Explain me about oral cavity and salivary glands for a seminar
Reading File
Finding Sources
Finding Sources
Searching the Web
oral cavity anatomy salivary glands seminar overview 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Searching Images
oral cavity anatomy diagram salivary glands parotid submandibular sublingual
Loading Image
Loading Image
Finding Sources
Loading Image
Finding Sources
Reading File
Loading Image
Now I have comprehensive content. Let me compile the full seminar-ready response.
Oral Cavity and Salivary Glands — Seminar Notes
1. ORAL CAVITY — Overview
The oral cavity is the gateway to the digestive system. It lies inferior to the nasal cavities, opens anteriorly through the oral fissure, and communicates posteriorly with the oropharynx via the oropharyngeal isthmus.
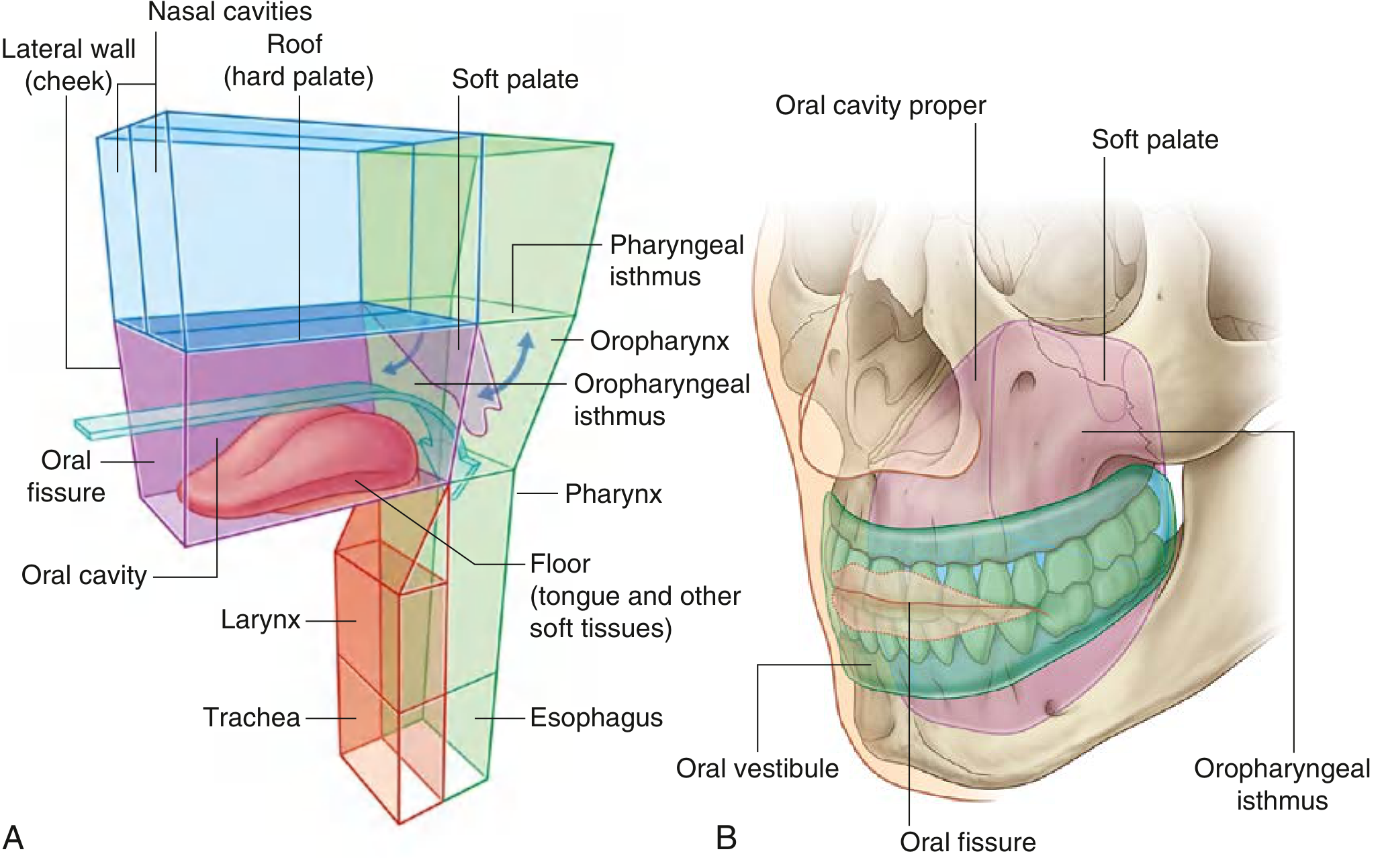
Boundaries
| Wall | Structure |
|---|---|
| Roof | Hard palate (anterior 2/3) + Soft palate (posterior 1/3) |
| Floor | Mylohyoid muscle + tongue + soft tissues |
| Lateral walls | Cheeks (buccinator muscle) |
| Anterior opening | Oral fissure (lips) |
| Posterior opening | Oropharyngeal isthmus |
Two Compartments
The dental arches (teeth + alveolar bone) divide the cavity into:
- Oral Vestibule — horseshoe-shaped space between dental arches and cheeks/lips
- Oral Cavity Proper — inner space enclosed by the dental arches
Seven Anatomic Subsites (clinically important)
- Lips
- Oral tongue (anterior 2/3)
- Floor of mouth
- Buccal mucosa
- Gingiva / alveolar ridges (upper and lower)
- Retromolar trigone (RMT)
- Hard palate
(KJ Lee's Essential Otolaryngology)
Functions
- Digestion: mastication + initial chemical breakdown (salivary amylase)
- Speech: modulates sounds from the larynx; palate, tongue, teeth act as articulators
- Breathing: alternate airway when nasal passages are obstructed
- Dental access: rubber dams prevent debris passage into airway
2. WALLS AND SKELETAL FRAMEWORK
Bones Contributing to the Oral Cavity
- Maxillae — form anterior 2/3 of the hard palate (via palatine processes)
- Palatine bones — form posterior 1/3 of hard palate (horizontal plates); contain the greater palatine foramen (transmits greater palatine nerve + vessels) and lesser palatine foramen (transmits lesser palatine nerve → soft palate)
- Mandible — movable lower jaw; establishes separation between dental arches
- Sphenoid, temporal, hyoid — associated muscular attachments
Incisive Canal
Opens behind incisor teeth → transmits greater palatine vessels and nasopalatine nerves to the hard palate.
3. TONGUE
The tongue occupies much of the oral cavity floor and has an oral (anterior 2/3) and a pharyngeal (posterior 1/3) part.
Surface Features
| Structure | Description |
|---|---|
| Filiform papillae | Most numerous; no taste function |
| Fungiform papillae | Diffusely scattered; have taste buds |
| Foliate papillae | Lateral tongue; have taste buds |
| Circumvallate papillae | Large; V-shaped row at junction of anterior & posterior; have taste buds |
| Sulcus terminalis | Groove just anterior to circumvallate papillae |
| Foramen cecum | Pit at apex of sulcus terminalis — embryologic origin of thyroid gland |
| Frenulum | Anterior fold attaching tongue to floor of mouth; Wharton ducts open on either side |
Innervation
| Function | Nerve |
|---|---|
| General sensation — anterior 2/3 | Lingual nerve (V3) |
| Taste — anterior 2/3 | Chorda tympani (VII) via lingual nerve |
| General sensation + taste — posterior 1/3 | Glossopharyngeal nerve (IX) |
| Motor (all muscles except palatoglossus) | Hypoglossal nerve (XII) |
| Palatoglossus | Vagus nerve (X) |
4. PALATE
Hard Palate
- Formed by palatine processes of maxillae (anterior 2/3) and horizontal plates of palatine bones (posterior 1/3)
- Sensory: maxillary nerve (V2) via greater/lesser palatine nerves and nasopalatine nerve
Soft Palate
- Posterior muscular extension; can be raised to close off nasopharynx (during swallowing/speech)
- All muscles innervated by vagus nerve (X) via pharyngeal plexus — except tensor veli palatini (innervated by V3)
5. INNERVATION OF THE ORAL CAVITY
General sensory innervation is predominantly via the trigeminal nerve (V):
- Upper cavity (palate, upper teeth): maxillary nerve (V2)
- Lower cavity (lower teeth, anterior tongue): mandibular nerve (V3)
Taste:
- Anterior 2/3 of tongue → facial nerve (VII)
- Posterior 1/3 → glossopharyngeal nerve (IX)
Autonomic (glandular):
- Parasympathetic (secretomotor): carried by CN VII branches → submandibular & sublingual glands; and CN IX → parotid gland
- Sympathetic: from T1 → superior cervical ganglion → travel with trigeminal branches
(Gray's Anatomy for Students)
6. SALIVARY GLANDS
Salivary glands open into the oral cavity. They are classified as major (paired, large, named) and minor (small, embedded in mucosa).
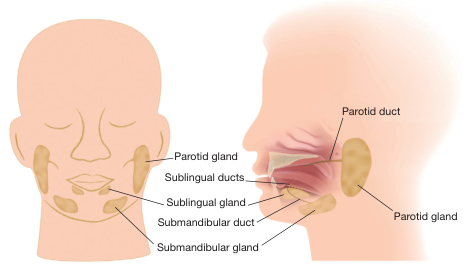
6A. MAJOR SALIVARY GLANDS
1. Parotid Gland
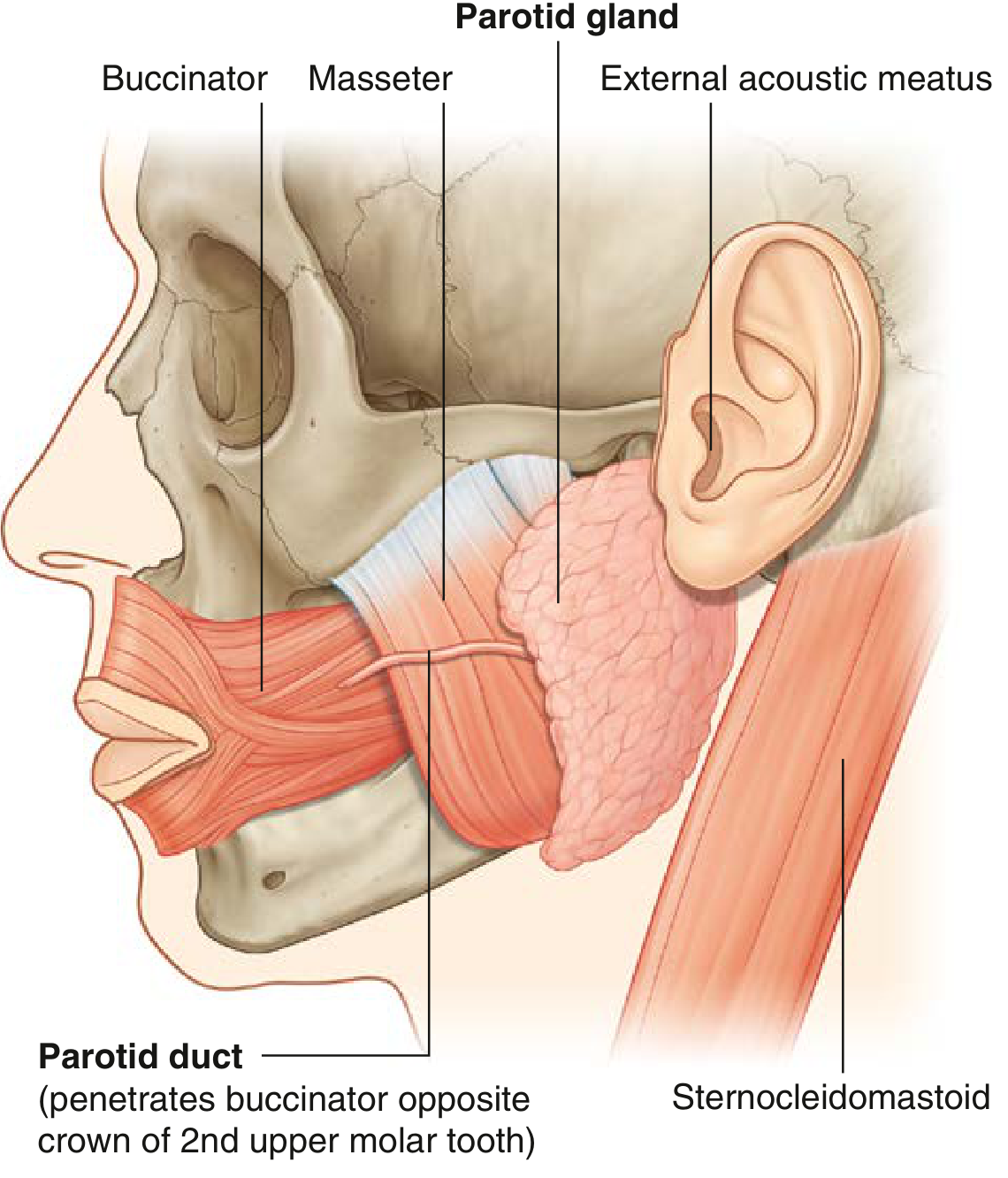
- Largest of the three major glands
- Located in a shallow triangular space bounded by:
- Posteriorly: sternocleidomastoid muscle
- Anteriorly: ramus of mandible
- Superiorly: external acoustic meatus + posterior zygomatic arch
- Extends over the masseter muscle anteriorly and posterobelly of digastric inferiorly
- Stensen's duct (parotid duct): passes anteriorly across the masseter → turns medially → penetrates the buccinator → opens at the parotid papilla opposite the crown of the 2nd upper molar
- Encloses: external carotid artery, retromandibular vein, facial nerve (VII) (extracranial portion)
- Secretion: purely serous (watery, high enzyme content)
- Produces ~2/3 of mouth's saliva when stimulated
2. Submandibular Gland
- Hook-shaped gland; smaller than parotid, larger than sublingual
- Superficial (larger) part: lies in submandibular fossa (below mylohyoid line, outside oral cavity proper), against medial surface of mandible
- Deep part: loops around posterior margin of mylohyoid → enters floor of oral cavity; lies lateral to root of tongue on hyoglossus
- Wharton's duct: emerges from deep part → passes forward → opens at sublingual caruncle (papilla) beside the base of the frenulum of the tongue
- The lingual nerve loops under Wharton's duct — crosses first lateral then medial as it descends
- Secretion: mixed (serous + mucous) — thicker saliva; produces 2/3 of mouth's saliva when unstimulated
3. Sublingual Gland
- Smallest of the three major glands
- Almond-shaped; immediately lateral to Wharton's duct and lingual nerve in floor of oral cavity
- Rivinus ducts (multiple): drain directly into floor of mouth or join the submandibular duct
- Secretion: mainly mucous
Summary Table — Major Salivary Glands
| Feature | Parotid | Submandibular | Sublingual |
|---|---|---|---|
| Size | Largest | Intermediate | Smallest |
| Location | Preauricular / retromandibular | Submandibular triangle | Floor of mouth |
| Duct name | Stensen's | Wharton's | Rivinus (multiple) |
| Duct opens | Opposite 2nd upper molar | Sublingual caruncle, beside frenulum | Floor of mouth / into submandibular duct |
| Secretion type | Serous only | Mixed | Mainly mucous |
| Unstimulated contribution | 20–25% | ~65% | Small |
| Stimulated contribution | ~60–65% | ~35% | Small |
6B. MINOR SALIVARY GLANDS
- 600–1000 small glands embedded in the mucosa and submucosa of lips, cheeks, tongue, palate, and floor of mouth
- Secrete mainly mucous; primarily lubricate the oral mucosa
- 5% of salivary gland tumors arise here, but ~80% of these are malignant — clinically important!
7. HISTOLOGY OF SALIVARY GLANDS
Ductal Architecture
Acinus → Intercalated duct → Striated duct → Excretory duct
- Acini: secretory end-pieces; surrounded by myoepithelial cells (contract to expel saliva)
- Serous acini (parotid): produce watery, protein-rich secretion
- Mucous acini (sublingual, minor glands): produce viscid, mucin-rich secretion
- Mixed acini (submandibular): both types, often with serous demilunes capping mucous acini
- Intercalated ducts: small caliber; lined by low cuboidal cells
- Striated ducts: lined by columnar cells with basal striations (abundant mitochondria) — responsible for ion modification of saliva
- Excretory ducts: larger, stratified epithelium
(KJ Lee's Essential Otolaryngology)
8. SALIVA — Composition and Functions
Composition (Whole Saliva)
- 99.5% water; specific gravity 1.002–1.012; pH 6.2–7.4
- Produced at ~1500 mL/day
| Component | Parotid | Submandibular |
|---|---|---|
| Flow (mL/min/gland, stimulated) | 0.7 | 0.6 |
| K⁺ (mEq/L) | 20 | 17 |
| Na⁺ (mEq/L) | 23 | 21 |
| HCO₃⁻ (mEq/L) | 20 | 18 |
| Ca²⁺ (mEq/L) | 2 | 3.6 |
| Protein (mg/dL) | 250 | 150 |
(Cummings Otolaryngology, Table 81.3)
Organic components: amylase (distinct from pancreatic amylase), glycoproteins, mucins, proline-rich proteins, cystatins, statherins
Functions of Saliva
- Digestion: salivary amylase initiates starch hydrolysis
- Lubrication: mucins coat food bolus, aiding swallowing
- Dental protection: bicarbonate buffers plaque acids; calcium/phosphate promote remineralization
- Antimicrobial: secretory IgA (sIgA), lysozyme, lactoferrin, leukotaxins, opsonins
- Taste: dissolves food molecules, delivering them to taste receptors
- Wound healing: growth factors (EGF) in saliva
9. AUTONOMIC INNERVATION OF SALIVARY GLANDS
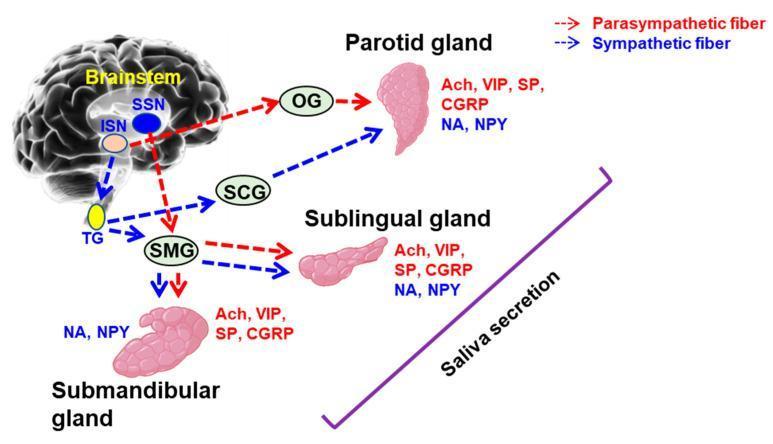
| Gland | Parasympathetic | Sympathetic |
|---|---|---|
| Parotid | CN IX → tympanic plexus → lesser petrosal nerve → otic ganglion → auriculotemporal nerve | Superior cervical ganglion (T1) |
| Submandibular & Sublingual | CN VII → chorda tympani → lingual nerve → submandibular ganglion | Superior cervical ganglion (T1) |
- Parasympathetic stimulation (via ACh/muscarinic M3) → increased watery saliva (IP3 → Ca²⁺ mobilization → fluid secretion)
- Sympathetic stimulation (β-adrenergic) → protein-rich secretion (cAMP → protein exocytosis)
10. DISORDERS OF THE SALIVARY GLANDS
A. Infectious
| Condition | Cause | Key Features |
|---|---|---|
| Mumps (viral parotitis) | Paramyxovirus | Children 4–6 yrs; bilateral parotid swelling; can cause orchitis, encephalitis, pancreatitis; self-limited |
| Acute sialadenitis | S. aureus (most common) | Debilitated/dehydrated patients; Rx: anti-staphylococcal antibiotics, hydration, warm compresses, sialogogues |
| Chronic sialadenitis | Decreased flow (sialolith, stasis) | Recurrent painful swelling; Rx: hydration, sialagogues, duct dilation, occasional sialoadenectomy |
| Granulomatous | Actinomyces israelii, TB, Sarcoidosis, Cat scratch disease | Often in HIV; Actinomycosis shows sulfur granules, draining sinuses; Rx: Penicillin 4–6 weeks |
B. Non-infectious
| Condition | Key Features |
|---|---|
| Sialolithiasis | 80% in submandibular gland; 65% of submandibular stones are radiopaque; 65% of parotid stones are radiolucent; pain/swelling after meals; Rx: sialolithotripsy, endoscopy, or sialodochoplasty |
| Sjögren syndrome | Autoimmune; bilateral gland swelling + xerostomia + keratoconjunctivitis sicca; Rx: pilocarpine (Salagen), cevimeline (Evoxac) |
| Xerostomia | Aging, radiation, medications (anticholinergics), Sjögren, diabetes; Rx: pilocarpine; amifostine for radiation-induced prevention |
| Necrotizing sialometaplasia | Benign, self-healing; lobular necrosis + pseudoepitheliomatous hyperplasia; heals in 6–12 weeks |
C. Neoplastic Disease
Key Rule: The smaller the gland, the higher the malignancy rate.
| Gland | Tumors | % Malignant |
|---|---|---|
| Parotid | 80% of all salivary tumors | 20–25% |
| Submandibular | 15% of all salivary tumors | 40–50% |
| Minor salivary glands | 5% | ~80% |
Benign Tumors:
- Pleomorphic adenoma — most common salivary neoplasm overall; 85% in parotid (90% in superficial lobe tail); slow, painless, firm; mixed epithelial + myoepithelial + stromal elements; Rx: excision with cuff of normal tissue; risk of malignant transformation to carcinoma ex-pleomorphic adenoma
- Warthin tumor (papillary cystadenoma lymphomatosum) — 2nd most common parotid tumor; older white males, smokers; bilateral in 10%; Tc-99m uptake on scan; Rx: excision
- Oncocytoma — elderly; Tc-99m uptake; sheets of granular oncocytes
Malignant Tumors:
| Type | % of Malignancies | Key Features |
|---|---|---|
| Mucoepidermoid carcinoma | 34% | Most common parotid malignancy; derived from excretory ducts; low-grade (mucous-rich, cystic) vs high-grade (epidermoid-rich, aggressive — 25% with facial palsy) |
| Adenoid cystic carcinoma | 20% | Most common submandibular + minor gland malignancy; perineural invasion ("skip lesions"); cribriform/tubular/solid subtypes; late distant metastases |
Poor prognostic signs: pain, CN VII involvement, fixation to adjacent structures.
(KJ Lee's Essential Otolaryngology; Cummings Otolaryngology Head & Neck Surgery)
11. TEETH AND DENTAL FORMULA
- Deciduous (primary): 20 teeth
- Permanent: 32 teeth — numbered superiorly right to left (1–16), inferiorly left to right (17–32)
- Each quadrant: 2 incisors, 1 canine, 2 premolars, 3 molars
Quick Revision Summary
| Topic | Key Points |
|---|---|
| Oral cavity compartments | Vestibule (outer) + Oral cavity proper (inner) |
| Roof | Hard palate (maxilla + palatine bone) + Soft palate |
| Floor | Mylohyoid + tongue |
| Tongue taste nerve | CN VII (anterior 2/3), CN IX (posterior 1/3) |
| Tongue motor | CN XII (all except palatoglossus — CN X) |
| Parotid duct | Opens opposite 2nd upper molar |
| Submandibular duct | Opens at sublingual caruncle beside frenulum |
| Saliva volume | ~1500 mL/day; 99.5% water |
| Sialolithiasis | 80% submandibular; submandibular stones = radiopaque |
| Most common benign tumor | Pleomorphic adenoma (parotid, superficial lobe) |
| Most common malignant tumor | Mucoepidermoid carcinoma |
| Smaller gland → | Higher malignancy rate |
Sources: Gray's Anatomy for Students | KJ Lee's Essential Otolaryngology | Cummings Otolaryngology Head & Neck Surgery | Bailey & Love's Short Practice of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.