Megaloblastic anemia
Reading File
Finding Sources
Searching PubMed
"megaloblastic anemia"[MeSH Terms] AND ("vitamin B12" OR "folate")
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, rich content from multiple authoritative textbooks. Let me compile the full response.
Megaloblastic Anemia
Megaloblastic anemia is a disorder of impaired DNA synthesis in hematopoietic (and other rapidly dividing) cells, resulting in abnormally large, nuclear-cytoplasmic asynchronous precursors and a characteristic peripheral blood picture. The two principal causes are vitamin B12 (cobalamin) deficiency and folate (folic acid) deficiency.
Pathogenesis
Both vitamin B12 and folate are required for synthesis of thymidine (dTMP), one of the four DNA bases. The key pathway:
- Folate (as FH4) acts as a one-carbon carrier. Its derivative N5,10-methylene-FH4 is needed to convert dUMP → dTMP for DNA synthesis.
- Vitamin B12 (as methylcobalamin) acts as cofactor for methionine synthase, converting homocysteine → methionine. In this reaction, N5-methyl-FH4 (the circulating form of folate) is converted back to FH4. Without B12, folate is "trapped" as N5-methyl-FH4 and unavailable for DNA synthesis - the "methyl-folate trap."
- A second B12-dependent reaction: adenosylcobalamin is required by methylmalonyl-CoA mutase to convert methylmalonyl-CoA → succinyl-CoA. Deficiency raises methylmalonic acid (MMA) levels, which is diagnostically useful.
The net result in either deficiency: deranged DNA synthesis → delayed nuclear maturation while cytoplasmic maturation proceeds normally → nuclear-cytoplasmic asynchrony → most precursors undergo apoptosis in the marrow (ineffective hematopoiesis) → pancytopenia.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 608-609
Causes
Vitamin B12 Deficiency
| Category | Examples |
|---|---|
| Decreased intake | Strict vegetarianism/veganism |
| Impaired absorption - Intrinsic factor (IF) deficiency | Pernicious anemia, total/partial gastrectomy |
| Impaired absorption - Ileal disease | Ileal resection, Crohn's ileitis |
| Diffuse intestinal disease | Lymphoma, systemic sclerosis |
| Competitive parasitic uptake | Fish tapeworm (Diphyllobothrium latum), bacterial overgrowth (blind loops) |
| Medications | Metformin, proton pump inhibitors, nitrous oxide |
| Pancreatic insufficiency | Reduced proteases → B12 not released from haptocorrin |
B12 stores (hepatic) last 3-5 years, so deficiency develops insidiously.
Folate Deficiency
| Category | Examples |
|---|---|
| Decreased intake | Alcoholism, poverty, elderly, psychiatric patients |
| Impaired absorption | Celiac disease, bariatric surgery |
| Drug-induced | Methotrexate, trimethoprim, pyrimethamine, phenytoin, sulfasalazine, ethanol, OCP |
| Increased requirement | Pregnancy (3-4x increase), hemolytic anemias (e.g., sickle cell), disseminated cancer |
| Increased loss | Hemodialysis |
Folate stores are limited - deficiency can develop within weeks to months.
- Washington Manual of Medical Therapeutics, p. 803; Robbins p. 608
Normal Vitamin B12 Absorption (Key for Pernicious Anemia)
- Stomach: Pepsin releases B12 from food proteins; B12 binds salivary haptocorrin
- Duodenum: Pancreatic proteases cleave B12 from haptocorrin; B12 binds intrinsic factor (IF) secreted by gastric parietal cells
- Terminal ileum: B12-IF complex binds cubilin receptor on ileal enterocytes → endocytosed
- Bloodstream: B12 bound to transcobalamin II → delivered to liver and bone marrow
Daily requirement: 2-3 µg. Animal products (meat, fish, eggs, dairy) are the only dietary sources; plants contain negligible amounts.
- Robbins p. 609
Pernicious Anemia (Major Cause of B12 Deficiency)
Pernicious anemia (PA) is an autoimmune gastritis destroying parietal cells, impairing IF production.
Key features:
-
Mean age of onset: 60 years; typically >40 years
-
Up to 30% have positive family history
-
Associated autoimmune conditions: Graves disease (~30%), Hashimoto thyroiditis (~11%), Addison disease (5-10%)
-
Antibodies: Anti-parietal cell antibodies (90% of PA patients); anti-IF antibodies (60%, highly specific)
-
Pathology: Chronic atrophic gastritis with loss of parietal and chief cells, lymphocytic/plasma cell infiltrate; intestinal metaplasia
-
Increased risk of gastric carcinoma (mucosa atrophy/metaplasia is irreversible with B12 therapy)
-
Washington Manual p. 803; Robbins p. 609-610
Morphology
Peripheral Blood Smear
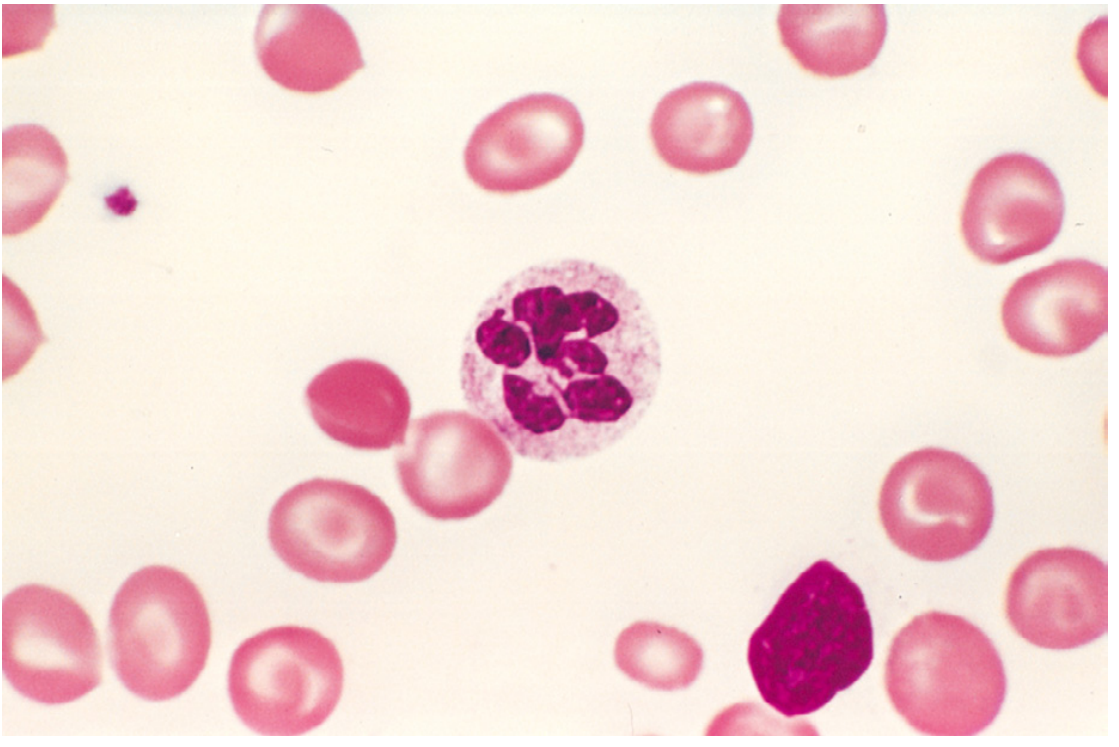
Fig. 14.15: Peripheral blood smear showing a hypersegmented neutrophil (6 lobes) and macro-ovalocytes. (Robbins)
- Macro-ovalocytes: Large, oval RBCs without central pallor - pathognomonic
- Anisocytosis and poikilocytosis
- Hypersegmented neutrophils: ≥5 nuclear lobes (normal: 3-4); even a single neutrophil with 6+ lobes is highly significant
- Low reticulocyte count (ineffective erythropoiesis)
- Pancytopenia in severe cases
Bone Marrow
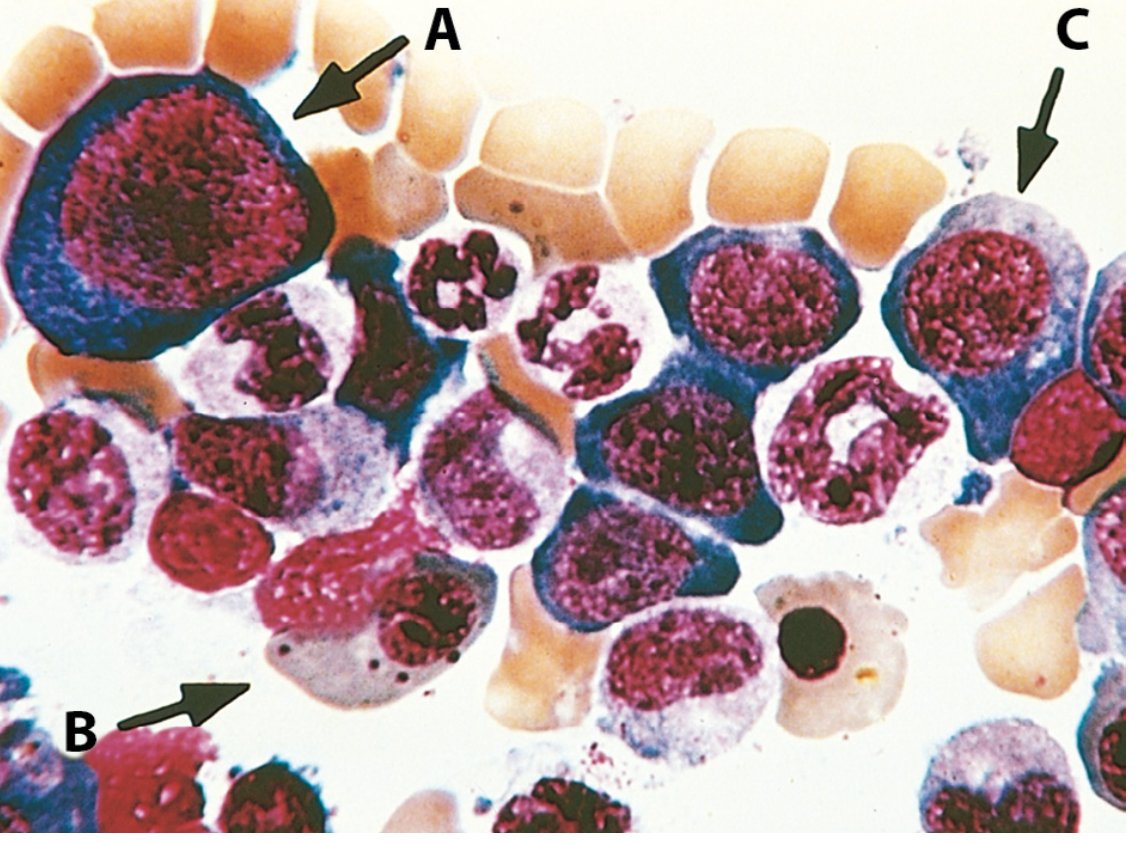
Fig. 14.16: Bone marrow aspirate showing megaloblasts (A-C) with nuclear-cytoplasmic asynchrony. (Robbins)
-
Hypercellular marrow (erythroid hyperplasia in response to elevated EPO)
-
Megaloblasts: Large erythroid precursors with finely distributed ("open") chromatin despite cytoplasmic hemoglobinization (nuclear-cytoplasmic asynchrony)
-
Giant metamyelocytes and band forms (granulocyte precursors also affected)
-
Bizarre, multilobate megakaryocytes
-
Robbins p. 608-609
Clinical Features
Hematologic
- Symptoms of anemia: fatigue, pallor, dyspnea, palpitations
- Jaundice (mild, from intramedullary hemolysis - elevated indirect bilirubin + LDH)
- Splenomegaly (extramedullary hematopoiesis in severe cases)
- Glossitis (beefy red, smooth tongue) - due to mucosal cell damage
- Skin/nail pigmentation
Neurologic (B12 deficiency only - NOT folate deficiency)
-
Subacute combined degeneration (SCD) of the spinal cord: demyelination of dorsal and lateral columns
-
Peripheral neuropathy, paresthesias, loss of vibratory and positional sense
-
Ataxia, positive Romberg sign
-
Confusion, dementia, behavioral changes
-
Neurologic symptoms can occur without anemia and may not fully reverse with treatment
-
Duration/severity before treatment inversely correlates with reversibility
-
Washington Manual p. 803-804; Goldman-Cecil p. 1734-1735
Diagnosis
Laboratory Tests
| Test | Findings |
|---|---|
| CBC | Macrocytic anemia (↑MCV), leukopenia, thrombocytopenia |
| Peripheral smear | Macro-ovalocytes, hypersegmented neutrophils |
| Serum B12 | Low (<200 pg/mL; borderline 100-400) |
| Serum/RBC folate | Low in folate deficiency |
| Methylmalonic acid (MMA) | Elevated in B12 deficiency; normal in folate deficiency |
| Homocysteine | Elevated in both B12 and folate deficiency |
| LDH | Markedly elevated (ineffective erythropoiesis) |
| Indirect bilirubin | Elevated |
| Anti-IF antibodies | Highly specific for pernicious anemia (60% sensitivity) |
| Anti-parietal cell antibodies | Sensitive (90%) but less specific for PA |
Key differentiator: MMA elevated = B12 deficiency; MMA normal + homocysteine elevated = folate deficiency.
Bone Marrow Biopsy
-
May be needed to exclude MDS or AML, which can mimic megaloblastic anemia with hypercellular marrow and immature cells
-
Washington Manual p. 803-804; Robbins p. 1276
Treatment
Vitamin B12 Deficiency
- Cyanocobalamin IM: 1 mg/day IM for 7 days, then 1 mg/week for 4 weeks, then 1 mg/month for life (for pernicious anemia or chronic malabsorption)
- High-dose oral B12 (1000-2000 µg/day): Effective even in PA because ~1% absorbed by passive diffusion (bypasses IF). An option for compliant patients without severe neurologic disease.
- Monitor: Reticulocytosis begins within 5-7 days; Hgb normalizes by 1-2 months
Folate Deficiency
- Folic acid 1 mg PO daily until corrected
- High-dose folic acid (5 mg/day) for malabsorption syndromes
- 5 mg/day periconceptionally for women at high risk of neural tube defects
Important Treatment Considerations
- Potassium monitoring: Transient hypokalemia at initiation due to rapid hematopoiesis - potentially life-threatening arrhythmias; supplement as needed
- Coexisting iron deficiency: Present in ~1/3 of patients - blunts response (MCV may fall into microcytic range with treatment)
- Do NOT give folate alone in B12 deficiency: Corrects anemia but does NOT halt neurologic deterioration - and may even worsen it
- Neurologic recovery: Paresthesias and behavioral changes respond best; established spinal cord lesions often do not fully reverse
- Pernicious anemia: B12 therapy is lifelong; gastric mucosal changes and carcinoma risk are unaffected by treatment
- Washington Manual p. 803-804; Goldman-Cecil p. 1734-1735
B12 vs. Folate Deficiency: Key Differences
| Feature | Vitamin B12 Deficiency | Folate Deficiency |
|---|---|---|
| Time to deficiency | Years (large hepatic stores) | Weeks-months (limited stores) |
| Common causes | PA, gastrectomy, ileal disease, veganism | Alcoholism, malnutrition, pregnancy, drugs |
| Neurologic disease | Yes (SCD, peripheral neuropathy) | No |
| Methylmalonic acid | Elevated | Normal |
| Homocysteine | Elevated | Elevated |
| Treatment | Cyanocobalamin IM or high-dose oral | Folic acid 1 mg PO daily |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 608-610; Washington Manual of Medical Therapeutics, pp. 803-804; Goldman-Cecil Medicine, pp. 1734-1735
This is a shared conversation. Sign in to Orris to start your own chat.