Viral hepatitis mbbs 2nd proff
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have all the key content and images. Let me compile the comprehensive MBBS 2nd year notes on Viral Hepatitis.
Viral Hepatitis - MBBS 2nd Year (Pathology)
Source: Robbins & Kumar Basic Pathology, 10th Edition
Overview
Viral hepatitis refers to liver inflammation caused by hepatotropic viruses (HAV, HBV, HCV, HDV, HEV). The same word "hepatitis" also describes liver injury from EBV, CMV, autoimmune reactions, drugs, and toxins - but the hepatotropic viruses are the primary concern here.
Comparison Table - The Five Hepatitis Viruses
| Feature | HAV | HBV | HCV | HDV | HEV |
|---|---|---|---|---|---|
| Genome | ssRNA | Partially dsDNA | ssRNA | Circular defective ssRNA | ssRNA |
| Family | Hepatovirus (Picornavirus) | Hepadnaviridae | Flaviviridae | Deltaviridae | Hepeviridae |
| Transmission | Fecal-oral | Parenteral, sexual, perinatal | Parenteral | Parenteral | Fecal-oral |
| Incubation | 2-6 weeks | 2-26 weeks (mean 8 wks) | 4-26 weeks (mean 9 wks) | Same as HBV | 4-5 weeks |
| Chronic disease | Never | 5%-10% | >80% | 10% (coinfection); 90-100% (superinfection) | Only in immunocompromised |
| Fulminant hepatitis | 0.1% | 0.1%-0.5% | Rare | Higher risk | High in pregnant women (~20% mortality) |
1. Hepatitis A Virus (HAV)
Virology: Nonenveloped, positive-strand RNA picornavirus (genus Hepatovirus). Shed in stool 2-3 weeks before and 1 week after onset of jaundice.
Epidemiology: Endemic in countries with poor healthcare infrastructure. Accounts for ~25% of acute hepatitis worldwide.
Transmission: Fecal-oral (contaminated water/food), shellfish consumption, infected food handlers.
Key Features:
- Incubation: 2-6 weeks
- Self-limited; does NOT cause chronic hepatitis
- Does NOT establish a carrier state (viremia is transient)
- Rarely (<0.1%) produces fulminant hepatitis
- Hepatocellular injury is immune-mediated, predominantly by cytotoxic CD8+ T cells (HAV is not directly cytopathic)
Serology (very high-yield):
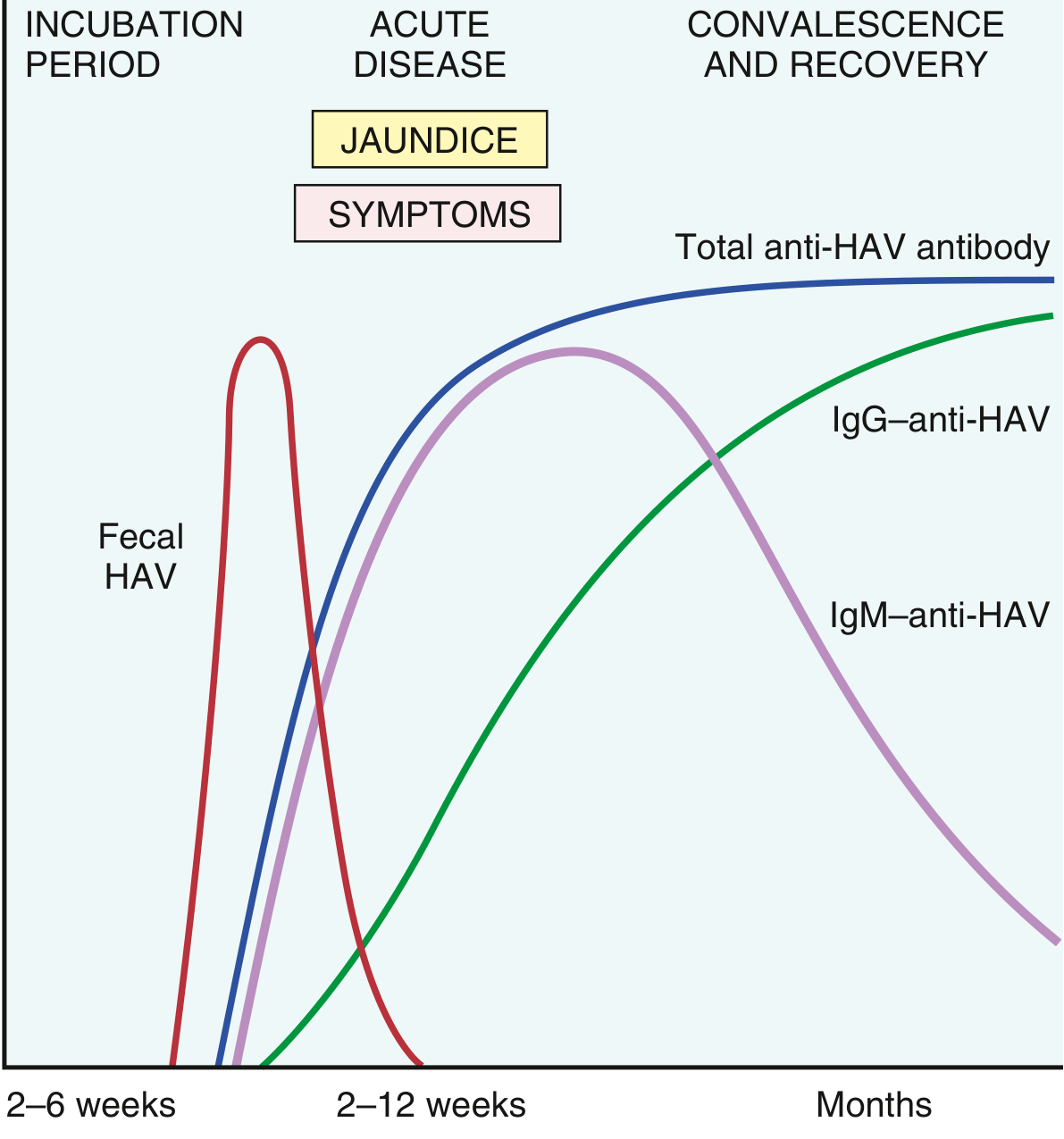
FIG: Serologic markers in acute HAV infection. IgM anti-HAV = acute infection marker. IgG anti-HAV = lifelong immunity.
- IgM anti-HAV = marker of acute infection; appears at symptom onset, declines in a few months
- IgG anti-HAV = appears during convalescence; persists for years (lifelong immunity)
- Blood not screened (viremia transient)
- Vaccine available since 1995; has reduced HAV rates by >95%
2. Hepatitis B Virus (HBV)
Virology: Member of Hepadnaviridae. Partially double-stranded circular DNA (~3200 nucleotides). Unique replication: DNA → RNA → DNA via reverse transcriptase.
Four HBV Proteins/Antigens:
- HBcAg (core antigen) - stays in hepatocytes; participates in virion assembly
- HBeAg (e antigen) - secreted into blood; marker of active replication
- HBsAg (surface antigen) - envelope glycoprotein; secreted in massive quantities; basis of the vaccine
- HBx protein - transcriptional transactivator; implicated in hepatocellular carcinoma pathogenesis
Epidemiology: 2 billion people infected; 250 million chronic carriers. Predominantly in Asia and Western Pacific rim.
Transmission varies by prevalence:
- High-prevalence areas: perinatal (accounts for 90% of cases)
- Intermediate prevalence: horizontal transmission in early childhood
- Low-prevalence areas: unprotected sex, IV drug use
Outcomes of Acute HBV Infection (Fig. 14.9):
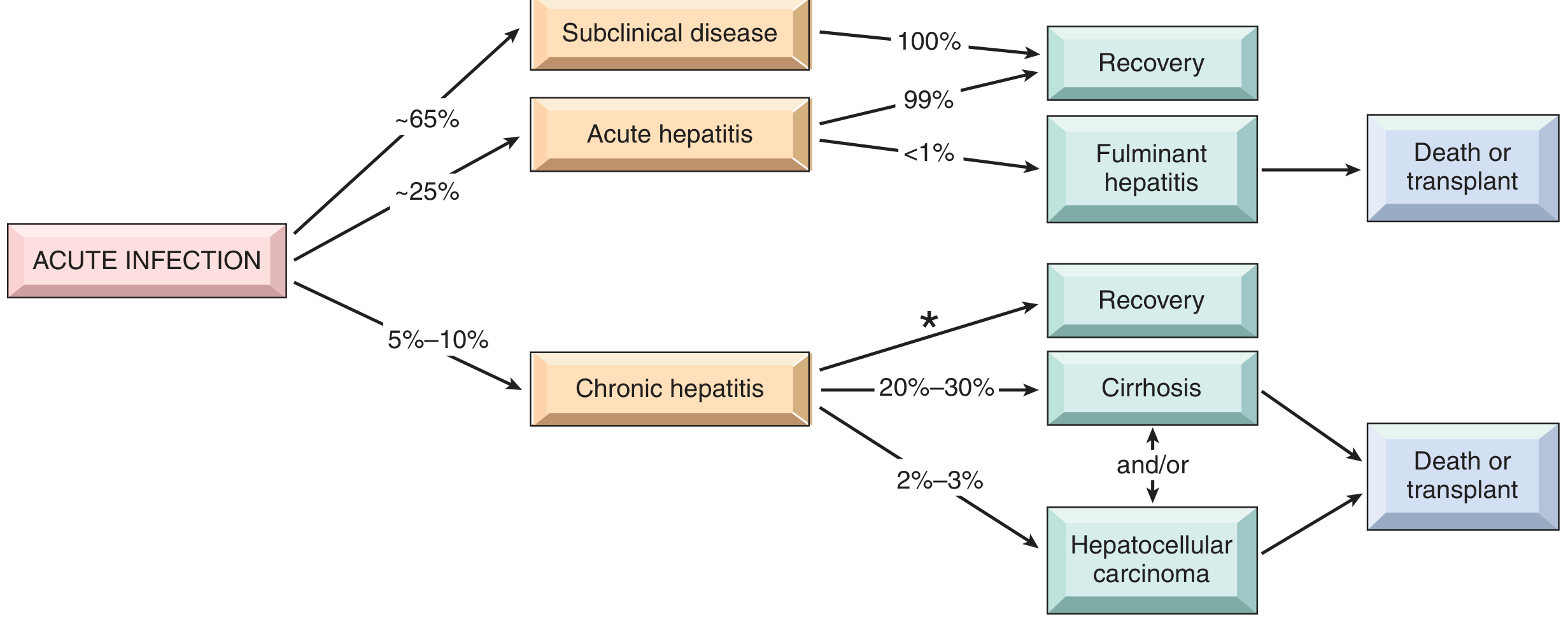
FIG: Potential outcomes of HBV infection. Note that ~65% of adults have subclinical/anicteric disease.
- Acute hepatitis with recovery (most common in adults)
- Nonprogressive chronic hepatitis
- Progressive chronic disease → cirrhosis
- Fulminant hepatitis with massive liver necrosis
- Asymptomatic "healthy" carrier state
Risk of chronic infection is inversely related to age at infection:
- Neonates: >90% become chronic carriers
- Children: ~30%
- Adults: only 5%-10%
HBV Serology (HIGH-YIELD):
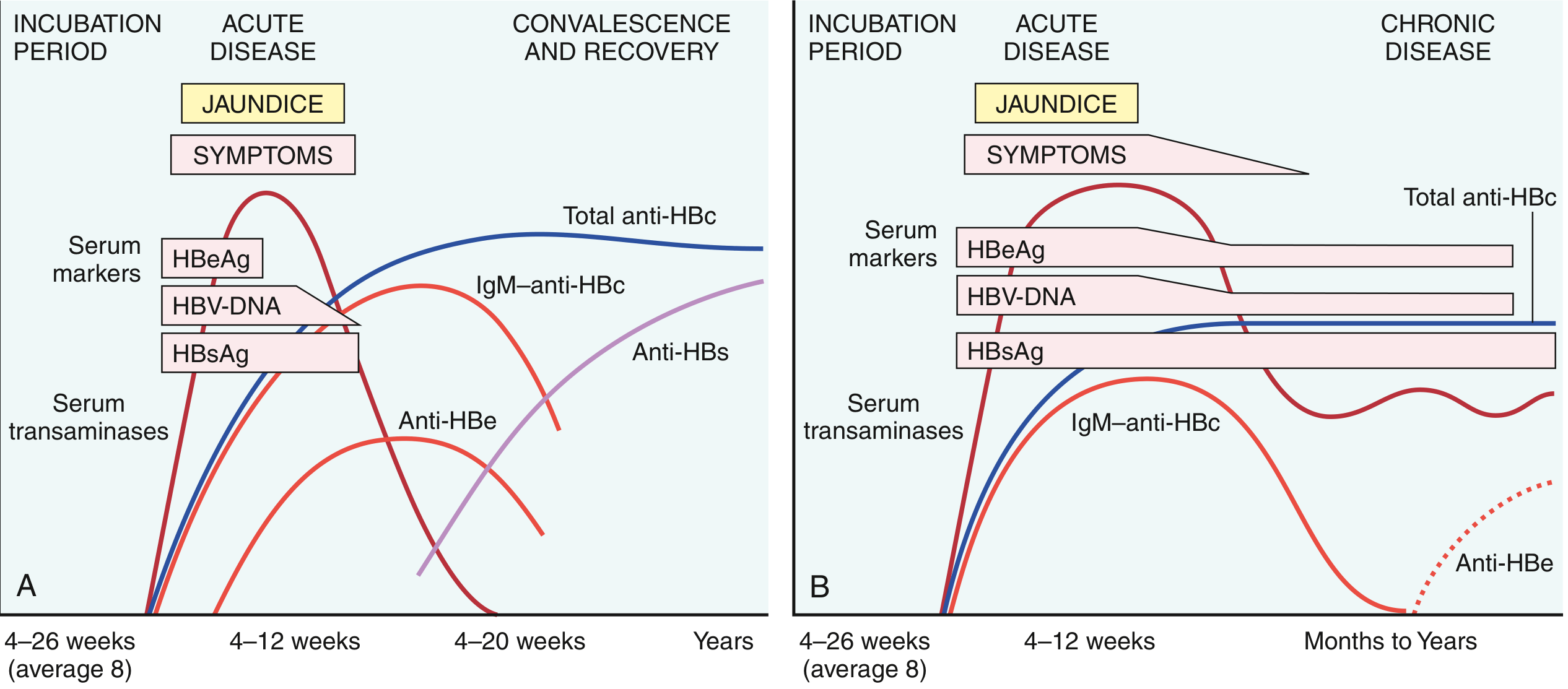
FIG: HBV serologic markers. (A) Acute resolving infection. (B) Chronic infection.
| Marker | Interpretation |
|---|---|
| HBsAg | First marker to appear; persists in chronic infection; basis of screening |
| Anti-HBs | Appears after acute disease resolves; confers protection (also seen after vaccination); NOT produced in chronic infection |
| HBeAg | Marker of active viral replication and high infectivity |
| Anti-HBe | Implies acute infection is peaking/waning; favorable sign |
| IgM anti-HBc | Reliable marker of recent/acute HBV infection (appears just before symptoms) |
| IgG anti-HBc | Replaces IgM over months; marker of past/chronic infection |
| HBV-DNA | Present with active replication; used to monitor treatment |
| "Window period" | Period when HBsAg has disappeared but Anti-HBs not yet present; IgM anti-HBc is the only marker |
Treatment of chronic HBV: HBV polymerase inhibitors (e.g., tenofovir, entecavir) and IFN-α - slow progression, reduce damage, prevent cirrhosis/cancer, but do not eliminate infection.
3. Hepatitis C Virus (HCV)
Virology: Enveloped, single-stranded RNA virus; Flaviviridae family. Encodes a single polyprotein processed into 10 functional proteins, including:
- A protease (needed for polyprotein processing) - target of direct-acting antivirals
- NS5A (essential for viral assembly)
- RNA polymerase (needed for replication) - target of antivirals
HCV has low-fidelity RNA polymerase → rapid genetic variants → 7 major genotypes worldwide → quasispecies within each host. This explains immune evasion and chronicity.
Epidemiology: ~170 million affected worldwide; 2.7 million Americans with chronic HCV. Most common cause of chronic liver disease. Responsible for ~1/3 of liver cancer cases in the US.
Transmission: Blood-borne. Risk factors: IV drug use (most important currently), needlestick injury, perinatal (~5-6%), sexual intercourse (low efficiency). Transfusion risk is now near zero due to screening.
Key Feature - HIGH RATE OF CHRONICITY:
- ~85% of acute infections are asymptomatic and go unrecognized
- Chronic hepatitis develops in 80%-90% (contrast: only 5-10% with HBV)
- Cirrhosis develops in ~20% over 20-30 years
HCV Serology:
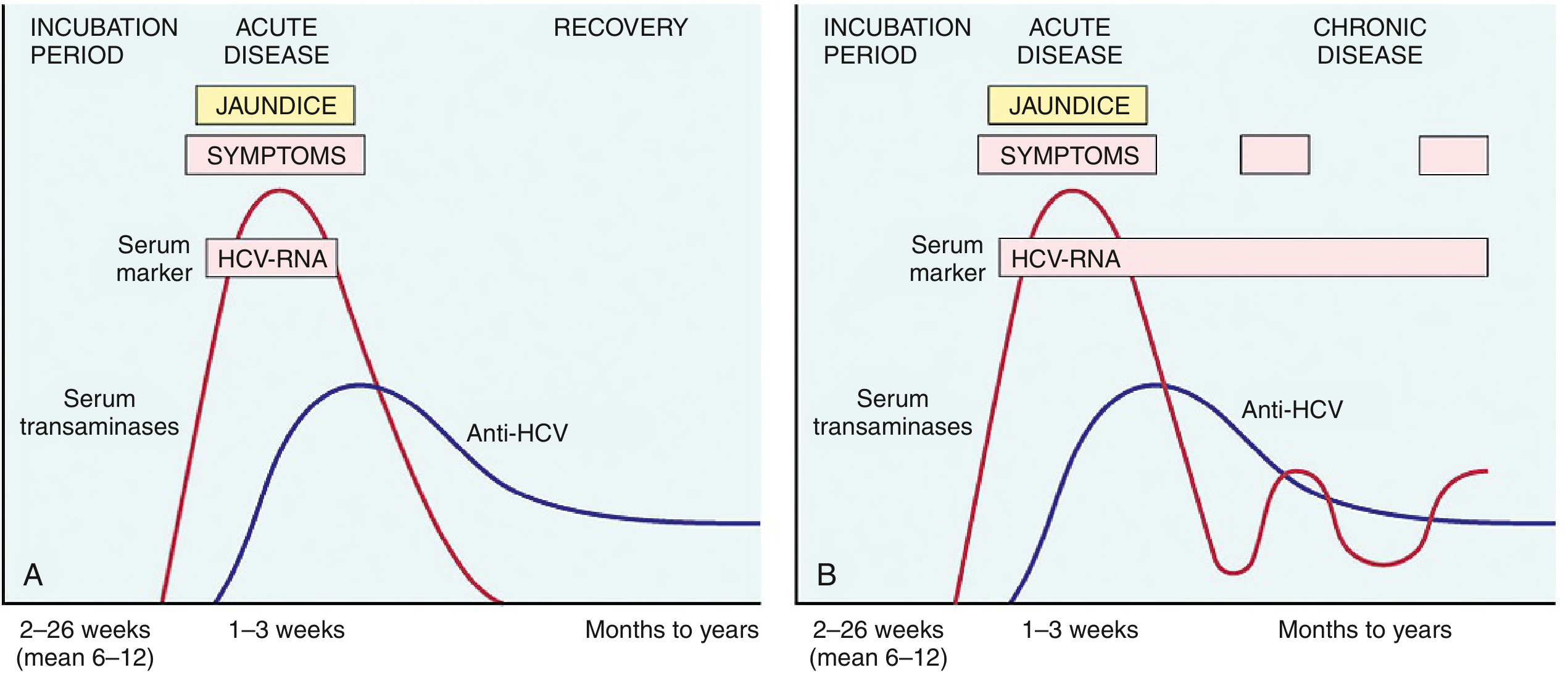
FIG: HCV serologic markers. (A) Acute resolving. (B) Chronic infection.
- HCV RNA detectable 1-3 weeks after exposure (before symptoms)
- Anti-HCV appears later; does NOT confer protection (circulating HCV RNA persists in 90% of patients despite antibody)
- Diagnosis of chronic HCV: confirmed by HCV RNA PCR (not just antibody alone)
- Episodic transaminase elevations with intervening normal periods are characteristic
Treatment: Direct-acting antivirals (DAAs) targeting the viral protease, RNA polymerase, and NS5A. Achieve >95% cure rates. No vaccine available.
4. Hepatitis D Virus (HDV)
- Also called delta agent - a defective RNA virus that requires HBV for its life cycle (uses HBsAg as its envelope)
- Circular defective ssRNA; classified in Deltaviridae family
- Affects ~15 million people worldwide (5% of HBV carriers)
- Transmission: parenteral (IV drug use, transfusions)
Two Forms of HDV Infection:
| Coinfection | Superinfection | |
|---|---|---|
| Definition | HBV + HDV simultaneously | HDV infects existing HBV carrier |
| Outcome | Usually self-limited; both viruses cleared | Chronic HDV in >80%; severe disease |
| Chronic disease | Low | Very high (>90%) |
| Clinical presentation | Like acute hepatitis B | Severe acute hepatitis or exacerbation of chronic HBV |
Key point: Because HDV depends on HBV, HBV vaccination also prevents HDV infection.
Serology:
- HDV RNA in blood and liver at onset
- IgM anti-HDAg = recent HDV exposure
- In chronic superinfection: HBsAg + IgG/IgM anti-HDV persist
5. Hepatitis E Virus (HEV)
- Enterically transmitted, waterborne infection (like HAV)
- Zoonotic disease - animal reservoirs include monkeys, cats, pigs, dogs
- Incubation: 4-5 weeks
- Epidemics in Asia, Indian subcontinent, sub-Saharan Africa, Mexico
- Accounts for 30%-60% of sporadic acute hepatitis in India
Key Distinguishing Feature (HIGH-YIELD):
- High mortality in pregnant women - approaching 20% (especially 3rd trimester)
- Usually self-limiting; does NOT cause chronic liver disease in immunocompetent hosts
- Can cause chronic infection in immunocompromised patients only
- No specific antiviral treatment; a vaccine exists (licensed in China but not widely elsewhere)
Clinicopathologic Syndromes
-
Acute asymptomatic infection with recovery - identified by elevated transaminases or antiviral antibodies incidentally (common with HAV and HBV in children)
-
Acute symptomatic infection with recovery:
- Incubation → preicteric phase (fever, malaise, nausea, RUQ pain) → icteric phase (jaundice, dark urine, pale stools) → convalescence
- Peak infectivity: last asymptomatic days of incubation + early symptomatic days
-
Acute liver failure (fulminant hepatitis):
- Viral hepatitis = ~10% of cases of acute hepatic failure
- HAV = most common cause worldwide; HBV more common in Asia/Mediterranean
- Defined by massive hepatic necrosis with hepatic encephalopathy
-
Chronic hepatitis: hepatic disease >6 months. Can lead to:
- Cirrhosis
- Portal hypertension
- Hepatocellular carcinoma (especially with HBV and HCV)
- Extrahepatic manifestations: vasculitis, glomerulonephritis (immune complex disease), cryoglobulinemia (~35% of chronic HCV)
-
Carrier state: Individual harbors and can transmit virus without symptoms. HBV acquired in early life (endemic areas): carrier state in >90%.
Morphology (Pathology HIGH-YIELD)
Acute Viral Hepatitis
- Liver may be normal, enlarged (due to inflammation), or shrunken (massive necrosis)
- Microscopically:
- Portal and lobular inflammatory infiltrate: predominantly lymphocytes, plasma cells, eosinophils
- Hepatocyte injury - necrosis or apoptosis
- Councilman bodies / acidophilic bodies - apoptotic hepatocytes (small, densely eosinophilic, often extruded from the plate)
- Ballooning degeneration - swelling of hepatocytes due to hydropic change
- Confluent necrosis → bridging necrosis (connecting portal-portal or portal-central veins) in severe cases → panlobular (panacinar) necrosis in fulminant disease
Chronic Viral Hepatitis
- Defining histologic feature: Dense portal lymphocytic or lymphoplasmacytic inflammation with fibrosis
- Interface activity (piecemeal necrosis): inflammatory cells crossing the limiting plate, injuring periportal hepatocytes
- Fibrosis progression: portal/periportal fibrosis → portal-portal bridging fibrosis → cirrhosis
Virus-Specific Histologic Clues:
Chronic Hepatitis B:
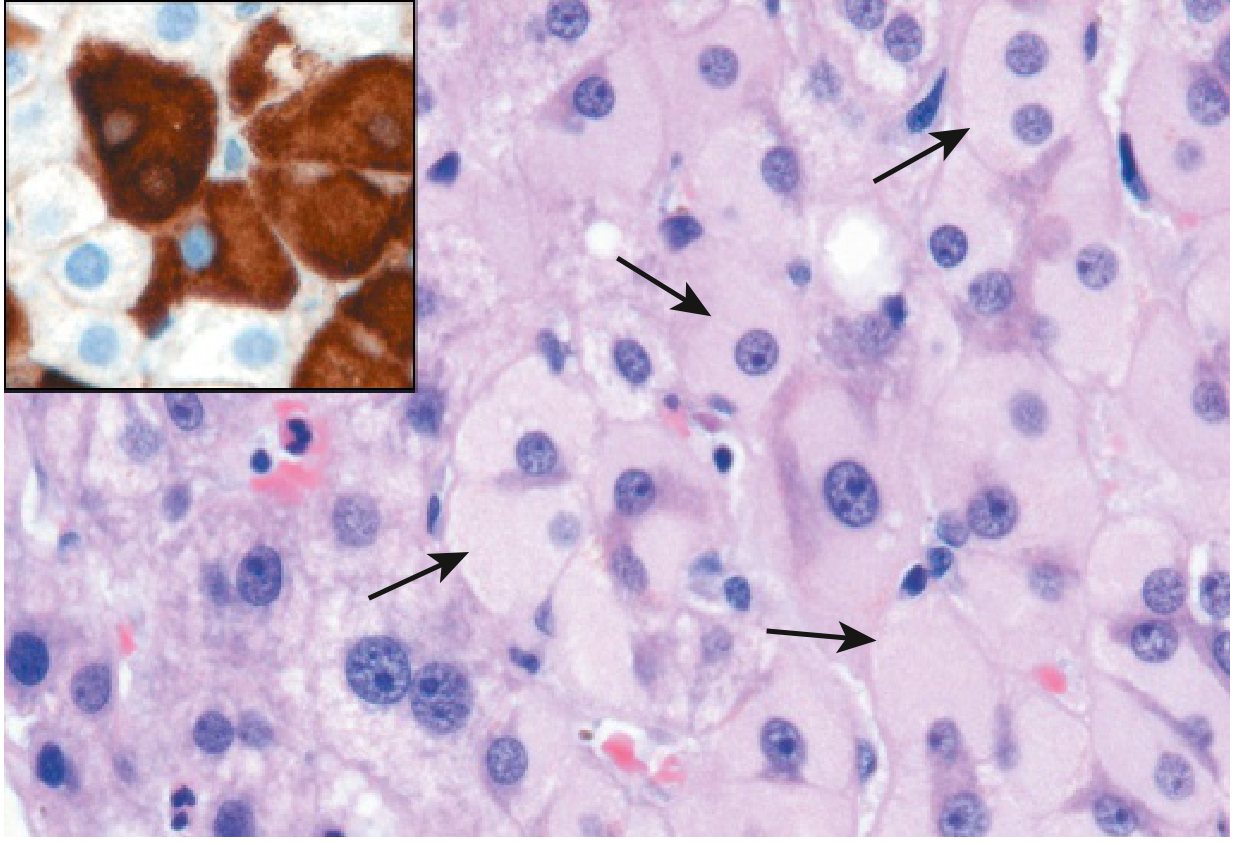
FIG: Ground-glass hepatocytes (arrows) in chronic hepatitis B. Caused by accumulation of HBsAg in the endoplasmic reticulum. Inset: immunostaining confirms HBsAg (brown).
- "Ground-glass" hepatocytes - pale, finely granular eosinophilic cytoplasm due to HBsAg accumulation in ER - DIAGNOSTIC hallmark of chronic HBV
Chronic Hepatitis C:
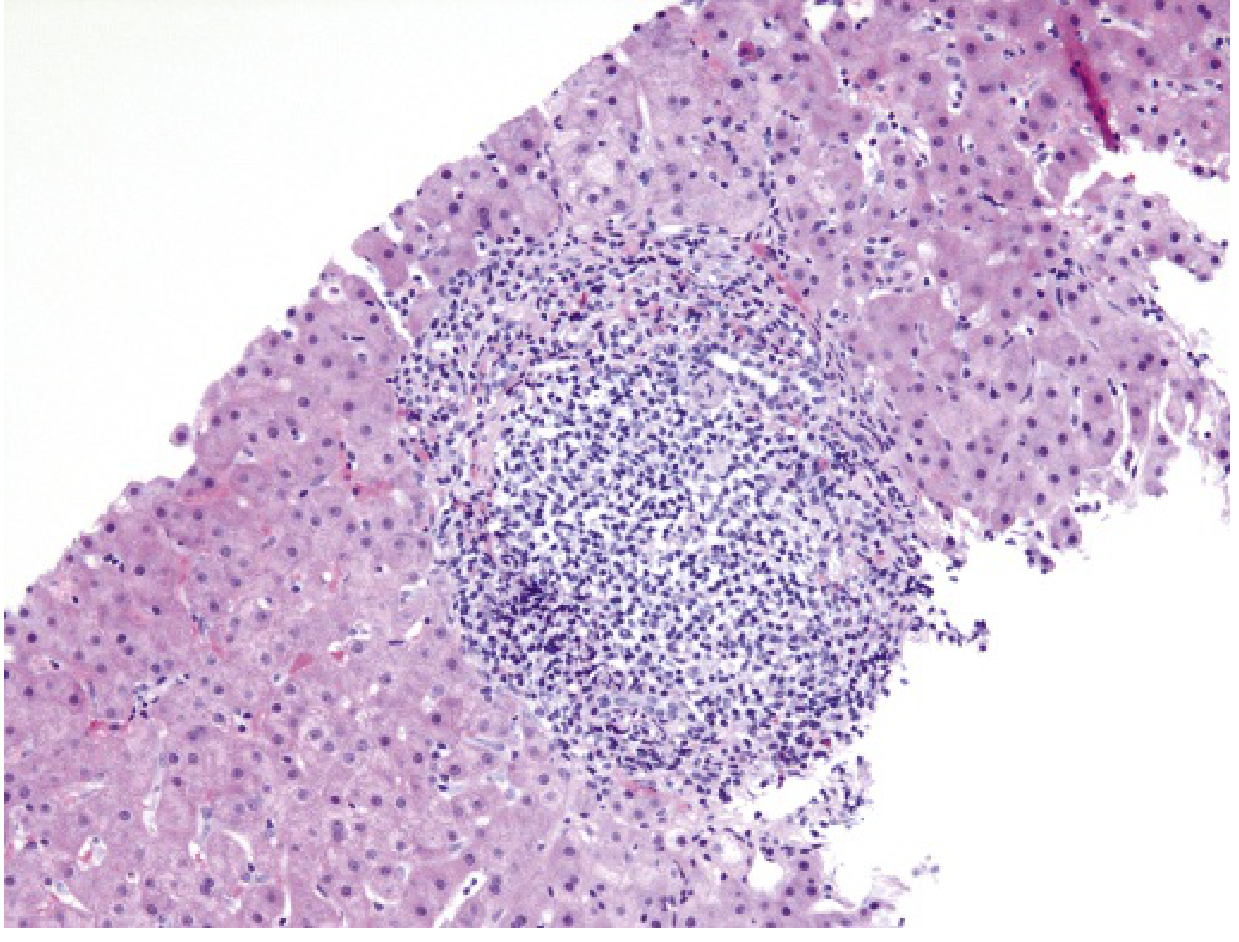
FIG: Chronic HCV - characteristic portal tract expansion by dense lymphoid infiltrate with lymphoid follicle formation.
- Large lymphoid aggregates in portal tracts (lymphoid follicles)
- Fatty change (steatosis) in scattered hepatocytes
- Bile duct injury in some cases (mimics primary biliary cholangitis)
Summary - High-Yield Memory Points for Exams
| Point | Answer |
|---|---|
| Never causes chronic hepatitis | HAV, HEV |
| Highest chronicity rate | HCV (>80%) |
| Dependent on HBV | HDV |
| High mortality in pregnancy | HEV (~20%) |
| Ground-glass hepatocytes | Chronic HBV (HBsAg in ER) |
| Lymphoid follicles in portal tracts | Chronic HCV |
| Marker of acute HAV | IgM anti-HAV |
| Marker of acute HBV | IgM anti-HBc |
| Marker of high HBV infectivity | HBeAg, HBV-DNA |
| "Window period" marker | IgM anti-HBc (only positive marker) |
| Anti-HBs = | Immunity (vaccine or resolved infection) |
| HCV diagnosis confirmed by | HCV RNA PCR |
| HBV replication mechanism | DNA → RNA → DNA (reverse transcriptase) |
| HBx protein | Implicated in HBV-associated HCC |
| Quasispecies concept | HCV - explains immune evasion and chronicity |
Robbins & Kumar Basic Pathology, 10th Edition - Chapter 14: Liver and Gallbladder
This is a shared conversation. Sign in to Orris to start your own chat.