Myocardial infarction treatment
"myocardial infarction"[MeSH Terms] AND "treatment"[MeSH Terms]
myocardial infarction treatment guidelines 2025 STEMI NSTEMI
"acute coronary syndrome"[MeSH Terms] AND "percutaneous coronary intervention"[MeSH Terms]
Myocardial Infarction Treatment
The Core Principle
"The majority of patients who suffer an acute STEMI have thrombotic occlusion of a coronary artery. Early restoration of coronary perfusion limits infarct size, preserves LV function, and reduces mortality. All other therapies are secondary and should not delay the timely goal of achieving coronary reperfusion."
- Washington Manual of Medical Therapeutics
1. Immediate / Upstream Therapy (All MI Types)
| Agent | Dose | Purpose |
|---|---|---|
| Aspirin (ASA) | 162-325 mg chewed | Antiplatelet - 27% relative mortality reduction |
| P2Y12 inhibitor | Ticagrelor 180 mg, Prasugrel 60 mg, or Clopidogrel 300-600 mg | Added antiplatelet effect |
| Anticoagulation | UFH bolus 60 U/kg IV (max 4000 U) + infusion | Prevent thrombus extension |
| Nitroglycerin | SL or IV | Ischemic pain relief |
| Beta-blocker | Oral (if no contraindication) | Reduce O2 demand |
| Supplemental O2 | If SpO2 <90% | Reduce ischemic burden |
2. STEMI Reperfusion Strategy
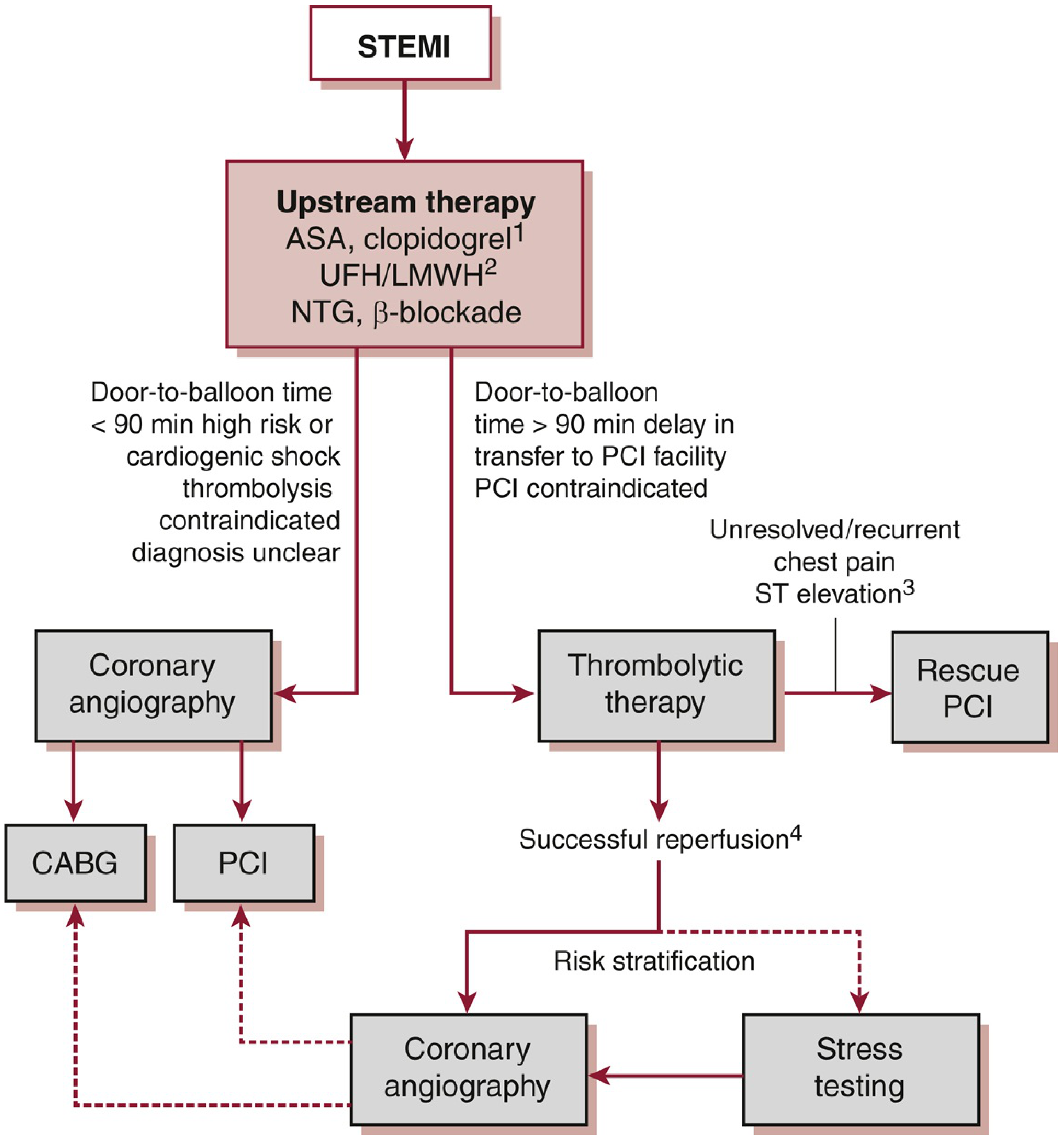
Primary PCI (Preferred)
- Target: Door-to-balloon time ≤90 minutes from first medical contact
- Superior to fibrinolysis for: vessel patency (TIMI 3 flow), less reinfarction, lower intracranial hemorrhage risk, improved survival
- Preferred when diagnosis is uncertain, cardiogenic shock is present, bleeding risk is high, or symptoms >2-3 hours (clot less lysable)
- PCI is preferred over fibrinolysis unless time to first coronary device delivery exceeds 120 minutes
- Complete revascularization: In STEMI patients without shock, PCI of non-culprit vessels (either at index procedure or within 45 days) reduces cardiovascular events. Exception: In cardiogenic shock, routine PCI of non-culprit arteries during initial primary PCI is contraindicated.
- P2Y12 choice for PCI: Ticagrelor, prasugrel, or clopidogrel
Fibrinolytic Therapy (when PCI not timely)
- Target: Door-to-needle time ≤30 minutes
- Agents: tPA, Tenecteplase (TNK - 0.5 mg/kg IV bolus, max 50 mg), Reteplase (rPA), Streptokinase
- TNK: slower clearance, improved fibrin specificity, equivalent mortality to tPA with less bleeding
- Always combine with ASA, clopidogrel (not prasugrel/ticagrelor - not studied with fibrinolytics), and anticoagulation (LMWH preferred over UFH when fibrinolysis used)
- Do NOT use GPIIb/IIIa inhibitors with fibrinolytics
- Prior intracranial hemorrhage / hemorrhagic stroke
- Ischemic stroke within 3 months
- Known intracranial structural lesion (AVM, aneurysm, tumor)
- Closed head injury within 3 months
- Aortic dissection
- Severe uncontrolled hypertension (SBP >180, DBP >110)
- Active bleeding or bleeding diathesis
- Acute pericarditis
Rescue PCI
- For failed fibrinolysis (persistent chest pain, <50% ST resolution at 90 min, hemodynamic instability)
- Class IIa recommendation - reduces HF and recurrent infarction even if no clear mortality benefit
- Repeat fibrinolysis is not recommended
Emergency CABG
- Reserved for: left main disease, failed PCI, coronary anatomy not amenable to PCI, mechanical complications (papillary muscle rupture, VSD, free wall rupture, ventricular aneurysm with refractory arrhythmia)
3. Anticoagulation in Detail
| Agent | Use Case |
|---|---|
| UFH | Standard with primary PCI; add to aspirin + fibrinolytic for patency |
| LMWH (Enoxaparin) | Preferred with fibrinolytics; reduces death/reinfarction vs UFH, but more bleeding |
| Bivalirudin | Direct thrombin inhibitor; studied with PCI only |
| Fondaparinux | Superior to placebo in STEMI without reperfusion; risky with PCI alone (catheter thrombosis risk) |
4. NSTEMI / UA Management
- All patients: ASA + P2Y12 inhibitor (DAPT) + anticoagulation + beta-blocker + statin
- High-risk features (elevated troponin, dynamic ST changes, refractory ischemia, hemodynamic instability, Killip class >1): Early invasive strategy - coronary angiography within 24-48 hours
- Lower-risk: Conservative (medical) strategy with stress testing for risk stratification
Recent meta-analysis (PMID: 40549394, JAMA Internal Medicine 2025) found early invasive strategy benefits older patients with ACS as well - this challenges older conservative approaches in the elderly.
5. Peri-Infarct Care (CCU)
- All STEMI patients: monitored CCU/ICU for ≥24 hours
- Continuous telemetry for ischemia and arrhythmias
- Daily ECGs, exam for new murmurs (VSD, MR) or HF signs
- Baseline echocardiogram: assess EF, wall motion, valvular lesions, ventricular thrombus
- Cardiac pacing: AV block in anterior MI is often unstable with wide QRS escape - usually requires temporary then permanent pacemaker. AV block in inferior MI tends to be transient.
| Class | Signs | Historical Mortality |
|---|---|---|
| I | No congestion | 0-5% |
| II | Basal rales, S3, mild HF | 10-20% |
| III | Pulmonary edema | 35-45% |
| IV | Cardiogenic shock (SBP <90, peripheral shutdown) | 85-95% |
6. Post-MI Long-Term / Secondary Prevention
| Drug Class | Specifics | Benefit |
|---|---|---|
| ASA | 81 mg/day indefinitely | Antiplatelet |
| P2Y12 inhibitor | Clopidogrel 75 mg/d, Prasugrel 10 mg/d, or Ticagrelor 90 mg BID for minimum 12 months (BMS or DES) | Reduced stent thrombosis, recurrent MI |
| Beta-blocker | Start within 24h, continue indefinitely | Mortality benefit post-MI |
| ACE inhibitor | Within 24h; most benefit in EF <40%, large anterior MI, prior MI | Reduces short-term mortality, HF incidence, recurrent MI |
| ARB | If ACE inhibitor intolerant | Equivalent benefit |
| Statin (high-intensity) | Goal: LDL <70 mg/dL or ≥50% LDL reduction | Multiple trials show benefit; start early |
| Ezetimibe / PCSK9 inhibitor | If LDL target not met on maximal statin | Additional LDL lowering |
7. Mechanical Complications (Post-MI)
| Complication | Onset | Key Feature |
|---|---|---|
| Ventricular septal rupture | 1-14 days (peak 24h + 3-5 days) | Harsh holosystolic murmur + thrill, biventricular failure |
| Free wall rupture | 1-14 days | Electromechanical dissociation, tamponade |
| Papillary muscle rupture | 1-14 days | Abrupt pulmonary edema, soft murmur, severe MR |
2025 Guideline Update (ACC/AHA)
- Intracoronary imaging during PCI upgraded from Class IIa to Class I recommendation for complex lesions
- Ticagrelor monotherapy (after ≥1 month of DAPT post-PCI) now a recommended de-escalation strategy to reduce bleeding
- For patients needing long-term anticoagulation post-PCI: discontinue aspirin 1-4 weeks after PCI, continue P2Y12 (preferably clopidogrel) with anticoagulant
- Dissolving the artificial STEMI/NSTEMI divide in initial evaluation and medical management
Search PubMed for latest primary PCI vs fibrinolysis outcomes
"percutaneous coronary intervention"[MeSH Terms] AND "fibrinolytic agents"[MeSH Terms] AND "myocardial infarction"[MeSH Terms]
"primary PCI" AND "thrombolysis" AND "STEMI" AND outcomes
primary PCI vs fibrinolysis STEMI outcomes 2024 2025 clinical trial meta-analysis
PMID: 37439219
PMID: 38925881
PMID: 35166796
https://pmc.ncbi.nlm.nih.gov/articles/PMC11607716
PMID: 41364063
PMID: 33838227
"pharmaco-invasive" AND STEMI AND outcomes
PMID: 39952376
PMID: 40035501
PMID: 41329963
PubMed Literature Review: Primary PCI vs. Fibrinolysis in STEMI
Evidence Summary
Tier 1 Evidence - Systematic Reviews & Meta-Analyses
Intracoronary Thrombolysis Adjunct to Primary PCI
- IC thrombolysis significantly reduced MACE: RR 0.65 (95% CI 0.51-0.82, p<0.0004)
- Improved LVEF: +1.87% (WMD, 95% CI 1.07-2.67, p<0.0001)
- No significant reduction in mortality alone (RR 0.91, p=0.77)
- No increase in major or minor bleeding
- Subgroup findings: benefit was significant with non-fibrin-specific (RR 0.39) and moderately fibrin-specific agents (RR 0.62), but not with highly fibrin-specific agents (RR 1.10, p=0.75)
Intracoronary Adjunctive Therapies - Network Meta-Analysis
- No IC adjunctive therapy significantly reduced all-cause mortality, non-fatal MI, or HF hospitalization vs. conventional primary PCI
- However, several strategies significantly reduced post-PCI TIMI 0-2 flow (a surrogate for microvascular obstruction):
- Fibrinolytic + manual thrombus aspiration: OR 0.24 (0.12-0.48) - strongest effect
- Verapamil: OR 0.22; Tirofiban: OR 0.43; Adenosine: OR 0.40; Manual aspiration alone: OR 0.61
- Safety signals: IC tirofiban increased any bleeding (IRR 1.65); IC adenosine increased peri-procedural AV blocks (OR 2.80)
Tier 3 Evidence - Randomized Controlled Trials
STREAM-2 Trial (Landmark RCT)
| Outcome | Pharmaco-Invasive (half TNK) | Primary PCI |
|---|---|---|
| ST resolution ≥50% (last angiography) | 85.2% | 78.4% |
| 30-day composite (death/shock/HF/reinfarction) | 12.8% | 13.3% (RR 0.96, CI 0.62-1.48) |
| Intracranial hemorrhage | 1.5% | 0% |
| Major non-ICH bleeding | <1.5% | <1.5% |
STREAM-1 vs. STREAM-2 Inter-Trial Comparison
- Half-dose vs. full-dose TNK: similar ST resolution ≥50% (71.2% vs. 68.7%, p=0.519) and similar ICH risk (2.1% vs. 1.5%, p=0.605) in ages 60-74
- Major non-ICH bleeding was dramatically lower in STREAM-2: 0.3% vs. 7.1% in the PI arm - attributed to refined anticoagulation protocols
Pharmaco-Invasive Strategy with Half-Dose Prourokinase vs. Primary PCI
Rescue PCI in the Pharmaco-Invasive Era (STREAM-2 Sub-Analysis)
- Rescue PCI patients had significantly worse outcomes vs. those with successful fibrinolysis + scheduled PCI: 30-day composite 16.7% vs. 6.0% (p<0.001); higher ICH risk 2.4% vs. 0.5%
- Primary PCI patients had intermediate outcomes (30-day composite 12.2%)
- Delays in deploying rescue PCI were shortened in hub-and-spoke systems, resulting in comparable outcomes regardless of initial setting (ambulance vs. community hospital)
Review-Level Evidence
Comprehensive ACS Diagnosis & Treatment Review (JAMA)
- Primary PCI within 120 min reduces STEMI mortality from 9% → 7%
- For NSTE-ACS: early invasive strategy (angiography + revascularization within 24-48h) reduces mortality from 6.5% → 4.9%
- Fibrinolytic dosing protocol: full-dose for patients <75 years; half-dose for patients ≥75 years (or full-dose streptokinase if cost is a concern)
- ACS affects >7 million people/year globally, >1 million hospitalizations/year in the US
Rural STEMI: Fibrinolysis vs. Primary PCI
Synthesis: What the Current Evidence Says
| Dimension | Primary PCI | Pharmaco-Invasive / Fibrinolysis |
|---|---|---|
| Gold standard | Yes - when achievable within 90-120 min | Second-line when PCI delayed |
| Mortality reduction (STEMI) | 9% → 7% (Bhatt, JAMA 2022) | Comparable if PI strategy used correctly |
| ICH risk | ~0% | ~1.5% (half-dose TNK, STREAM-2) |
| Procedure-related complications (no-reflow, arrhythmia) | Higher in some RCTs | Lower with pharmaco-invasive (Jiang 2025) |
| Elderly patients (≥60 yrs) | Preferred when available | Half-dose TNK PI strategy = reasonable alternative (STREAM-2, 2023) |
| Rescue PCI (failed fibrinolysis) | Required in ~43% of PI cases | Worst outcomes if delayed; hub-and-spoke systems critical |
| IC adjunctive thrombolysis | Reduces MACE (RR 0.65) and improves LVEF | No hard outcome benefit from IC vasoactive agents (network MA, 2026) |
| Rural/resource-limited settings | Preferred if achievable | Fibrinolysis not inferior for in-hospital mortality (rural cohort 2024) |