Clinical examination of occulumotor, trochlear and abducens nerve
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full clinical answer.
Clinical Examination of the Oculomotor (CN III), Trochlear (CN IV), and Abducens (CN VI) Nerves
Functional Anatomy - Quick Reference
| Nerve | Muscle(s) Innervated | Primary Action(s) |
|---|---|---|
| CN III (Oculomotor) | Superior rectus, inferior rectus, medial rectus, inferior oblique, levator palpebrae superioris + pupil constrictor/ciliary (parasympathetic via EW nucleus) | Elevation, depression, adduction; lid elevation; pupil constriction & accommodation |
| CN IV (Trochlear) | Superior oblique | Depression in adduction (looking down-and-in); intorsion |
| CN VI (Abducens) | Lateral rectus | Abduction (lateral gaze) |
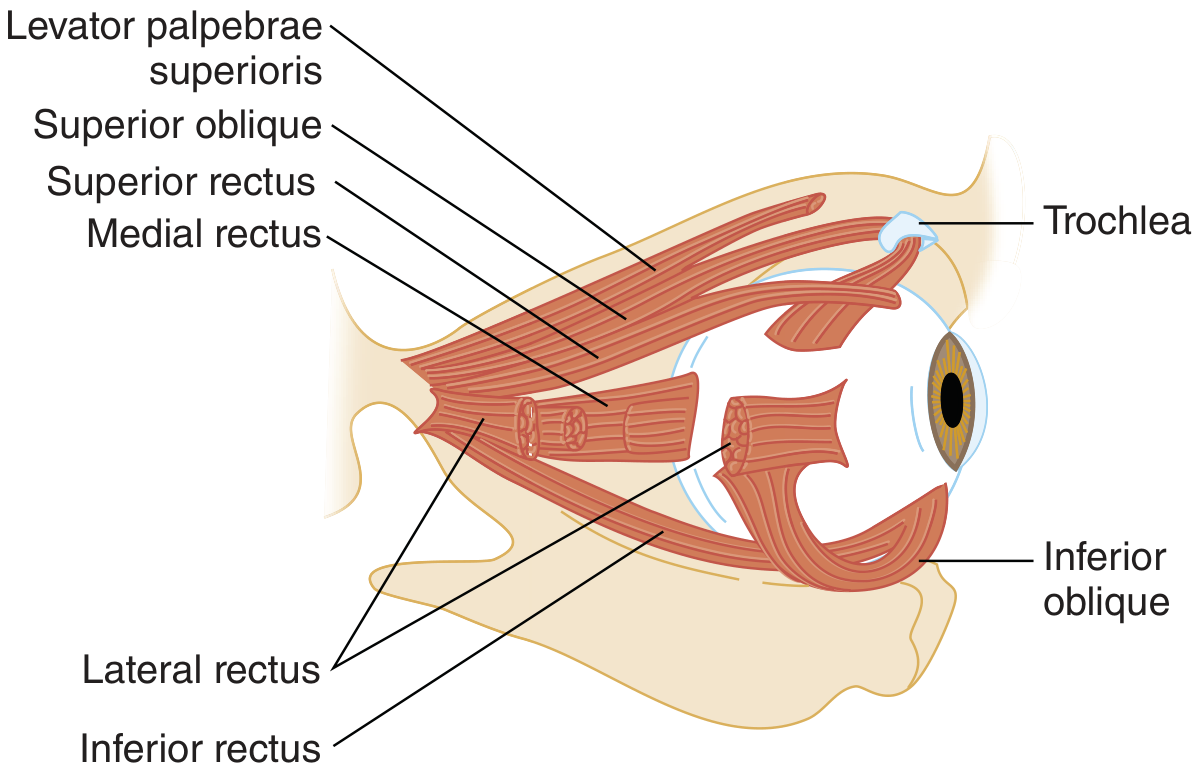
Extraocular muscles and their relationships within the orbit - Tintinalli's Emergency Medicine
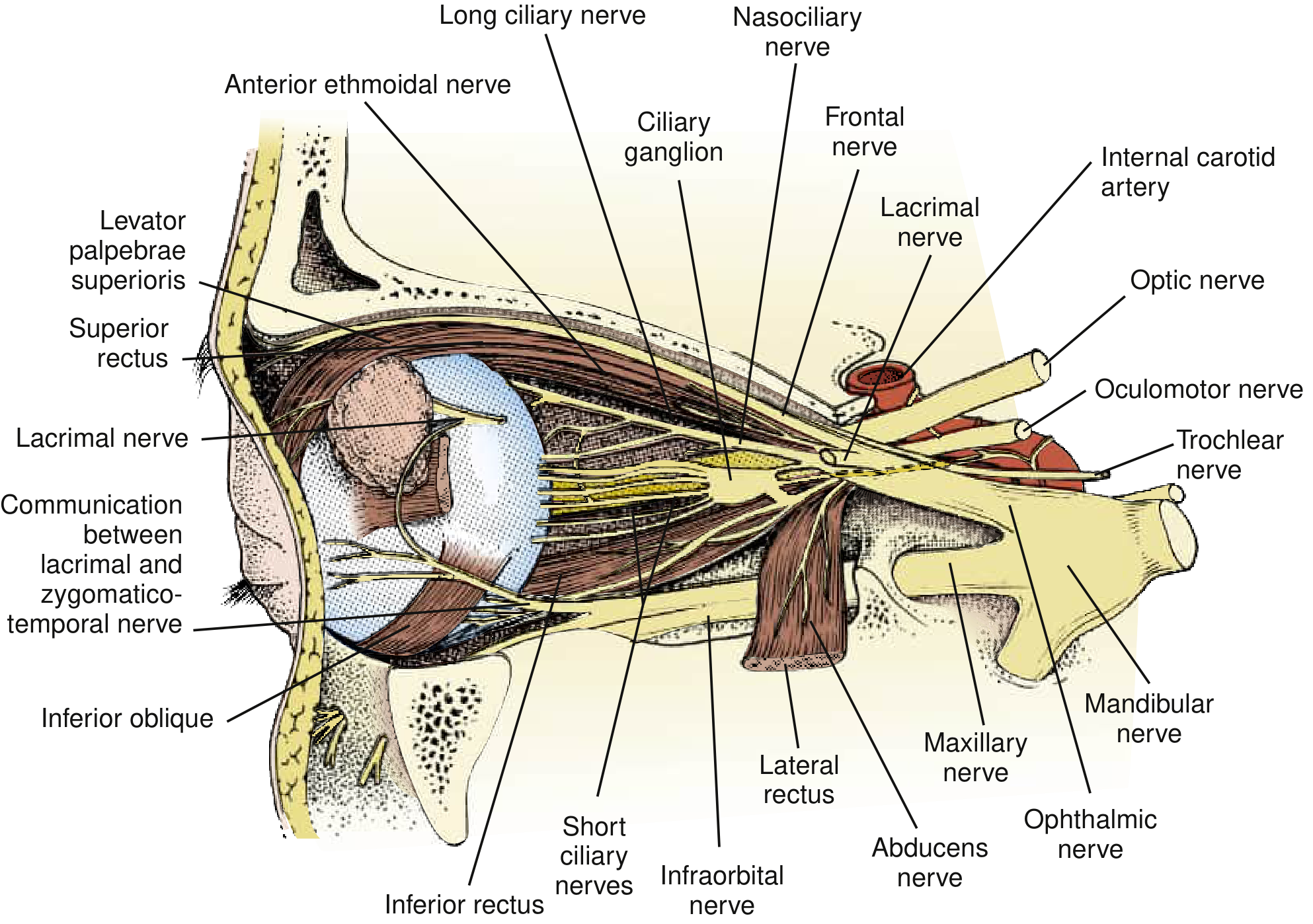
CN III, IV, and VI distributions in the orbital apex - Bradley and Daroff's Neurology in Clinical Practice (from Gray's Anatomy, 39th ed.)
Step-by-Step Clinical Examination
1. Inspect at Rest (Primary Gaze)
- Ptosis: Look for drooping of the upper lid. Partial or complete ptosis points to CN III palsy (levator palpebrae) or sympathetic chain (Horner's - partial ptosis).
- Eye position: Note any resting deviation. A "down and out" eye at rest is the classic position of complete CN III palsy (unopposed CN IV + CN VI action). A medially deviated (esotropic) eye at rest suggests CN VI palsy.
- Head posture: A head tilt away from the affected side (compensatory) suggests CN IV palsy. Ask about old photographs to determine whether the tilt is longstanding (congenital palsy).
2. Pupil Examination
Examine under slightly dim light.
- Size: Measure in mm; compare both eyes. Note anisocoria.
- Direct and consensual light reflex: Shine a light in one eye; look for ipsilateral constriction (direct) and contralateral constriction (consensual). CN III carries the efferent (constrictor) limb.
- Swinging flashlight test: Detects an afferent pupillary defect (CN II problem, not CN III).
- Accommodation reflex: Ask the patient to look at a distant object, then quickly at your finger close up. Expect miosis and convergence. Loss of accommodation (cycloplegia) accompanies CN III palsy.
Key clinical point - pupil involvement in CN III palsy:
- Pupil-involving CN III palsy (dilated, non-reactive pupil): Strongly suggests compressive etiology - posterior communicating artery (PCOM) aneurysm until proven otherwise. Parasympathetic fibers lie superficially on the nerve, making them vulnerable to external compression. Requires urgent neuroimaging + CT/MR angiography.
- Pupil-sparing CN III palsy: More typical of microvascular ischemia (diabetes, hypertension). However, a pupil-sparing incomplete palsy still warrants urgent vascular imaging - some aneurysmal palsies lack pupil involvement initially and progress within 1 week.
- Rule: Any incomplete or pupil-involving CN III palsy = immediate evaluation for PCOM aneurysm. - Bradley and Daroff's Neurology in Clinical Practice
3. Ocular Motility - Six Cardinal Positions of Gaze
Ask the patient to follow your finger or a pen in an "H" or "star" pattern, testing all six positions. Always ask about diplopia - it may be the only subtle sign.
| Direction of Gaze | Muscle Tested | Nerve |
|---|---|---|
| Right | Right lateral rectus | CN VI (right) |
| Left | Left lateral rectus | CN VI (left) |
| Up-right | Right superior rectus | CN III (right) |
| Down-right | Right inferior rectus | CN III (right) |
| Up-left | Left superior rectus | CN III (left) |
| Down-left | Left inferior oblique → but mainly tests superior oblique (down in adduction) | CN IV |
Tip: CN IV is best tested by asking the patient to look down and in (adducted position). The superior oblique depresses the eye in adduction. If the affected eye elevates instead of depressing when adducted, the superior oblique is weak.
- Diplopia assessment: Ask if double vision persists with one eye covered. Binocular diplopia (resolves on cover) = extraocular muscle or nerve pathology. Monocular diplopia = corneal/lens problem or malingering.
- Diplopia from CN VI palsy is horizontal, worst on ipsilateral lateral gaze, and worst at distance.
- Diplopia from CN IV palsy is vertical/oblique, worst going down stairs or reading (down-and-in gaze), worse with ipsilateral head tilt.
- Diplopia from CN III palsy is multidirectional depending on which muscles are affected.
4. Cover and Alternate Cover Tests
Used when a manifest deviation (tropia) or latent deviation (phoria) is suspected, especially to quantify deviation in six cardinal positions.
- Cover-uncover test: Cover one eye; watch the uncovered eye - if it moves to take up fixation, a tropia is present.
- Alternate cover test: Alternately cover each eye rapidly. Allows latent deviations to manifest.
- The higher (hyperdeviated) eye in primary gaze - when uncovered, it moves downward to take fixation, indicating a hypertropia.
5. Park's Three-Step Test (for CN IV/Superior Oblique palsy)
Used specifically to identify which vertically acting muscle is paretic when vertical diplopia is present:
- Step 1: Identify which eye is higher (hypertropic) in primary gaze.
- Step 2: Is the hyperdeviation greater on right gaze or left gaze?
- Step 3: Is the hyperdeviation greater on right head tilt or left head tilt?
A CN IV palsy (superior oblique weakness) gives: hypertropia worse on contralateral gaze and on ipsilateral head tilt (Bielschowsky head tilt test positive). This pattern results from unopposed intortion of the affected eye when tilted toward it.
Bielschowsky head tilt sign: Tilting the head toward the affected shoulder worsens the hypertropia; tilting away relieves it. Patients spontaneously tilt away (compensatory head tilt) to minimize double vision. - Adams and Victor's Principles of Neurology, 12th Edition
In bilateral CN IV palsy (common after head trauma): alternating hyperdeviation depending on gaze direction, "V-pattern" esotropia (eyes cross more on downgaze), and the double Maddox rod test shows total excyclotorsion >10 degrees.
6. Convergence
Ask the patient to follow your finger as it moves from distance toward the bridge of the nose. Normal convergence requires symmetric adduction and pupillary constriction.
- Loss of convergence suggests bilateral CN III involvement or a supranuclear (midbrain) problem.
- Light-near dissociation (pupils react to near but not light) = Parinaud's/dorsal midbrain syndrome or Argyll Robertson pupils.
7. Additional Tests When Indicated
- Double Maddox rod test: For suspected bilateral CN IV palsy or torsional diplopia; excyclotorsion >10 degrees total = bilateral superior oblique paresis.
- Ice test / rest test: If myasthenia gravis is in the differential (fatiguable ptosis and ophthalmoplegia that fluctuates, mimics CN III/IV/VI palsy).
- Prism bar: Measure vertical fusional amplitudes - >6 prism diopters suggests congenital (rather than acquired) CN IV palsy.
Clinical Findings in Palsy of Each Nerve
CN III Palsy - "Down and Out Eye"
- Complete: ptosis, eye deviated down and out, no elevation/depression/adduction, dilated non-reactive pupil (if pupil-involved), loss of accommodation
- Partial: any combination of the above
- Nuclear CN III palsy (rare): bilateral ptosis, contralateral superior rectus weakness (unique cross-innervation anatomy)
Eponymous midbrain syndromes (fascicular CN III palsy + adjacent structure involvement):
- Weber's syndrome: ipsilateral CN III palsy + contralateral hemiparesis (cerebral peduncle)
- Benedikt's syndrome: ipsilateral CN III palsy + contralateral tremor/chorea (red nucleus)
- Claude's syndrome: ipsilateral CN III palsy + contralateral cerebellar ataxia (superior cerebellar peduncle)
- Nothnagel's syndrome: ipsilateral CN III palsy + ipsilateral hemiataxia
Aberrant regeneration (after compressive/traumatic CN III injury): lid elevates on downgaze or adduction; pupil constricts on attempted adduction/elevation/depression. Does NOT occur with microvascular palsy - its presence implies structural injury.
CN IV Palsy - "Can't Read, Can't Go Downstairs"
- Vertical/torsional diplopia; worse going downstairs or reading (downgaze in adduction)
- Compensatory contralateral head tilt
- Bielschowsky sign positive
- Overaction of ipsilateral inferior oblique (excessive elevation on adduction)
- Most common cause of isolated symptomatic vertical diplopia
- Most common cause: congenital, trauma (CN IV decussates in the midbrain - both nerves vulnerable to head trauma), microvascular ischemia
Nuclear CN IV lesion (rare): Causes contralateral (not ipsilateral) superior oblique palsy, so the patient tilts toward the side of the lesion.
CN VI Palsy - "Crossed Eyes Looking to One Side"
- Horizontal diplopia, worst on ipsilateral gaze, worst at distance
- Affected eye fails to abduct; at rest it may be medially deviated (esotropia)
- Patient may compensate with a face turn toward the affected side
- CN VI has the longest intracranial course - prone to raised intracranial pressure (false localizing sign), trauma, and microvascular ischemia
- Bilateral CN VI palsy: raised ICP (e.g., pseudotumor cerebri), Wernicke's encephalopathy, meningitis
Localizing the Lesion
| Location | CN III Signs | Additional Clues |
|---|---|---|
| Nuclear (midbrain) | Bilateral ptosis; contralateral superior rectus weakness | Brainstem signs |
| Fascicular (midbrain) | Ipsilateral CN III palsy | Weber/Benedikt/Claude syndromes |
| Subarachnoid space | Pupil-involving (PCOM aneurysm commonest) | Pain, SAH signs |
| Cavernous sinus | CN III + IV + VI + V1 all affected | Horner's; proptosis |
| Orbital apex | CN III + IV + VI + V1 + CN II | Proptosis, chemosis, visual loss |
| Microvascular (anywhere) | Pupil-sparing (usually) | DM/HTN, older patient, recovers in months |
Summary of Examination Sequence
- Inspection at rest - ptosis, eye position, head tilt
- Pupils - size, direct/consensual reflex, accommodation, swinging flashlight
- Six cardinal positions of gaze - note restricted movement, diplopia
- Cover/alternate cover test - identify and quantify tropia
- Convergence test
- Park's three-step test if vertical diplopia present
- Head tilt test (Bielschowsky) for CN IV palsy
- Maddox rod / double Maddox rod if torsional diplopia suspected
- Ice test / fatigue test if myasthenia gravis in differential
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Adams and Victor's Principles of Neurology, 12th Ed. | Bradley and Daroff's Neurology in Clinical Practice | Tintinalli's Emergency Medicine | Wills Eye Manual | Scott-Brown's Otorhinolaryngology, Vol. 2
This is a shared conversation. Sign in to Orris to start your own chat.