I have heart heavyness, difficulty in breathing, abdominal distention and not having satisfaction after eating stomach full and still hungry.whats the diagnosis
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Now I have solid textbook evidence. Let me compose the full clinical answer.
Your Symptom Cluster - Differential Diagnosis
Your four symptoms together form a very specific and important clinical picture:
| Symptom | Clinical Term |
|---|---|
| Heart heaviness / chest discomfort | Cardiac fullness / palpitation |
| Difficulty breathing | Dyspnea |
| Abdominal distension (bloating, belly swelling) | Abdominal bloating / distension |
| Full stomach yet still hungry / not satisfied | Early satiety + postprandial fullness |
This combination points most strongly toward two main diagnostic possibilities - and they can actually coexist:
Most Likely Diagnosis 1: Congestive Heart Failure (Right-Sided or Biventricular)
This is the most serious possibility and deserves urgent evaluation.
Why it fits your symptoms:
According to Frameworks for Internal Medicine:
"Symptoms of heart failure include dyspnea, cough, orthopnea, paroxysmal nocturnal dyspnea, fatigue, weight gain, nausea, early satiety, and abdominal discomfort."
"Physical findings of right-sided heart failure include elevated JVP, right ventricular heave, ascites, and lower extremity edema."
In right-sided heart failure, blood backs up into the abdomen causing:
- Liver congestion (hepatomegaly) - creates the feeling of upper abdominal fullness
- Ascites (fluid in the belly) - causes abdominal distension
- The swollen, congested liver and gut press on the stomach, causing early satiety (feeling full quickly but not satisfied)
- The failing heart causes dyspnea (difficulty breathing)
- The heart itself can feel heavy, pressure-like, or uncomfortable
Braunwald's Heart Disease confirms: "The usual presentation consists of signs and symptoms of right heart failure, lower extremity edema, vague abdominal complaints, and passive hepatic congestion, which can progress to ascites."
Red flag signs to check: Do you also have swollen legs/ankles, waking up at night breathless, inability to lie flat, or rapid weight gain? These strongly suggest heart failure.
Most Likely Diagnosis 2: Gastroparesis
This is a condition where the stomach empties too slowly (delayed gastric emptying).
Why it fits:
According to Yamada's Textbook of Gastroenterology:
"The clinical presentation of gastroparesis may vary. Symptoms include nausea, vomiting, early satiety, postprandial fullness, and upper abdominal pain. Most patients have nausea and early satiety."
"Women have more severe symptoms of stomach fullness, early satiety, postprandial fullness, bloating, stomach visibly larger, and abdominal pain."
In gastroparesis:
- Food sits in the stomach too long, causing the stomach to look/feel distended
- You feel full quickly but the hunger signal stays because nutrients aren't absorbed normally
- The distended stomach can push upward, pressing on the diaphragm and causing breathing difficulty
- The heaviness you feel around the heart area may actually be referred discomfort from a distended stomach pressing upward
Common causes of gastroparesis include diabetes, post-viral illness, thyroid disease, or it can be idiopathic (no known cause).
Other Possibilities to Consider
| Condition | Why it could fit |
|---|---|
| Functional dyspepsia / Postprandial distress syndrome | Bloating, early satiety, fullness after eating - overlaps significantly with gastroparesis |
| Peptic ulcer disease | Can cause postprandial fullness, early satiety, and abdominal discomfort |
| Ascites from liver disease (cirrhosis) | Abdominal distension + breathlessness from diaphragm elevation |
| Pericardial effusion / Pericarditis | Heart heaviness, breathlessness, with possible abdominal involvement |
What You Should Do - Urgently
Given the combination of heart heaviness + difficulty breathing, this needs prompt medical evaluation. Please see a doctor soon. Tests likely recommended:
- ECG and Echocardiogram - to check heart function and rule out heart failure
- Chest X-ray - to see if there is fluid in the lungs or an enlarged heart
- Blood tests - BNP/NT-proBNP (heart failure marker), liver function, blood sugar (for gastroparesis)
- Abdominal ultrasound - to check for ascites, liver congestion
- Gastric emptying study - if heart cause is ruled out and gastroparesis is suspected
Important: The combination of breathlessness and heart heaviness should never be self-managed. Please visit a physician or emergency department as soon as possible, especially if you also have leg swelling, chest pain, or worsening shortness of breath at rest.
Search for recent heart failure diagnostic guidelines and criteria
Reading File
Searching PubMed
"heart failure"[MeSH Terms] AND "diagnosis"[MeSH Terms] AND "guideline"[pt]
Searching the Web
heart failure diagnostic guidelines criteria 2023 2024 AHA ACC ESC
Finding Sources
Reading Article
PMID: 38466244
Reading Article
PMID: 37117140
Reading Web Page
https://reference.medscape.com/cc1/p10/heart-failure-reduced…
Finding Sources
Searching PubMed
"heart failure"[MeSH Terms] AND "diagnosis" AND "BNP" AND "echocardiography"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I have rich textbook visuals and comprehensive guideline data. Here is the full synthesis:
Heart Failure: Recent Diagnostic Guidelines & Criteria
Key Guideline Sources (2021-2025)
| Guideline | Year | Organization |
|---|---|---|
| ACC/AHA/HFSA Heart Failure Guideline | 2022 | American College of Cardiology / AHA / HFSA |
| ESC Heart Failure Guidelines | 2021 (partial update 2023) | European Society of Cardiology |
| 2024 ACC Expert Consensus Decision Pathway for HFrEF | 2024 | American College of Cardiology [PMID: 38466244] |
| Natriuretic Peptides in HF Diagnosis - Joint ESC/HFSA/JHFS Statement | 2023 | ESC + HFSA + Japanese HF Society [PMID: 37117140] |
An ESC 2026 guideline update is expected to be presented at ESC Congress in August 2026, per Medscape's current HFrEF guidelines overview.
1. Definition of Heart Failure
Heart failure is a clinical syndrome resulting from structural or functional impairment of ventricular filling or ejection of blood. It is diagnosed on the combination of symptoms, signs, and objective evidence of cardiac dysfunction - not any single test.
Fuster and Hurst's The Heart, 15th Ed.: "Cardinal manifestations include dyspnea which may limit exercise tolerance, and fluid retention which may lead to pulmonary, splanchnic and peripheral edema."
2. ACC/AHA 2022 Staging System (A-D)
This replaced the older binary "have HF / don't have HF" model with a progressive 4-stage framework:
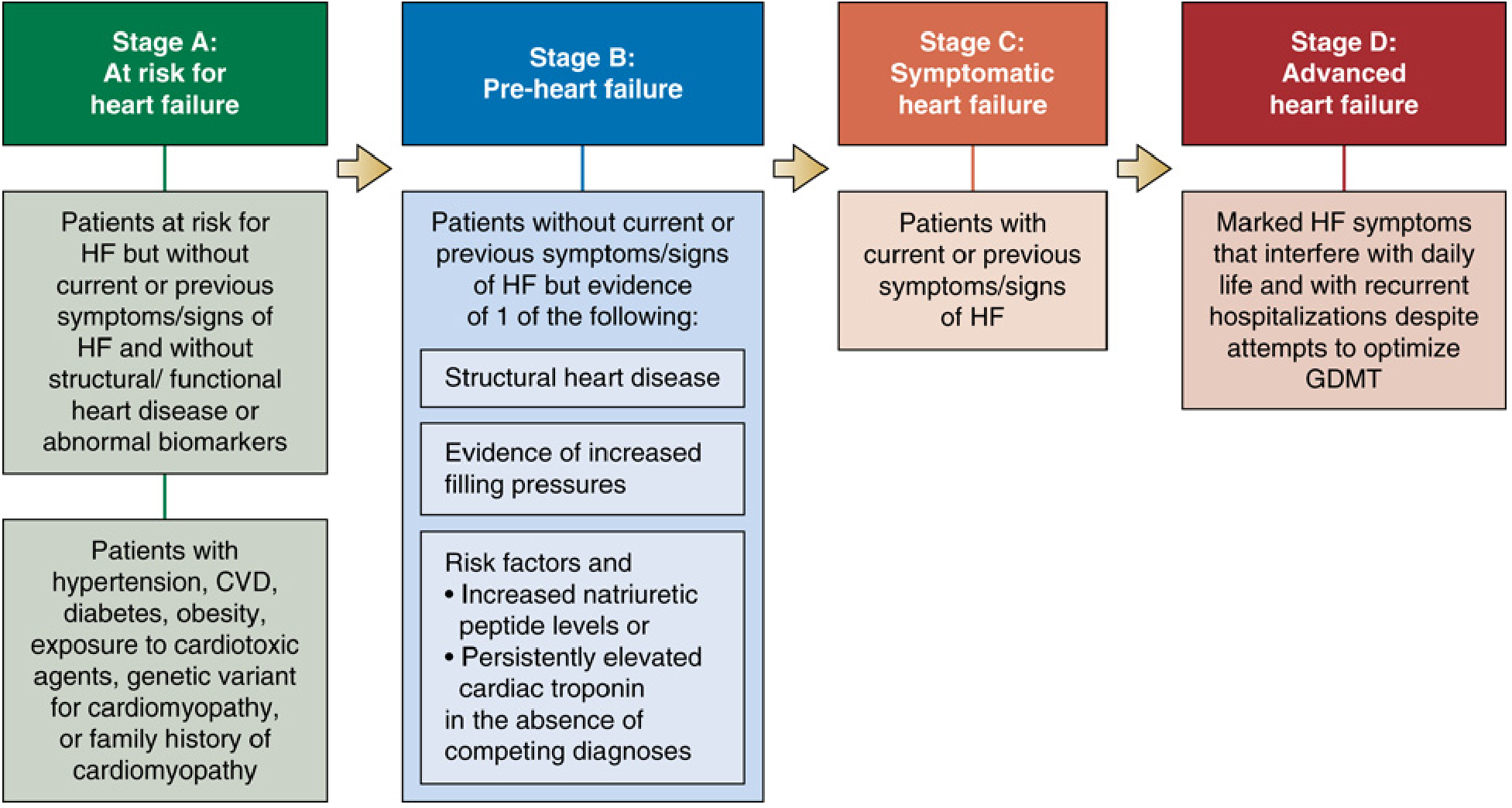
| Stage | Description |
|---|---|
| A | At risk - hypertension, diabetes, obesity, cardiotoxic drugs, family history of cardiomyopathy; NO symptoms or structural disease |
| B | Pre-HF - structural heart disease OR elevated natriuretic peptides OR elevated troponin; NO symptoms |
| C | Symptomatic HF - current or previous symptoms (dyspnea, fatigue, edema) with structural disease |
| D | Advanced HF - marked symptoms at rest, recurrent hospitalizations despite optimized therapy |
3. NYHA Functional Classification (Still Used Alongside Staging)
| Class | Description |
|---|---|
| I | No limitation. Ordinary activity causes no symptoms |
| II | Slight limitation. Ordinary activity causes dyspnea or fatigue |
| III | Marked limitation. Less-than-ordinary activity causes symptoms; comfortable at rest |
| IV | Symptoms at rest; unable to carry on any physical activity |
Fuster and Hurst's The Heart, 15th Ed.: "Patients with NYHA class I have no symptoms attributable to heart disease; those in NYHA classes II, III, or IV have mild, moderate, and severe symptoms, respectively."
4. Classification by Ejection Fraction (LVEF)
The echocardiogram is the cornerstone test for classifying HF type:
| Type | LVEF | Former Term |
|---|---|---|
| HFrEF (reduced EF) | < 40% | Systolic HF |
| HFmrEF (mildly reduced EF) | 40-49% | - |
| HFpEF (preserved EF) | ≥ 50% | Diastolic HF |
| HFrecEF (recovered EF) | Previously reduced, now ≥ 40% | - |
Miller's Anesthesia, 10th Ed.: "HFpEF now accounts for about 50% of the HF population."
5. Diagnostic Criteria & Workup
Step 1 - Clinical Suspicion
Symptoms and signs that raise suspicion:
Symptoms: Dyspnea (exertional or at rest), orthopnea, paroxysmal nocturnal dyspnea, fatigue, ankle swelling, early satiety, nausea, abdominal discomfort
Signs of left-sided HF: Basal crepitations, S3 gallop, laterally displaced apex beat, pulsus alternans
Signs of right-sided HF: Elevated jugular venous pressure (JVP), peripheral edema, ascites, hepatomegaly, right ventricular heave
Step 2 - Biomarkers (BNP/NT-proBNP)
All major guidelines (NICE, ESC, ACC/AHA) recommend natriuretic peptides as first-line biomarkers:
| Biomarker | ESC/ACC/AHA threshold | NICE thresholds |
|---|---|---|
| BNP | > 35 pg/mL (chronic HF) | - |
| NT-proBNP | > 125 pg/mL (chronic HF) | 400-2000 ng/L: refer within 6 weeks; >2000 ng/L: urgent assessment |
The 2023 Joint ESC/HFSA/JHFS Natriuretic Peptide Statement also highlights their role in prognosis and guiding therapy with ARNI agents.
Note: BNP levels can be falsely low in obesity and falsely elevated in renal failure and atrial fibrillation.
Step 3 - Echocardiography (Transthoracic Echo, TTE)
TTE is the primary and initial imaging test recommended by all three major guidelines. It:
- Measures LVEF (using Simpson's biplane method, or 3D echo which is more accurate)
- Identifies structural abnormalities (valvular disease, cardiomyopathy, wall motion)
- Assesses diastolic function and filling pressures
For HFpEF specifically, the 2025 ASE Updated Recommendations on Diastolic Function provide the most current criteria [PMID: 40617625].
Step 4 - Additional Tests
| Test | Purpose |
|---|---|
| ECG | Arrhythmia, ischemia, LVH, bundle branch block |
| Chest X-ray | Cardiomegaly, pulmonary venous congestion, pleural effusion |
| Cardiac MRI | Gold standard for LV function quantification; tissue characterization (fibrosis, infiltration) |
| Troponin | Myocardial injury, risk stratification |
| Blood tests | FBC, renal function, LFTs, TFTs, glucose/HbA1c |
| Cardiopulmonary exercise test | Gold standard for risk stratification pre-transplant |
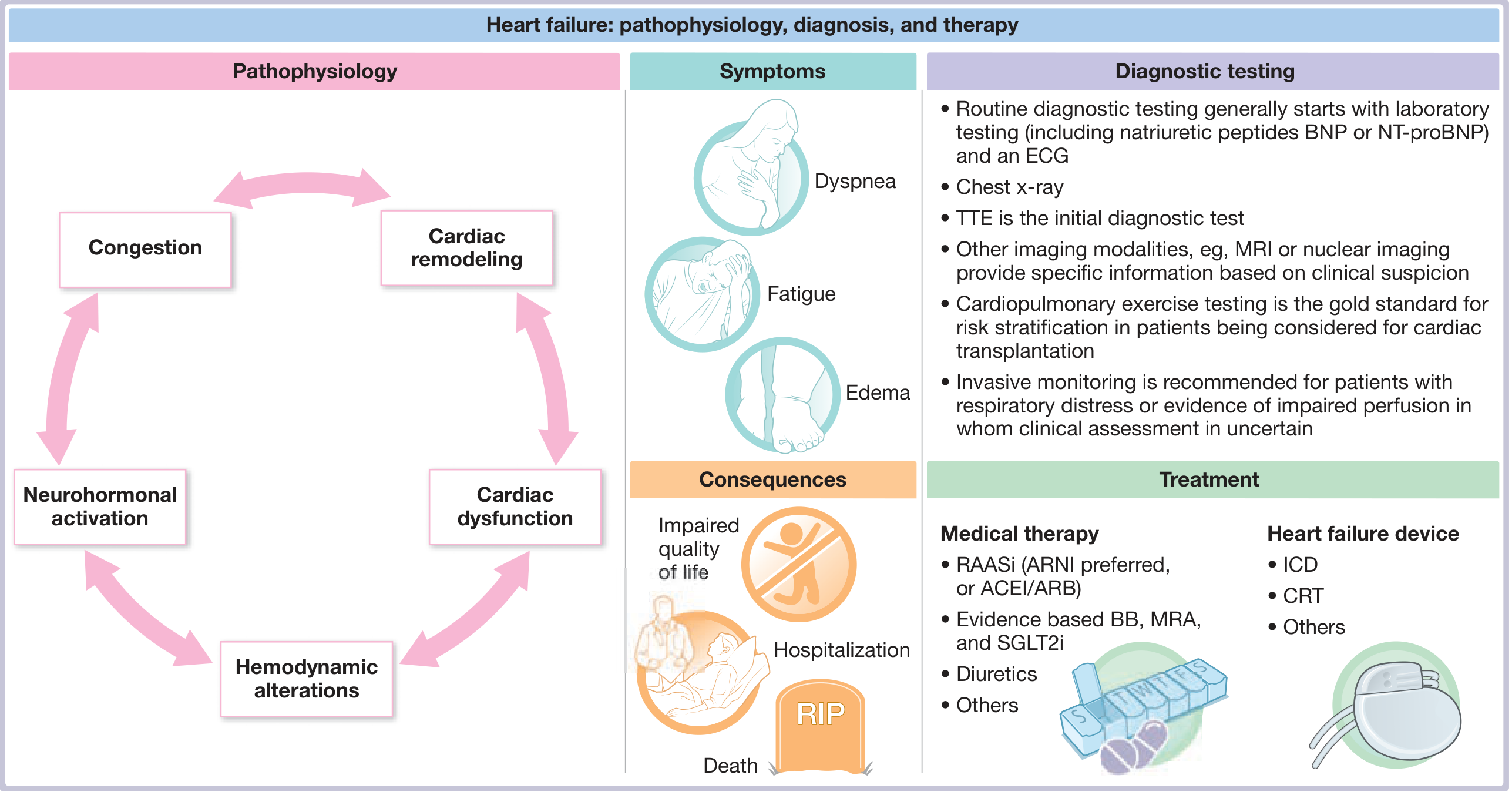
6. Pathophysiology - Diagnosis - Treatment at a Glance
7. Guideline-Directed Medical Therapy (GDMT) for HFrEF
Per the 2024 ACC Decision Pathway for HFrEF, the "Fantastic Four" drug classes are now the foundation of treatment for LVEF < 40%:
- ARNI (sacubitril/valsartan) - or ACEI/ARB if ARNI not tolerated
- Beta-blocker (bisoprolol, carvedilol, or metoprolol succinate)
- MRA (spironolactone or eplerenone)
- SGLT2 inhibitor (dapagliflozin or empagliflozin)
Target or maximally tolerated doses should ideally be reached within 3 months of diagnosis, per the 2024 ACC consensus.
Recent Evidence of Note
- [Systematic Review 2023] Goyder et al. confirmed that natriuretic peptide screening accurately detects left ventricular systolic dysfunction in community settings - supports its use as a first-line diagnostic tool [PMID: 36785511]
- [2025 ASE Guidelines] New ASE recommendations update diastolic function assessment criteria for HFpEF diagnosis [PMID: 40617625]
- [2025 CCS/CHFS Guidelines] Updated pharmacologic management for HF with non-reduced EF (LVEF > 40%) published October 2025 [PMID: 41110921]
This is a shared conversation. Sign in to Orris to start your own chat.