Lab diagnosis of TB refer microbiology book
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from both microbiology textbooks. Let me compile the full answer.
Laboratory Diagnosis of Tuberculosis
Sources: Medical Microbiology 9e (Murray et al.) and Jawetz, Melnick & Adelberg's Medical Microbiology 28e
Overview
A positive tuberculin test alone does not prove active disease - isolation of M. tuberculosis provides definitive proof. Laboratory diagnosis combines immunodiagnostic tests, microscopy, nucleic acid amplification, culture, and identification.
1. Specimens
Specimens include:
- Fresh sputum (early morning, 3 consecutive days)
- Gastric washings (especially in children who cannot expectorate)
- Urine
- Pleural fluid, cerebrospinal fluid (CSF), joint fluid
- Biopsy material
- Blood (for disseminated disease)
Recovery is virtually ensured from early morning sputum collected over 3 consecutive days in patients with cavitary pulmonary disease (up to 10⁸ bacilli/mL).
2. Decontamination and Concentration
Specimens from non-sterile sites (e.g., sputum) are treated with N-acetyl-L-cysteine (NALC) to liquefy mucus and NaOH (2% sodium hydroxide) to decontaminate - this kills most other bacteria and fungi while mycobacteria tolerate brief alkali exposure. The specimen is then neutralized with buffer and centrifuged. This selective decontamination is not performed for normally sterile specimens (CSF, pleural fluid).
3. Immunodiagnosis
A. Tuberculin Skin Test (TST / Mantoux / PPD Test)
- Principle: Intradermal injection of 5 tuberculin units of Purified Protein Derivative (PPD); read at 48-72 hours
- A positive reaction (induration) develops 3-4 weeks after exposure to M. tuberculosis
- Indicates past infection or exposure - does NOT imply active disease or immunity
- Limitations:
- False negative in anergic/immunocompromised patients (especially HIV+)
- False positive in BCG-vaccinated individuals (though generally low level)
- Positive in NTM infection
B. Interferon-Gamma Release Assays (IGRAs)
IGRAs measure IFN-γ produced by sensitized CD4+ T cells when stimulated by M. tuberculosis-specific antigens:
- ESAT-6 (early secretory antigenic target-6)
- CFP-10 (culture filtrate protein-10)
- TB7.7 (used in QuantiFERON)
These antigens are absent from BCG strains and most NTM, making IGRAs more specific than PPD.
Two FDA-cleared commercial assays:
| Assay | Method |
|---|---|
| QuantiFERON-TB Gold In-Tube (QFT-GIT) | ELISA on whole blood |
| T-SPOT.TB | ELISPOT on PBMCs |
- Results: Positive / Negative / Indeterminate
- Advantage: Not affected by prior BCG vaccination; single visit
- Limitations: Not recommended in severely immunocompromised patients or children <5 years
4. Microscopy (Smear Examination)
The most rapid method to confirm mycobacterial disease. Three standard stains are used:
| Stain | Method | Appearance |
|---|---|---|
| Ziehl-Neelsen (ZN) | Hot acid-fast (carbolfuchsin + heat + acid-alcohol decolorization) | Bright red/pink rods on blue background |
| Kinyoun | Cold acid-fast (no heat required) | Same as ZN |
| Auramine-Rhodamine (Truant fluorochrome) | Fluorescent dye + acid-alcohol | Yellow-orange fluorescent rods on dark/green background |
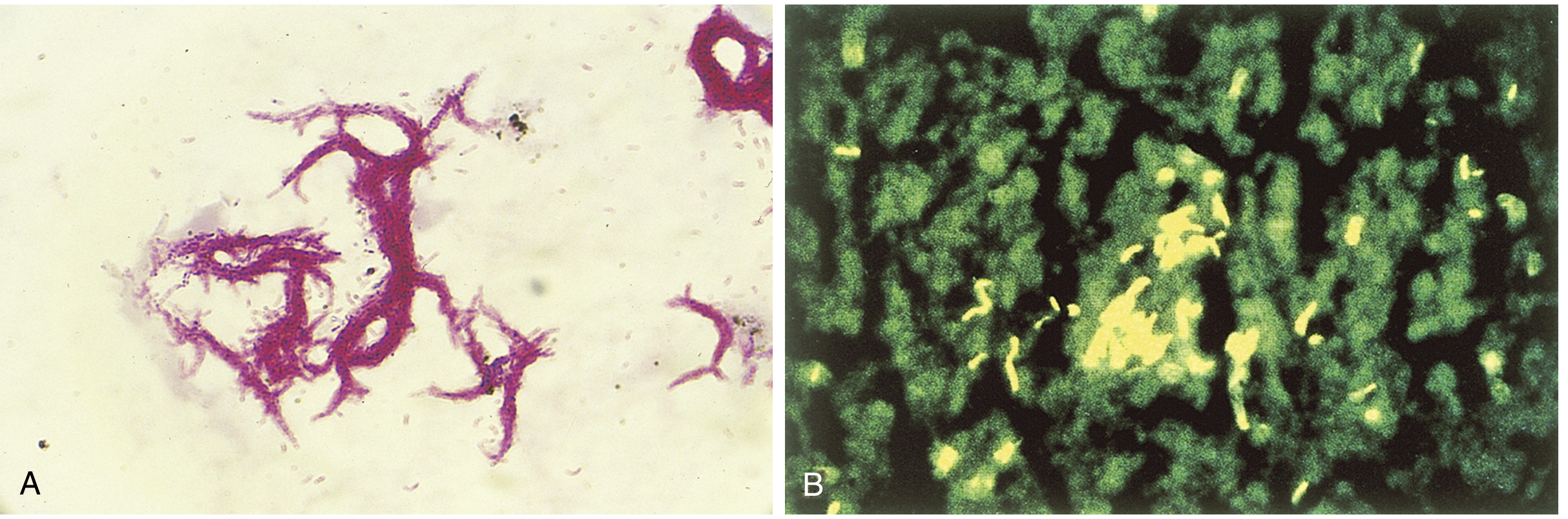
Fig. 22.5 Acid-fast stains of M. tuberculosis. (A) Kinyoun (cold acid-fast) stain showing serpentine cord formation. (B) Auramine-rhodamine fluorochrome stain - preferred for clinical specimens due to higher sensitivity. (From Medical Microbiology 9e)
Key points:
- Fluorochrome stain is the most sensitive - specimen can be scanned under low magnification and confirmed at high power; it is the preferred method for clinical specimens
- Sensitivity ~50% in culture-positive specimens (higher with cavitary disease)
- Specificity >95% when performed carefully
- A positive AFB smear = presumptive evidence only (cannot distinguish species); culture confirmation required
- Gastric washings and urine smears are generally not recommended alone due to saprophytic mycobacteria
- Note: M. tuberculosis forms characteristic "serpentine cords" - acid-fast bacilli arranged in parallel chains (correlated with virulence via "cord factor" - trehalose-6,6'-dimycolate)
5. Nucleic Acid Amplification Tests (NAATs)
NAATs are now the diagnostic test of choice for rapid detection and have largely transformed TB diagnosis.
Key features:
- Direct detection of M. tuberculosis in clinical specimens
- Results available within hours
- Can simultaneously detect rifampin resistance genes
GeneXpert MTB/RIF (Cepheid) - the most widely used NAAT:
- Real-time multiplex PCR
- Detects M. tuberculosis complex AND rpoB mutations (rifampin resistance)
- Sensitivity: 98.2% for smear-positive specimens; 72.5% for smear-negative specimens
- Specificity: 99.2%
- WHO strongly recommends as initial test in high-burden countries
Whole Genome Sequencing (WGS):
- Emerging approach for comprehensive resistance gene detection
- Goal: replace need for culture-based susceptibility testing
- Used to select therapy and identify resistance genes comprehensively
NAATs do NOT detect NTM (non-tuberculous mycobacteria), so supplementary tests are needed where NTM are common.
6. Culture
Culture is the gold standard - provides definitive diagnosis plus allows susceptibility testing and identification.
Media Types
| Media | Examples | Characteristics |
|---|---|---|
| Egg-based (solid) | Löwenstein-Jensen (LJ) | Traditional; good for colony morphology |
| Agar-based (solid) | Middlebrook 7H10, 7H11 | Defined salts, vitamins, oleic acid, albumin; 7H11 contains casein hydrolysate |
| Broth-based (liquid) | Middlebrook 7H9 broth, MGIT (Mycobacteria Growth Indicator Tube) | Fastest; most sensitive; results ~2 weeks earlier than solid media |
Key culture conditions:
- Incubation at 35-37°C in 5-10% CO₂
- Incubated for up to 8 weeks (solid) or can detect growth earlier in broth
- Selective media include antibiotics to prevent overgrowth of contaminating organisms
- If smear positive but culture negative, or slowly growing NTM suspected: also incubate at 24-33°C for up to 12 weeks
- Both a non-selective and selective medium should be inoculated in parallel
Time to positivity:
- Solid media: usually 4+ weeks for M. tuberculosis
- Broth cultures: approximately 2 weeks earlier than solid media
Colony morphology: M. tuberculosis forms dry, rough, non-pigmented (or light tan), "breadcrumb-like" colonies (buff/cream colored, eugonic).
7. Identification of Isolates
Once growth is detected, the isolate must be identified to species level.
A. Traditional/Conventional Methods (largely historical now)
- Growth rate: Slow growers (>7 days) vs. rapid growers (≤7 days)
- Pigmentation (Runyon classification):
- Photochromogens: pigment produced in light (e.g., M. kansasii)
- Scotochromogens: pigment in dark (e.g., M. scrofulaceum)
- Nonchromogens: no pigment (e.g., MAC, M. tuberculosis)
- Rapid growers (e.g., M. fortuitum, M. abscessus)
- Biochemical tests: Require 6-8 weeks; now largely replaced
B. Molecular Probe Methods (rapid - results in 1 day)
DNA probes specific for rRNA sequences, detected by chemiluminescence (AccuProbe system):
- M. tuberculosis complex (M. tuberculosis, M. bovis, M. africanum, M. caprae, M. microti, M. canettii, M. pinnipedii)
- M. avium complex (MAC)
- M. kansasii
- M. gordonae
These four groups account for >95% of clinical isolates in the USA.
C. 16S rRNA Gene Sequencing
Used for species that cannot be identified by DNA probes; can be used for probe-negative isolates.
D. High-Performance Liquid Chromatography (HPLC)
Based on mycolic acid profiles unique to each species; available in reference laboratories.
E. MALDI-TOF Mass Spectrometry
- Results in <1 hour
- Low cost
- Identifies virtually all species of acid-fast organisms
- Likely to become the identification method of choice
F. DNA Fingerprinting / Strain Typing
- Based on restriction fragment length polymorphism (RFLP)
- Used to track transmission chains, analyze outbreaks, and distinguish reactivation from reinfection
8. Antimicrobial Susceptibility Testing (AST)
Required for all M. tuberculosis isolates to detect drug resistance.
- Broth culture (MGIT): Standardized method for first-line drugs; faster
- Agar proportion method: More arduous, reference lab; tests first- and second-line drugs
- MODS assay (Microscopic Observation Drug Susceptibility): Multi-well broth plate + microscopy for "cording"; used mainly in resource-limited countries
- Molecular methods (e.g., GeneXpert) detect resistance genes (rpoB for rifampin, katG/inhA for isoniazid)
Summary Box: Laboratory Diagnosis of Mycobacterial Disease
(Medical Microbiology 9e, Box 22.1)
| Category | Tests |
|---|---|
| Immunodiagnosis | Tuberculin skin test (PPD/Mantoux), IFN-γ release assays (QuantiFERON, T-SPOT) |
| Microscopy | Ziehl-Neelsen stain, Kinyoun stain, Auramine-rhodamine (Truant) fluorochrome stain |
| Nucleic Acid Tests | NAATs (GeneXpert MTB/RIF), Whole genome sequencing |
| Culture | Egg-based (LJ), Agar-based (7H10/7H11), Broth-based (MGIT) |
| Identification | Growth rate/morphology/pigmentation, Biochemical tests, Molecular probes (AccuProbe), 16S rRNA sequencing, HPLC, MALDI-TOF MS |
| Susceptibility Testing | Broth MIC, Agar proportion, MODS assay, Molecular resistance genes |
References:
- Murray PR et al. Medical Microbiology, 9th ed. Chapter 22: Mycobacterium and Related Acid-Fast Bacteria
- Brooks GF et al. Jawetz, Melnick & Adelberg's Medical Microbiology, 28th ed. Chapter 23: Mycobacteria
This is a shared conversation. Sign in to Orris to start your own chat.