
- Place a suitable self-retaining retractor (e.g., Balfour)
- Grasp the uterus at each cornu with clamps (Kocher or Lahey) and elevate into the incision
2. Round Ligament Transection
- Identify and divide the round ligament bilaterally
- This opens the anterior and posterior leaves of the broad ligament
3. Broad Ligament Incision & Ureter Identification
- Extend the peritoneal incision from the round ligament laterally past the ovarian hilum (if oophorectomy planned) or medially below the utero-ovarian ligament (if ovaries are conserved)
- Bluntly open the retroperitoneal space and identify the ureter on the medial leaf of the broad ligament - this is critical to prevent ureteric injury
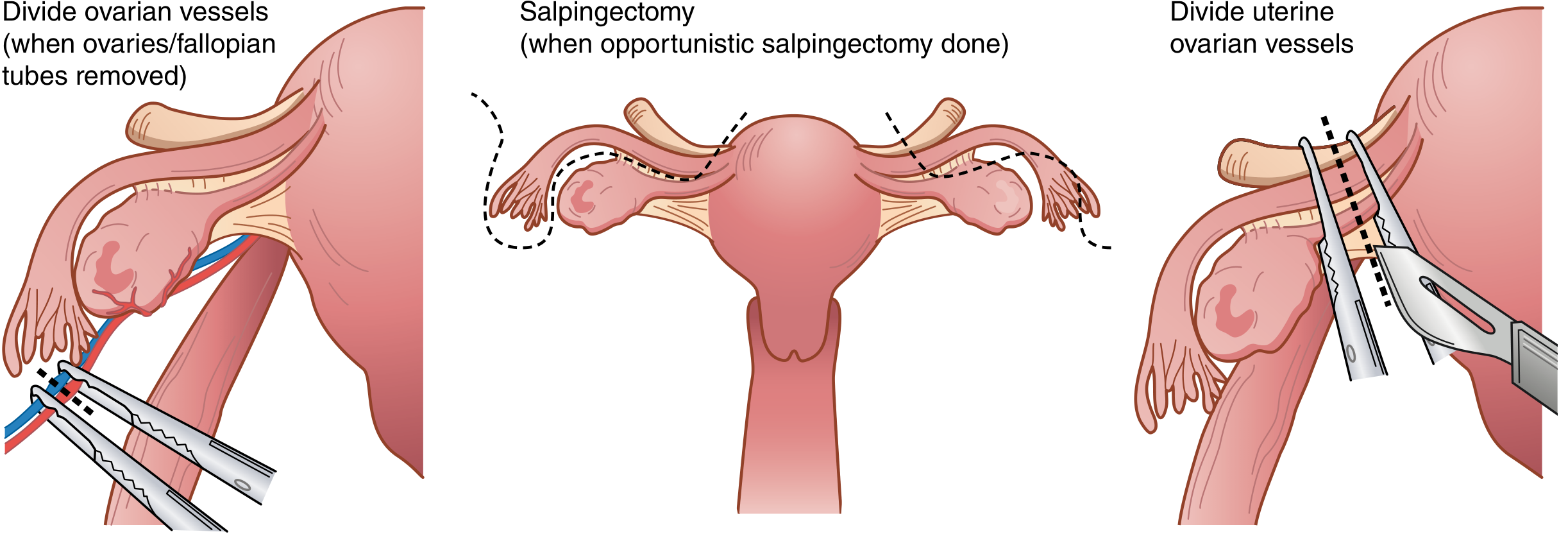
4. Adnexal Management
If ovaries/tubes are to be removed (BSO):
- Incise posterior leaves of broad ligament
- Double-clamp the infundibulopelvic (IP) ligament containing the ovarian vessels with curved Heaney or Zeppelin clamps
- Divide between clamps with curved Mayo scissors; doubly ligate pedicles
If ovaries are to be conserved:
- Create an opening below the utero-ovarian ligament and fallopian tube
- Clamp, divide, and doubly ligate the utero-ovarian vessels with Kelly or Heaney clamps
Opportunistic salpingectomy (removal of tubes only, conserving ovaries) is increasingly performed to reduce future ovarian cancer risk.
5. Bladder Mobilization
- Sharply dissect the bladder off the anterior surface of the uterus and cervix using Metzenbaum scissors or electrocautery
- Retract the bladder inferiorly below the level of the cervix
6. Uterine Vessel Ligation
- Skeletonize the uterine vessels along the lateral uterus by incising the remaining posterior broad ligament leaves
- Place a curved Heaney or Zeppelin clamp across the uterine vessels at the level of the internal cervical os
- Cut and suture-ligate the pedicle
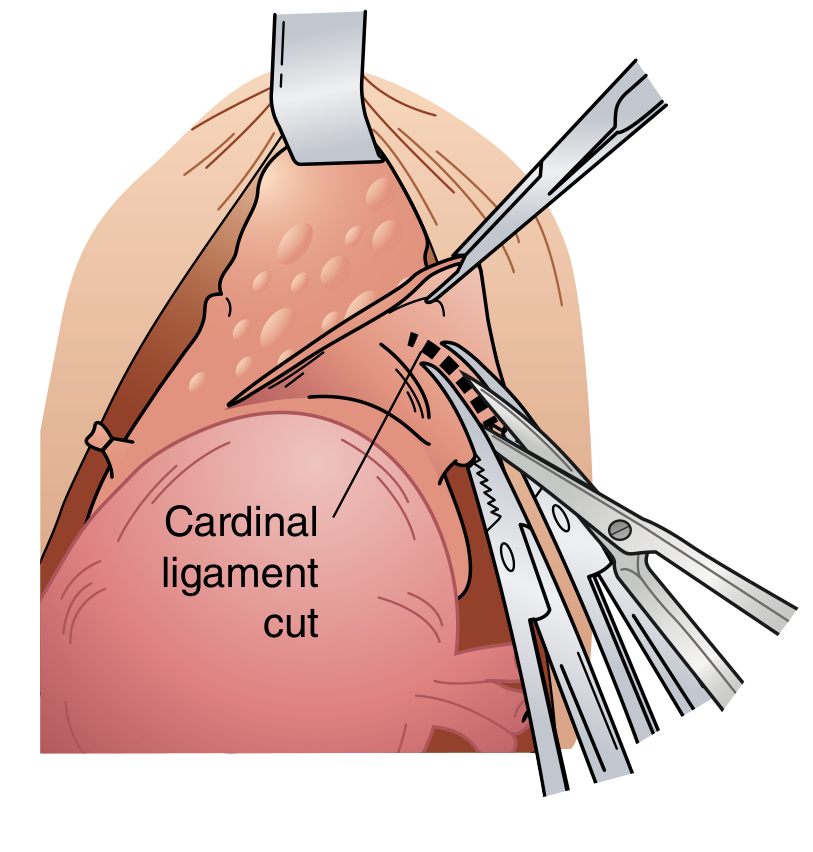
7. Cardinal & Uterosacral Ligament Division
- Serially clamp, cut, and ligate the cardinal ligaments (Mackenrodt's ligaments) bilaterally in steps
- Divide the uterosacral ligaments
- Continue until both sides are clear at the level of the external cervical os
8. Colpotomy & Specimen Removal
- Place curved clamps across the vagina just below the cervix bilaterally
- Cut with curved scissors just above the clamps to amputate the cervix from the vagina
- The specimen (uterus + cervix ± adnexa) is removed
9. Vaginal Cuff Closure
- Place Heaney transfixion stitches at each lateral vaginal angle - importantly, incorporating the ipsilateral uterosacral ligament for apical support (prevents vault prolapse)
- Close the remainder of the vaginal cuff with running or interrupted absorbable sutures (e.g., Vicryl 0 or 1)
- An alternative: direct sharp colpotomy around the cervix with Allis clamps placed on the vaginal edges for visualization before closure
10. Closure
- Pelvic reperitonization is not necessary
- Hemostasis confirmed
- Abdominal wall closed in layers (fascia, subcutaneous tissue, skin)
Key Anatomical Danger Points
| Structure at Risk | During Which Step | Prevention |
|---|---|---|
| Ureter | Broad ligament dissection, uterine vessel ligation | Retroperitoneal identification before clamping |
| Bladder | Anterior dissection, colpotomy | Sharp dissection under direct vision; mobilize completely below cervix |
| Uterine/ovarian vessels | Pedicle ligation | Double clamping and suture ligation |
| Bowel (sigmoid, rectum) | Posterior dissection, closure | Careful retraction, identify anatomy |
The ureter is at highest risk near the infundibulopelvic ligament and near the uterine artery (where it passes under the uterine artery - "water under the bridge"). Always identify it before clamping.
Complications
(Tintinalli's Emergency Medicine)
Infection rate: 3-10% (higher with abdominal vs. vaginal route). Overall complication rate is significantly higher for malignant vs. benign indications (19.4% vs. 7.9%). Risk factors include obesity, diabetes, and prolonged operative time.
| Category | Specific Complications |
|---|---|
| Infectious | Wound infection, infected vaginal cuff hematoma/cellulitis/abscess, ovarian abscess, UTI |
| Hemorrhagic | Intraoperative hemorrhage, postoperative hematoma |
| Urological | Bladder injury, ureteral injury, urinary retention |
| GI | Ileus, bowel injury, bowel obstruction |
| Wound | Dehiscence, evisceration |
| Thromboembolic | DVT, pulmonary embolism, phlebitis |
| Pulmonary | Atelectasis, pneumonia |
| Long-term | Vaginal vault prolapse, pelvic floor dysfunction, premature menopause (if BSO in premenopausal patient) |
Variants & Related Procedures
- TAH + BSO: adds bilateral salpingo-oophorectomy; standard for endometrial cancer, ovarian cancer, or peri/postmenopausal patients with benign disease
- TAH + BSO + Staging laparotomy: for gynecologic malignancies - includes omentectomy, peritoneal washings, and lymph node dissection
- Radical (Wertheim) hysterectomy: for cervical carcinoma - includes parametrectomy and upper vaginectomy
- Laparoscopic hysterectomy (TLH): same steps but using ports, energy devices, and a uterine manipulator with colpotomizer cup; avoids laparotomy
- Robotic hysterectomy: similar to laparoscopic but higher cost; no proven clinical benefit over laparoscopic for benign conditions
Postoperative Care
- Ambulation within 24 hours (DVT prevention)
- Foley catheter removal by postoperative day 1
- Diet advancement as tolerated
- Pain management (multimodal - NSAIDs + opioid-sparing)
- Pelvic rest for 6-8 weeks (no intercourse, tampon use, or heavy lifting)
- Discharge typically on postoperative day 2-4
- If premenopausal with BSO: hormone replacement therapy counseling
Sources:
- Sabiston Textbook of Surgery, pp. 2799-2800 (Chapter 120 - Steps to completing hysterectomy)
- Schwartz's Principles of Surgery, 11th Edition, p. 1825 (Chapter 41 - Procedures for Abnormal Uterine Bleeding)
- Tintinalli's Emergency Medicine, Chapter 105 - Complications of Major Gynecologic-Abdominal Surgery
This is a shared conversation. Sign in to Orris to start your own chat.