explain me pcos
Reading File
Finding Sources
Searching PubMed
"polycystic ovary syndrome"[MeSH Terms] AND management
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive, well-sourced content from authoritative textbooks. Let me compile the full answer.
Polycystic Ovary Syndrome (PCOS)
PCOS is the most common endocrine disorder of women in their reproductive years, affecting 6-12% of women of reproductive age worldwide, across all ethnic groups. It is a heterogeneous condition - meaning its presentation varies significantly between individuals.
What Is It?
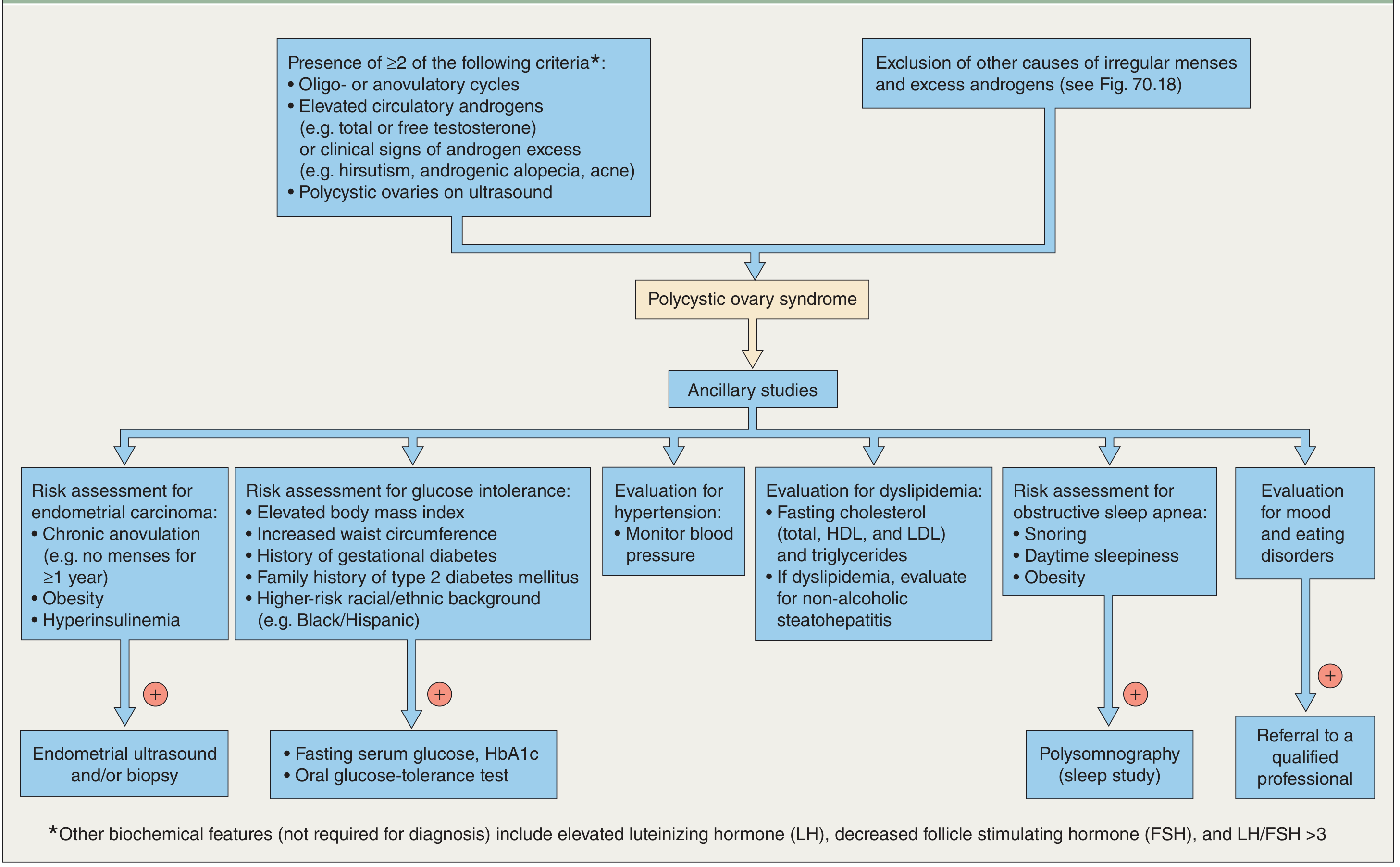
PCOS is defined by the Rotterdam criteria - a diagnosis requires any 2 of these 3 features, after excluding other causes:
- Oligo-ovulation or anovulation (irregular or absent ovulation)
- Hyperandrogenism - clinical (hirsutism, acne, androgenic alopecia) or biochemical (elevated testosterone)
- Polycystic ovaries on ultrasound (multiple small follicles arranged around the ovary)
Here is the diagnostic pathway:
Pathophysiology (How It Develops)
The hypothalamic-pituitary axis is structurally intact, but there is a functional derangement in how the ovaries communicate with it:
- The ovaries produce excess androgens (especially testosterone), driven partly by abnormal LH pulsatility
- Insulin resistance is a hallmark - present in the majority regardless of body weight. The resulting hyperinsulinemia stimulates the ovarian theca cells to produce even more androgens
- This creates a self-reinforcing cycle: high androgens + high insulin → disrupted follicle development → failure to ovulate → chronic anovulation → unopposed estrogen
- Genetic factors play a role - abnormalities in CYP17 and CYP19 (enzymes involved in androgen synthesis) have been identified
- LH levels tend to be elevated; FSH is relatively low and constant - the LH:FSH ratio is often >3
Clinical Features
Patients typically present with one or more of the following:
| Feature | Details |
|---|---|
| Menstrual irregularity | Oligomenorrhea (cycles > 35 days), amenorrhea, or sometimes heavy dysfunctional bleeding |
| Hirsutism | Excess androgen-driven hair growth on face, chest, abdomen |
| Acne & oily skin | Driven by androgens |
| Androgenic alopecia | Thinning at the crown |
| Obesity | Present in ~50-70%; exacerbates insulin resistance |
| Subfertility | Due to infrequent or absent ovulation |
Onset typically begins at puberty and can worsen over time, though symptoms often improve in the years before menopause.
Associated Long-Term Risks
PCOS carries significant systemic health risks:
- Type 2 diabetes: Over 50% of women with PCOS develop it by age 40
- Endometrial hyperplasia and cancer: Due to chronic unopposed estrogen from anovulation
- Cardiovascular disease: Driven by hyperandrogenism, insulin resistance, and dyslipidemia
- Obstructive sleep apnea: Higher prevalence, especially with obesity
- Mood disorders and eating disorders: Increased prevalence
Investigations / Lab Workup
- Androgens: Total and free testosterone (mild elevation typical; very high levels suggest tumor)
- LH/FSH ratio: Often > 3 (not required for diagnosis but supportive)
- Fasting glucose / HbA1c / oral glucose tolerance test: To screen for diabetes
- Lipid panel: Fasting cholesterol, triglycerides
- TSH and prolactin: To exclude thyroid disease and hyperprolactinemia (important differentials)
- 17-hydroxyprogesterone: To exclude late-onset congenital adrenal hyperplasia
- Pelvic ultrasound: Looking for polycystic ovarian morphology
Differential Diagnoses to Exclude
Before diagnosing PCOS, these must be ruled out:
- Cushing syndrome
- Congenital adrenal hyperplasia (CAH)
- Androgen-secreting tumors (ovarian or adrenal) - suspect if onset is rapid
- Hyperprolactinemia
- Hypothyroidism or hyperthyroidism
Management
Treatment is individualized based on the patient's primary concerns and whether pregnancy is desired.
1. Lifestyle Modification (First-line for all)
Even a 5-10% reduction in body weight significantly improves menstrual regularity, ovulation rates, and androgen levels in overweight women. Diet and exercise improve insulin sensitivity and are foundational to all other treatments.
2. Not Desiring Pregnancy
- Combined oral contraceptives (COCs): First-line for menstrual regulation, endometrial protection, and treatment of acne/hirsutism
- Intermittent progestins (e.g., medroxyprogesterone acetate 5-10 mg for 10-14 days/month): Protects the endometrium from hyperplasia in anovulatory women
- Metformin (1500-2000 mg/day): Suppresses hepatic gluconeogenesis, improves insulin sensitivity, reduces androgens; ovulation may resume in up to 60-70%
- Anti-androgens (spironolactone, cyproterone acetate): For hirsutism and acne, usually combined with contraception
3. Desiring Pregnancy (Ovulation Induction)
- Letrozole (aromatase inhibitor, 5 mg on days 3-7): Now preferred first-line over clomiphene for ovulation induction - supported by recent evidence
- Clomiphene citrate (50 mg days 3-7): Established alternative; ~75-80% of women conceive with medical induction
- Gonadotropin injections: Under specialist supervision if oral agents fail
- Laparoscopic ovarian drilling (LOD): Surgical option (diathermy or laser punctures) for women who don't respond to medications; achieves unifollicular ovulation but carries a risk of adhesions
4. Emerging Treatments
Recent meta-analysis (2024) shows GLP-1 receptor agonists (e.g., semaglutide) are effective in PCOS women with obesity for weight loss and hormonal regulation - PMID: 39178623. Probiotics and synbiotics also show promise for insulin resistance management - PMID: 39599701.
Key Points Summary
- PCOS = diagnosis of exclusion; requires 2 of 3 Rotterdam criteria
- Core mechanism: insulin resistance + androgen excess + anovulation
- Affects 6-12% of reproductive-age women; >50% develop T2DM by age 40
- Manage based on patient goals: cycle control, fertility, androgen symptoms, metabolic risk
- Lifestyle change is always first-line regardless of presenting complaint
Sources: Goldman-Cecil Medicine (p. 2560), Berek & Novak's Gynecology (p. 1879), Dermatology 5e - Diagnostic Flowchart
This is a shared conversation. Sign in to Orris to start your own chat.