Circle of willis
Reading File
Finding Sources
Searching the Web
circle of Willis anatomy components clinical significance
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough overview of the Circle of Willis, drawn from multiple authoritative textbooks.
Circle of Willis
Overview
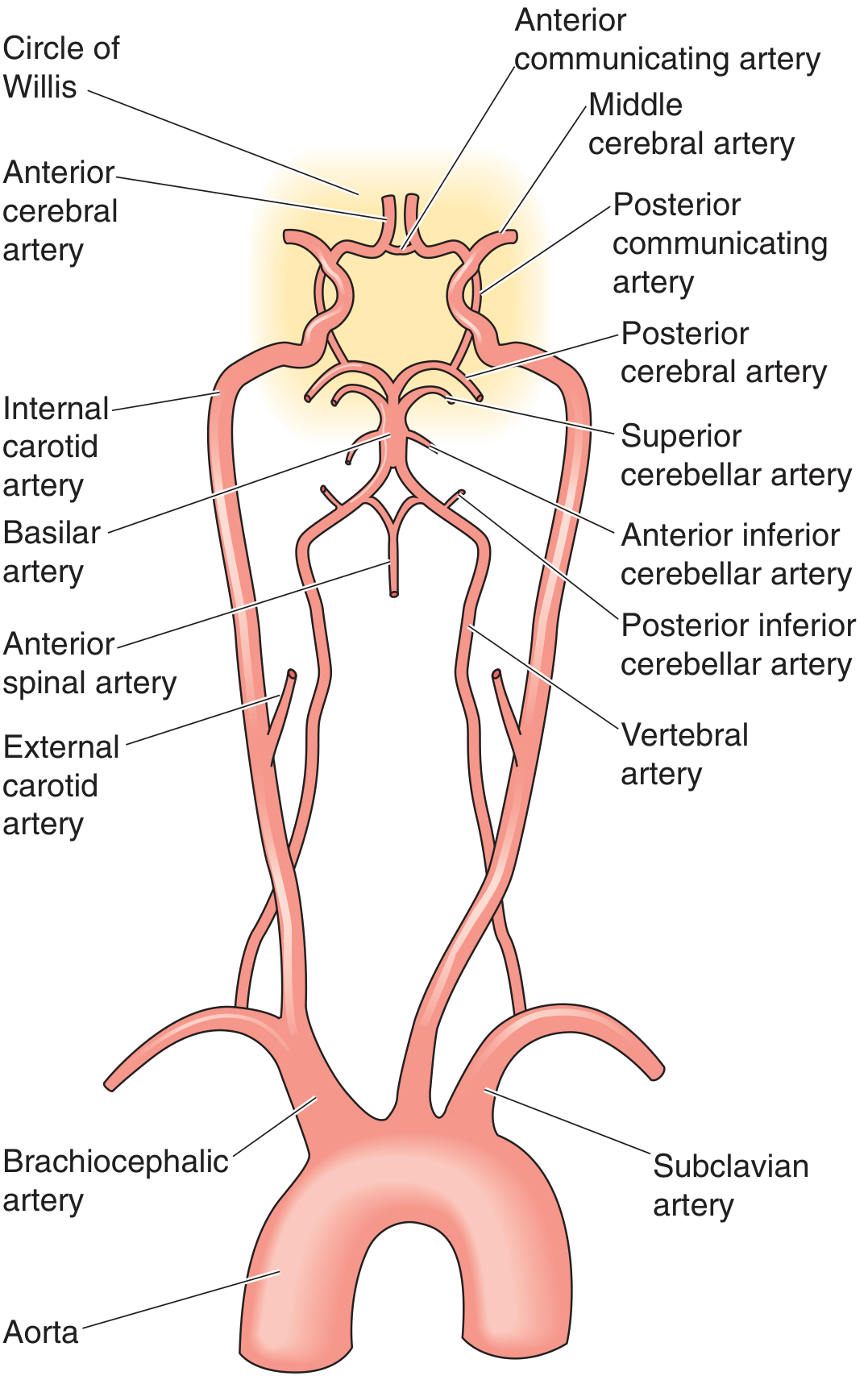
The Circle of Willis (circulus arteriosus cerebri) is an anastomotic arterial ring located at the base of the brain, below the hypothalamus, in the interpeduncular cistern. It connects the anterior circulation (internal carotid arteries) with the posterior circulation (vertebrobasilar system) and provides collateral pathways if any one vessel is occluded.
"In persons with an intact circle of Willis, the entire intracranial circulation can be supplied by a single patent internal carotid artery or vertebral artery."
- Goldman-Cecil Medicine
Anatomy and Components
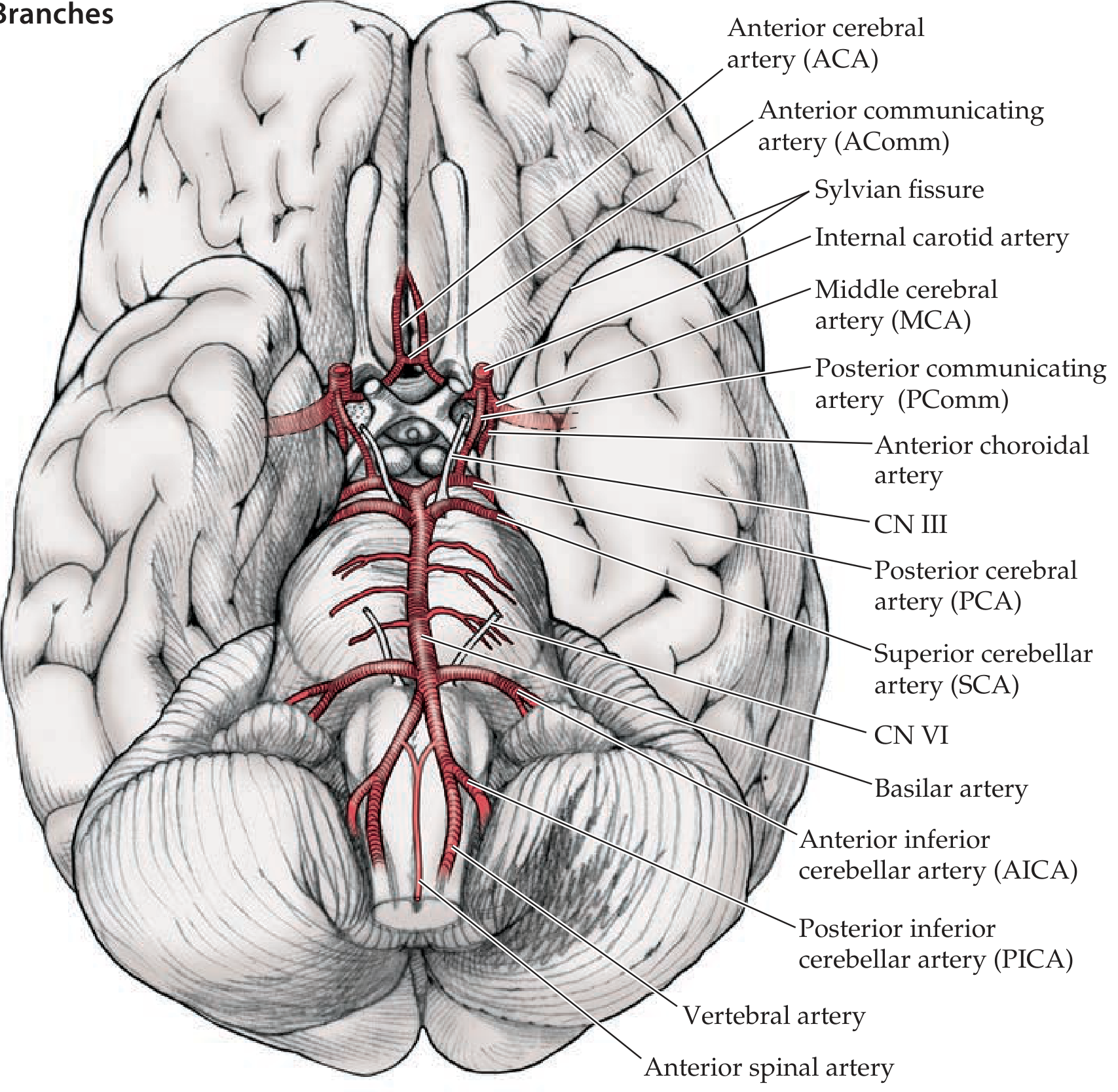
The ring is formed by seven vessels joined by two communicating arteries:
| Component | Origin | Role |
|---|---|---|
| Anterior cerebral arteries (ACA) x2 | ICA terminal branches | Supply medial frontal and parietal lobes |
| Anterior communicating artery (AComm) | Connects left and right ACA | Anterior bridge of the ring |
| Internal carotid arteries (ICA) x2 | Common carotid → ICA | Enter ring at supraclinoid segment |
| Posterior communicating arteries (PComm) x2 | ICA → PCA | Link anterior and posterior circulations |
| Posterior cerebral arteries (PCA) x2 | Top of basilar artery | Supply occipital lobes, thalamus |
The basilar artery (formed by union of both vertebral arteries at the pontomedullary junction) feeds into the ring by dividing into the two PCAs and anastomosing with the PComms.
Three Main Cerebral Arteries Arising from the Ring
| Artery | Territory Supplied |
|---|---|
| ACA | Medial frontal and parietal cortex (leg area of motor/sensory strip) |
| MCA | Lateral cortex - face, arm, language (Broca/Wernicke), insula |
| PCA | Occipital lobe (primary visual cortex), inferior temporal lobe, thalamus, midbrain |
The MCAs are direct continuations of the ICA but are not part of the ring itself - they branch laterally just after the ICA enters the ring.
Anatomical Variations (Very Common)
A complete, full-caliber Circle of Willis is present in only about 25-34% of individuals - Neuroanatomy through Clinical Cases and Localization in Clinical Neurology both cite this. Common variants include:
- Hypoplastic or absent A1 segment (ACA between ICA and AComm) - both ACAs then fed from one ICA
- "Fetal" PCA: P1 segment (between basilar and PComm) is absent/hypoplastic, so the PCA territory is supplied by the carotid rather than the vertebrobasilar system
- Hypoplastic PComm - reduces collateral reserve between anterior and posterior circulations
Because of these variants, collateral flow does not always function as textbooks classically imply. Patients with incomplete rings are at higher risk of infarction when a feeding artery is occluded.
Collateral Circulation
The Circle of Willis is the most important source of intracranial collateral flow. Other collateral sources (ranked by importance) are:
- Circle of Willis - connects carotid and vertebrobasilar systems
- Anastomoses between extracranial and intracranial arteries (e.g., ECA branches to ICA via ophthalmic artery)
- Leptomeningeal anastomoses between ACA, MCA, and PCA territories
- Localization in Clinical Neurology, 8e
Normally, no significant crossing-over of flow occurs between sides because pressure is equal bilaterally (Ganong's). Collateral flow activates only when a pressure differential exists (i.e., stenosis or occlusion).
Clinical Significance
1. Berry (Saccular) Aneurysms
The bifurcation points of the Circle of Willis are the most common sites for saccular aneurysms, which develop due to congenital defects in the vessel media combined with hemodynamic stress at branching points.
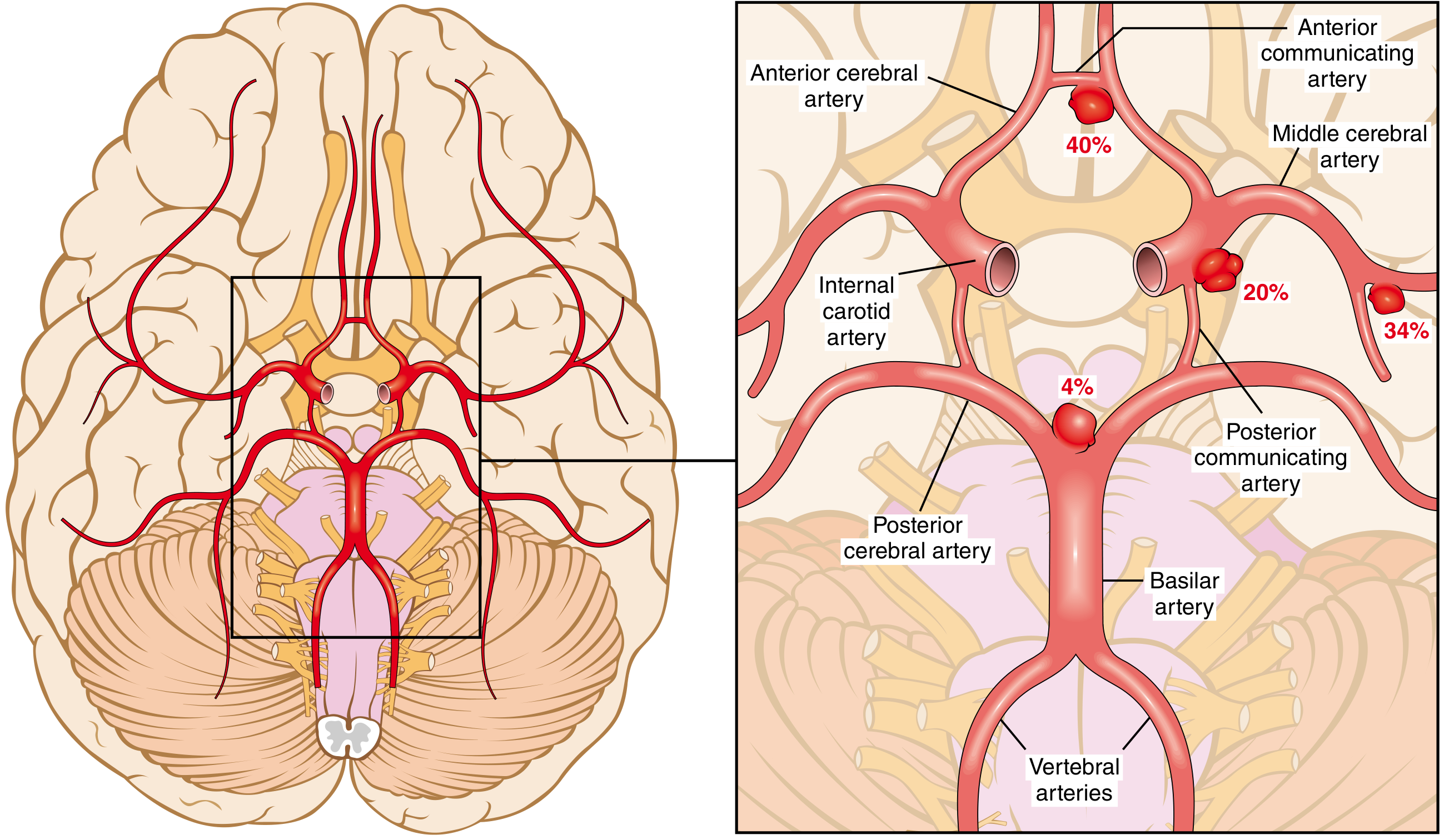
Distribution of aneurysms (from Robbins Pathologic Basis of Disease):
- AComm / ACA junction: ~40% (most common)
- MCA bifurcation: ~34%
- ICA / PComm junction: ~20%
- Basilar tip / PCA: ~4%
Rupture causes subarachnoid hemorrhage (SAH) - classically presenting as "the worst headache of life." Post-rupture vasospasm of circle of Willis vessels is a major cause of delayed ischemic injury.
2. Ischemic Stroke
Large artery occlusions involving the ICA, vertebral artery, basilar artery, or the proximal branches of the circle of Willis are classified as large vessel occlusions - the most amenable to mechanical thrombectomy. An intact circle provides collateral support during acute occlusion.
3. CN III Compression
The PComm artery runs adjacent to CN III (oculomotor nerve). An aneurysm at the ICA-PComm junction can compress CN III, producing a "surgical" third nerve palsy - painful, with pupil dilation (mydriasis), loss of elevation, and ptosis.
4. Watershed Infarcts
When perfusion pressure drops globally (e.g., cardiac arrest, severe hypotension), infarcts occur at the border zones between ACA-MCA and MCA-PCA territories - the furthest points from the circle of Willis.
5. Carotid Stenosis / Occlusion
Occlusion proximal to the circle of Willis (e.g., ICA stenosis) may be asymptomatic if the contralateral ICA and vertebrobasilar system can supply the deficit via the ring. This accounts for the variable presentation of carotid disease. - Schwartz's Principles of Surgery
Key Mnemonic
"2 ACAs + AComm + 2 ICAs + 2 PComms + 2 PCAs + basilar" = the ring
A handy way to remember the anterior vs. posterior contributions:
- Anterior half: 2 ACA + AComm (both from ICA)
- Posterior half: 2 PCA + 2 PComm (PCA from basilar, PComm bridges to ICA)
Sources: Goldman-Cecil Medicine | Neuroanatomy through Clinical Cases, 3e | Robbins Pathologic Basis of Disease | Localization in Clinical Neurology, 8e | Ganong's Review of Medical Physiology | Barash Clinical Anesthesia, 9e | Schwartz's Principles of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.