Emergency drugs duty doctor should know
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
emergency drugs duty doctor must know doses indications 2024
Reading File
Reading File
Reading Web Page
https://steinem.org/aaem-50-drugs-to-know
I now have rich data from Tintinalli's, Rosen's, the AAEM 50 drugs list, and Barash anesthesia. Let me compile a comprehensive, well-organized reference.
Emergency Drugs Every Duty Doctor Must Know
A practical, high-yield reference organized by clinical scenario. Doses are for adults unless noted.
1. CARDIAC ARREST (ACLS)
Epinephrine (Adrenaline)
- MOA: Alpha + beta adrenergic agonist; increases coronary/cerebral perfusion pressure
- Dose: 1 mg IV (1:10,000) every 3-5 min during CPR
- Pediatric: 0.01 mg/kg IV (1:10,000); max 1 mg
- Indications: VF/pulseless VT (after 2 shocks), PEA, asystole
- Pitfall: Tissue necrosis if extravasates - needs central line for infusion; dysrhythmias
Amiodarone
- MOA: Class III antiarrhythmic - blocks Na/K/Ca channels + beta blockade
- Dose: 300 mg IV bolus for shock-refractory VF/pulseless VT; second dose 150 mg
- Infusion: 1 mg/min x 6 h, then 0.5 mg/min x 18 h
- Indications: Shock-refractory VF/VT, stable VT, AF rate control
- Pitfall: Hypotension, bradycardia, pulmonary toxicity (chronic), thyroid disease
Lidocaine (alternative to amiodarone)
- Dose: 1-1.5 mg/kg IV bolus for VF/pulseless VT
- Maintenance: 1-4 mg/min infusion
- Pitfall: CNS toxicity (seizures, confusion) at toxic levels
Magnesium Sulfate
- Dose: 2 g IV push (pulseless Torsades); 2 g IV over 15 min (Torsades with pulse, status asthmaticus, eclampsia)
- Indications: Torsades de Pointes, eclampsia/pre-eclampsia, status asthmaticus, hypomagnesemia
- Pitfall: Hypotension, respiratory depression, loss of patellar reflex (monitor Mg levels)
2. BRADYCARDIA / HEART BLOCK
Atropine
- MOA: Muscarinic antagonist - increases SA node rate, AV conduction
- Dose: 0.5 mg IV; repeat every 3-5 min; max 3 mg
- Pediatric: 0.02 mg/kg IV; min dose 0.1 mg; max 0.5 mg (child), 1 mg (adolescent)
- Indications: Symptomatic bradycardia, vagal syncope, organophosphate poisoning
- Pitfall: Paradoxical bradycardia at doses < 0.1 mg (pediatrics); ineffective in heart transplant patients
Dopamine
- Dose: 2-20 mcg/kg/min IV infusion
- Low (2-5 mcg/kg/min): renal/mesenteric vasodilation
- Mid (5-10 mcg/kg/min): beta-1 = inotrope/chronotrope
- High (>10 mcg/kg/min): alpha = vasoconstrictor
- Indications: Symptomatic bradycardia unresponsive to atropine, cardiogenic/distributive shock
3. TACHYARRHYTHMIAS
Adenosine
- MOA: Blocks AV node conduction transiently (endogenous purinergic agonist)
- Dose: 6 mg rapid IV push + flush; if no response in 1-2 min, 12 mg; may repeat 12 mg once
- Indications: SVT (AVNRT, AVRT) - diagnostic and therapeutic
- Pitfall: Very short half-life (10 s) - must push fast and flush; transient complete heart block; bronchospasm in asthma; do not use in pre-excited AF (WPW) - may precipitate VF
Metoprolol / Esmolol (beta-blockers)
- Esmolol: 500 mcg/kg loading dose, then 50-300 mcg/kg/min infusion
- Indications: AF/flutter rate control, aortic dissection, SVT
- Pitfall: Decompensated CHF, bronchospasm, hypotension
Diltiazem (CCB)
- Dose: 0.25 mg/kg IV over 2 min; repeat 0.35 mg/kg in 15 min if needed
- Indications: AF/flutter rate control, SVT (if beta-blockers contraindicated)
- Pitfall: Hypotension, heart block; contraindicated in WPW with AF
4. ANAPHYLAXIS
(Source: Tintinalli's Emergency Medicine; Rosen's Emergency Medicine)
Epinephrine - FIRST LINE, give immediately
- Adult: 0.3-0.5 mg IM (1:1,000 = 1 mg/mL) in anterolateral thigh; repeat every 5-10 min
- Pediatric: 0.01 mg/kg IM (1:1,000); max 0.5 mg; repeat every 5-10 min
- IV infusion (severe/refractory): Start 1 mcg/min, titrate up
- Simultaneously: oxygen, supine position, large-bore IV, 1-2 L NS bolus
Second-Line (do NOT delay epinephrine for these)
| Drug | Adult Dose | Role |
|---|---|---|
| Diphenhydramine | 25-50 mg IV/IM/PO q6h | H1 blocker |
| Ranitidine/Famotidine | 50 mg IV (ranitidine) or 40 mg IV (famotidine) | H2 blocker |
| Hydrocortisone | 250-500 mg IV | Prevent biphasic reaction |
| Methylprednisolone | 80-125 mg IV | Prevent biphasic reaction |
| Albuterol | 2.5-5 mg nebulized q20 min | Bronchospasm |
| Glucagon | 1-5 mg IV bolus | Anaphylaxis refractory to epi (beta-blocker patients) |
5. RESPIRATORY EMERGENCIES
Salbutamol (Albuterol)
- MOA: Selective beta-2 agonist - bronchodilation
- Nebulized: 2.5-5 mg q20 min x 3, then q1-4h prn; or 10-15 mg continuous
- IV (severe): 5 mcg/min, titrate to 20 mcg/min
- Indications: Acute asthma, COPD exacerbation, anaphylaxis bronchospasm, hyperkalemia
- Pitfall: Hypokalemia, tachycardia, hyperglycemia
Ipratropium Bromide
- Dose: 0.5 mg nebulized q20 min x 3 (combined with albuterol in first hour)
- Indications: Acute asthma, COPD exacerbation (add to beta-agonist)
Hydrocortisone / Methylprednisolone
- Status asthmaticus: Hydrocortisone 1-2 mg/kg IV q6h; or methylprednisolone 1-2 mg/kg IV
- Reduces airway inflammation, decreases relapse rate
6. HYPERTENSIVE EMERGENCIES
Labetalol
- Dose: 20 mg IV slowly over 2 min; may repeat 40-80 mg q10 min; max 300 mg total. Infusion: 0.5-2 mg/min
- Indications: Hypertensive emergency, aortic dissection, hypertension in pregnancy (safe in pregnancy)
- Pitfall: Bronchospasm, heart block
Nitroglycerin (GTN)
- Dose: 5-200 mcg/min IV; start low and titrate q3-5 min
- Indications: Acute LVF/pulmonary edema, unstable angina/NSTEMI, hypertensive emergency
- Pitfall: Hypotension (especially with sildenafil/PDE5 inhibitors - absolute contraindication), methemoglobinemia
Sodium Nitroprusside
- Dose: Start 0.3 mcg/kg/min; titrate to effect; max 10 mcg/kg/min
- Indications: Hypertensive emergency with end-organ damage, acute LVF
- Pitfall: Cyanide toxicity (prolonged use or high doses), methemoglobinemia, photosensitive - cover infusion bag
Hydralazine
- Dose: 10-20 mg IV/IM; repeat q4-6h
- Indications: Hypertension in pregnancy/eclampsia (widely used)
- Pitfall: Reflex tachycardia, lupus-like syndrome (chronic)
7. CHEST PAIN / ACS
Aspirin
- Dose: 300-325 mg PO (chewed) immediately
- Indications: Suspected ACS (STEMI/NSTEMI), stroke prevention
- Pitfall: Active GI bleed, true aspirin allergy
Morphine
- Dose: 1-5 mg IV slow push; titrate q5-15 min
- Indications: Severe pain in ACS, acute pulmonary edema (use cautiously - some evidence of harm in NSTEMI)
- Pitfall: Respiratory depression, hypotension, nausea; may delay absorption of P2Y12 inhibitors
Heparin (Unfractionated)
- STEMI/NSTEMI: 60-70 units/kg IV bolus (max 5000 units), then 12-15 units/kg/h
- Indications: ACS, PE, DVT, AF
- Pitfall: HIT (heparin-induced thrombocytopenia), bleeding
Enoxaparin (LMWH)
- Dose: 1 mg/kg SC q12h; or 1.5 mg/kg SC q24h (PE/DVT)
- Indications: NSTEMI, PE, DVT
- Pitfall: Renally excreted - reduce dose in CKD; avoid with spinal anesthesia; monitor anti-Xa in obesity/renal impairment
8. SEIZURES / STATUS EPILEPTICUS
Diazepam
- Dose: 5-10 mg IV/IM/PR; repeat q5 min; max 30 mg
- Pediatric: 0.1-0.3 mg/kg IV/PR
- Indications: First-line status epilepticus, alcohol withdrawal seizures, eclamptic seizures
- Pitfall: Respiratory depression, hypotension; has propylen glycol vehicle (irritant IV)
Lorazepam
- Dose: 4 mg IV over 2 min; repeat once after 5-10 min if needed
- Indications: Status epilepticus (preferred by many guidelines over diazepam IV)
- Pitfall: Respiratory depression; requires refrigeration
Midazolam (IM preferred if no IV access)
- Dose: 10 mg IM (>40 kg); 5 mg IM (13-40 kg); buccal/intranasal: 0.2 mg/kg
- Indications: Status epilepticus, procedural sedation, RSI (as induction adjunct)
Phenytoin / Fosphenytoin
- Load: Phenytoin 15-20 mg/kg IV at max 50 mg/min (fosphenytoin 150 mg PE/min, faster)
- Second-line after benzodiazepines fail
- Pitfall: Cardiac arrhythmias during IV load, hypotension, Purple Glove Syndrome (phenytoin extravasation), zero-order kinetics
9. HYPOGLYCEMIA
Dextrose (Glucose)
- D50%: 25-50 mL (12.5-25 g) IV bolus - adults
- D10%: Preferred in many settings to avoid hyperglycemia rebound
- Pediatric: D10% 2-5 mL/kg IV, or D25% 1-2 mL/kg
- Pitfall: Do not give dextrose to Wernicke's-risk patients without thiamine first
Glucagon
- Dose: 1 mg IV/IM/SC (adult); 0.5 mg (child <25 kg)
- Indications: Hypoglycemia (no IV access), beta-blocker/CCB overdose (3-10 mg IV load)
- Pitfall: Vomiting (aspiration risk), ineffective in starvation/liver disease (depleted glycogen)
Thiamine (Vitamin B1) - give BEFORE dextrose in at-risk patients
- Dose: 100 mg IV/IM
- Indications: Wernicke's encephalopathy risk (alcohol use disorder, malnutrition, prolonged vomiting)
10. OVERDOSE / POISONING
Naloxone (Narcan)
- Dose: 0.4-2 mg IV/IM/IN; repeat q2-3 min; titrate to respiratory rate
- Indications: Opioid overdose (respiratory depression, coma)
- Pitfall: Short half-life (30-90 min) - opioid may outlast it; may precipitate acute withdrawal; may require infusion for long-acting opioids
Flumazenil
- Dose: 0.2 mg IV over 30 s; repeat 0.1 mg q1 min; max 1 mg
- Indications: Benzodiazepine reversal (diagnostic/therapeutic)
- Pitfall: Precipitates seizures in benzo-dependent patients or those with mixed TCA overdose; do not use routinely in undifferentiated coma
Activated Charcoal
- Dose: 1 g/kg PO (max 50 g); ideally within 1 hour of ingestion
- Indications: Most oral overdoses (effective for salicylates, TCAs, anticonvulsants)
- Pitfall: Contraindicated if airway not protected, caustic ingestion, hydrocarbons, or absent bowel sounds
Atropine (Organophosphate poisoning)
- Dose: 2-4 mg IV every 5-15 min until secretions dry; no ceiling dose
- Indications: Organophosphate/carbamate poisoning, nerve agent exposure
- Mnemonic for OP toxidrome: SLUDGE (Salivation, Lacrimation, Urination, Defecation, GI cramps, Emesis) + DUMBELS
11. SHOCK / HEMODYNAMIC SUPPORT
Norepinephrine (Noradrenaline)
- Dose: 0.01-3 mcg/kg/min IV infusion; titrate to MAP >65
- Indications: First-choice vasopressor in septic shock, distributive shock
- Pitfall: Tissue necrosis with extravasation; needs central line
Adrenaline (Epinephrine) infusion
- Dose: 1-10 mcg/min (or 0.01-0.5 mcg/kg/min)
- Indications: Anaphylactic shock, cardiogenic shock (add-on), anesthesia-induced hypotension
Dobutamine
- Dose: 2-20 mcg/kg/min IV infusion
- Indications: Decompensated heart failure, cardiogenic shock with low CO
- Pitfall: Tachycardia, hypotension if not euvolemic, proarrhythmic; PVCs
Vasopressin
- Dose: 0.03-0.04 units/min IV (fixed dose in septic shock, added to norepinephrine)
- Indications: Adjunct in vasoplegic/septic shock refractory to norepinephrine
12. PAIN & PROCEDURAL SEDATION
Morphine
- Dose: 2-4 mg IV q4-6h; titrate
- Pediatric: 0.05-0.1 mg/kg IV q2-4h
Fentanyl
- Dose: 25-100 mcg IV q1-2h; recommended 1 mcg/kg
- Procedural sedation: 1-2 mcg/kg IV (fast onset, short duration)
- Pitfall: Respiratory depression, rigid chest syndrome with rapid high-dose infusion, laryngospasm
Ketamine
- Dose (procedural sedation): 1-2 mg/kg IV; or 4-5 mg/kg IM
- Dissociative anesthesia dose (RSI): 1.5-2 mg/kg IV
- Indications: Procedural sedation, RSI induction (bronchospasm, hypotension, trauma), analgesic sub-dissociative (0.1-0.5 mg/kg IV)
- Pitfall: Laryngospasm (rare), emergence reaction (give midazolam 0.05 mg/kg IV to prevent), increased secretions, hypertension/tachycardia
13. ECLAMPSIA / OBSTETRIC EMERGENCIES
Magnesium Sulfate
- Pre-eclampsia/eclampsia seizure prophylaxis: 4-6 g IV over 15-20 min, then 1-2 g/h infusion
- Monitor: Respiratory rate, patellar reflexes, urine output, Mg level
- Antidote for Mg toxicity: Calcium gluconate 1 g (10 mL of 10%) IV
Labetalol / Hydralazine - for hypertension in pregnancy (see above)
14. QUICK-REFERENCE DOSE CARD
| Drug | Emergency Dose (Adult IV) | Primary Indication |
|---|---|---|
| Epinephrine | 1 mg q3-5 min (arrest); 0.3-0.5 mg IM (anaphylaxis) | Cardiac arrest, anaphylaxis |
| Atropine | 0.5-1 mg q3-5 min (max 3 mg) | Bradycardia, OP poisoning |
| Amiodarone | 300 mg bolus | VF/VT refractory |
| Adenosine | 6 mg rapid push, then 12 mg | SVT |
| Magnesium | 2 g push (Torsades); 4-6 g over 20 min (eclampsia) | Torsades, eclampsia, asthma |
| Morphine | 2-4 mg titrate | Severe pain, APO |
| Fentanyl | 1-2 mcg/kg IV | Procedural pain/sedation |
| Naloxone | 0.4-2 mg q2-3 min | Opioid overdose |
| Diazepam | 5-10 mg q5 min (max 30 mg) | Status epilepticus |
| Lorazepam | 4 mg IV over 2 min | Status epilepticus |
| Midazolam | 10 mg IM | Seizure (no IV access) |
| Dextrose 50% | 25-50 mL IV push | Hypoglycemia |
| Glucagon | 1 mg IV/IM | Hypoglycemia, beta-blocker OD |
| Norepinephrine | 0.01-3 mcg/kg/min infusion | Septic shock |
| Dobutamine | 2-20 mcg/kg/min infusion | Cardiogenic shock |
| GTN | 5-200 mcg/min infusion | ACS, LVF, hypertensive emergency |
| Labetalol | 20 mg IV q10 min (max 300 mg) | Hypertensive emergency |
| Hydrocortisone | 100-250 mg IV | Adrenal crisis, asthma, anaphylaxis |
| Ketamine | 1.5-2 mg/kg IV | RSI, procedural sedation |
Key Principles to Remember
- Epinephrine is the universal emergency drug - cardiac arrest, anaphylaxis, severe bronchospasm, airway emergencies
- ABCDE first - drugs support, not replace, basic resuscitation (airway, breathing, circulation)
- Pre-calculate weight-based doses - especially for pediatric and critically ill patients
- Know your antidotes: Naloxone (opioids), flumazenil (benzos), atropine/pralidoxime (organophosphates), calcium gluconate (Mg toxicity, CCB OD), N-acetylcysteine (paracetamol), Vitamin K/FFP (warfarin)
- Dose errors kill - particularly with epinephrine (1:1,000 vs 1:10,000 concentration); always double-check
- Always have emergency drugs drawn up and labeled before procedures - prefilled syringes with doses written for that patient's weight
Sources: Tintinalli's Emergency Medicine (9e); Rosen's Emergency Medicine (9e); Barash Clinical Anesthesia (9e); AAEM 50 Drugs Every Emergency Physician Should Know
Can you tell me the place where pain occurs and how this pain will tell about diagnosis
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
pain location diagnosis body regions clinical signs referred pain anatomy
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive data from multiple authoritative sources. Let me compile a thorough, well-organized answer.
Pain Location as a Diagnostic Guide
Understanding where pain occurs - and how it behaves - is one of the most powerful diagnostic tools in clinical medicine. Here is a body-region-by-region breakdown.
Understanding Pain Types First
Before going region by region, three types of pain matter clinically:
| Type | Mechanism | Character | Location |
|---|---|---|---|
| Visceral pain | Stretching/distension of hollow organs | Dull, crampy, poorly localized | Midline (epigastric, periumbilical, hypogastric) |
| Somatic/Parietal pain | Inflammation of peritoneum/parietal surfaces | Sharp, well-localized | Directly over affected organ |
| Referred pain | Shared spinal cord segments (dermatomes) | Variable | Felt away from source |
HEAD AND NECK PAIN
Headache Location → Diagnosis
| Location | Likely Diagnosis | Key Features |
|---|---|---|
| Unilateral, frontotemporal | Migraine | Throbbing, nausea, photophobia, 4-72 hours, worsened by activity |
| Around/behind one eye | Cluster headache | Excruciating, unilateral, with lacrimation, nasal congestion, Horner's; 15-180 min, nocturnal, "alarm clock" headache |
| Band-like, bilateral | Tension headache | Pressure/squeezing, no nausea/vomiting, not worsened by activity |
| Sudden "thunderclap" (worst of life) | Subarachnoid hemorrhage | Peaks in seconds, meningism, "hit on the back of the head" - emergency |
| Temple, jaw claudication (elderly) | Temporal arteritis (GCA) | >50 yrs, tender scalp, raised ESR/CRP, vision loss risk |
| Occipital + neck stiffness + fever | Meningitis | Kernig's/Brudzinski's signs |
| Morning headache, worse lying flat | Raised ICP | Nausea, papilloedema, worsens with Valsalva |
| Facial pain + blocked nose | Sinusitis | Tenderness over sinuses, worsens with bending forward |
| Jaw/ear/temple pain on chewing | TMJ disorder / dental | Crepitus in joint, malocclusion |
CHEST PAIN
(Source: Goldman-Cecil Medicine, TABLE 39-2)
| Location & Quality | Likely Diagnosis | Aggravating/Relieving | Clues |
|---|---|---|---|
| Retrosternal, radiates to jaw/left arm/shoulder | Angina / ACS | Worse with exertion/cold/stress; relieved by GTN and rest | Pressure, squeezing, "heaviness", < 20 min (angina) / ≥ 30 min (MI) |
| Substernal, ≥ 30 min, not relieved | Myocardial infarction | Not relieved by GTN; rest or exertion | Burning/constricting; sweating, nausea, vomiting |
| Anterior chest, tearing/ripping, radiates to back | Aortic dissection | Sudden onset, maximal from start | Excruciating, knifelike; BP difference between arms; hypertension, Marfan's |
| Over sternum/cardiac apex, sharp, stabbing | Pericarditis | Worse with breathing, rotating; relieved by sitting forward | Sharp/knifelike; pericardial rub; worsens supine |
| Localized unilateral, sharp | Pleurisy / Pneumonia / PE | Worse with deep breathing and coughing | Pleuritic character; fever (pneumonia); sudden onset + dyspnea (PE) |
| Substernal, pressure | Pulmonary hypertension | Worse with effort | Dyspnea, tachycardia, signs of right heart failure |
| Epigastric or lower sternal, burning | GERD / Oesophageal | Worse after meals, lying flat; relieved by antacids | Acid taste, regurgitation; no radiation to arm |
| Localized, point tenderness on pressure | Costochondritis (Tietze) | Worsened by palpation | Reproducible tenderness at costochondral junctions |
| Left anterior chest, brief, sharp | Functional / Da Costa / Musculoskeletal | Not related to exertion | Seconds, anxiety, young patients |
Key Rule: Radiation Pattern in Cardiac Pain
- Radiates to left arm/shoulder → ischemic heart disease
- Radiates to jaw → MI (often missed, especially in women/diabetics)
- Radiates to back (tearing) → aortic dissection
- Radiates to jaw + back → dissection vs. severe MI
ABDOMINAL PAIN BY QUADRANT
(Source: Textbook of Family Medicine, Table 38-1; Tintinalli's; Rosen's)
The Four Quadrant Rule
RUQ | LUQ
------+------
RLQ | LLQ
Right Upper Quadrant (RUQ)
| Diagnosis | Character | Key Signs |
|---|---|---|
| Biliary colic / Cholecystitis | Colicky → constant, RUQ/epigastric | Murphy's sign, radiates to right shoulder/scapula, post-fatty meal |
| Hepatitis / Liver abscess | Dull aching, RUQ | Tender hepatomegaly, jaundice, fever |
| Amoebic hepatitis | RUQ pain referred to right shoulder | History of dysentery, fever |
| Peptic ulcer (duodenal) | Epigastric/RUQ, burning | Relieved by food (duodenal), worse with food (gastric) |
| Pneumonia / Pleurisy (right lower lobe) | RUQ pain, pleuritic | Fever, cough, referred from chest |
| Inferior MI | RUQ/epigastric pain | ECG changes, diaphoresis |
| Renal colic (right) | Severe, flank → loin → groin | Colicky, hematuria, can't stay still |
| Fitz-Hugh-Curtis | RUQ pain, young woman | STI history, perihepatitis from gonorrhea/chlamydia |
Left Upper Quadrant (LUQ)
| Diagnosis | Character | Key Signs |
|---|---|---|
| Gastritis / Peptic ulcer | Epigastric/LUQ, burning | H. pylori, NSAIDs, worse with food |
| Pancreatitis | LUQ/epigastric, radiates to back like a band | Severe, nausea, vomiting; alcohol/gallstones history |
| Splenic pathology | LUQ aching | Rupture: sudden severe (trauma, EBV); infarct: sharp |
| Cardiac (angina/MI) | LUQ/epigastric - can be confused | ECG required |
| Left lower lobe pneumonia | LUQ pain, pleuritic | Fever, respiratory signs |
| Renal/Ureteral calculi (left) | Flank → groin, colicky | Hematuria |
Right Lower Quadrant (RLQ)
| Diagnosis | Character | Key Signs |
|---|---|---|
| Appendicitis | Starts periumbilical → migrates to McBurney's point (RLQ) | Rebound tenderness, guarding; anorexia, fever; Rovsing's/psoas/obturator signs |
| Ovarian cyst / Torsion | Sudden severe RLQ | Young woman; nausea/vomiting; US confirms |
| Ectopic pregnancy | RLQ or LLQ | Missed period, +hCG; shoulder pain (haemoperitoneum) |
| Renal/Ureteral colic (right) | Flank → RLQ → groin | Hematuria, colicky |
| Meckel's diverticulum | RLQ, like appendicitis | Children, painless rectal bleeding |
| Crohn's disease | RLQ, chronic/recurrent | Diarrhoea, weight loss, mouth ulcers |
| Psoas abscess | RLQ/hip pain | Hip flexion contracture, fever |
| Inguinal hernia (incarcerated) | RLQ/groin | Irreducible groin lump |
Left Lower Quadrant (LLQ)
| Diagnosis | Character | Key Signs |
|---|---|---|
| Diverticulitis | LLQ (sigmoid), constant, aching | Elderly, fever, altered bowel habit; "left-sided appendicitis" |
| Ovarian pathology (left) | LLQ | Cyst/torsion/ectopic; same as RLQ but left side |
| Ureteral colic (left) | Flank → LLQ → groin | Hematuria, restless |
| Irritable bowel syndrome | LLQ or generalized | Relieved by defecation; altered stool form; no alarm features |
| Ulcerative colitis | LLQ + rectal | Bloody diarrhoea, urgency, tenesmus |
Central / Periumbilical Pain
| Diagnosis | Character | Key Signs |
|---|---|---|
| Early appendicitis | Periumbilical → RLQ | Classic migration |
| Small bowel obstruction | Central, colicky | Distension, vomiting, tinkling bowel sounds |
| Mesenteric ischemia | Severe central, "pain out of proportion to exam" | Atrial fibrillation, vascular disease, elderly |
| Aortic aneurysm (rupture) | Severe central/back | Pulsatile mass, hypotension, collapse |
| Pancreatitis | Epigastric → central → back | Amylase/lipase elevated |
| Gastroenteritis | Periumbilical, crampy | Diarrhoea, vomiting, fever |
Epigastric Pain
| Diagnosis | Character | Key Signs |
|---|---|---|
| Gastric ulcer | Epigastric burning, worse with food | H. pylori, NSAIDs |
| Duodenal ulcer | Epigastric, relieved by food, wakes patient at night | Hunger pain 2-3 hrs after meal |
| Pancreatitis | Severe epigastric, radiates to back, band-like | Worse supine, relieved by leaning forward |
| GERD | Burning epigastric + retrosternal | Worse postprandial, lying flat |
| MI (inferior) | Epigastric - mimics indigestion | ECG is mandatory; diaphoresis |
LOIN / FLANK / BACK PAIN
| Location | Diagnosis | Character |
|---|---|---|
| Loin → groin (colicky) | Ureteral colic (renal stone) | Excruciating colicky, hematuria, can't find comfortable position, nausea/vomiting |
| Loin pain + fever + dysuria | Pyelonephritis | Renal angle tenderness, systemic upset |
| Loin pain (dull, aching) | Renal cell carcinoma / hydronephrosis | Haematuria, weight loss, abdominal mass |
| Central back, tearing | Aortic dissection | Radiates from anterior chest to back |
| Low back + belt-like to left shoulder | Pancreatitis | Bandlike, radiates through to back |
| Low back pain + sciatica (L4-S1) | Disc prolapse / nerve root compression | Straight-leg raise test positive; dermatomal distribution |
| Low back + fever | Vertebral osteomyelitis / discitis | Night pain, point tenderness over spine |
| Low back + bilateral leg weakness/bladder | Cauda equina syndrome | Saddle anaesthesia, urinary retention - surgical emergency |
PELVIC PAIN
| Location | Diagnosis | Character |
|---|---|---|
| Suprapubic | UTI / Cystitis | Dysuria, frequency, urgency |
| Suprapubic + fever | PID | Cervical excitation, adnexal tenderness |
| Iliac fossa, sudden, severe | Ovarian torsion | Nausea/vomiting, US shows absent flow |
| Unilateral, + missed period | Ectopic pregnancy | hCG positive, US - no intrauterine pregnancy |
| Cyclical pelvic pain | Endometriosis / Dysmenorrhoea | Dyspareunia, infertility, worse at menstruation |
| Perineal/rectal | Prostatitis / Perianal abscess | Fever, perineal tenderness, PR examination |
REFERRED PAIN PATTERNS - IMPORTANT CHART
(Source: Harrison's Principles of Internal Medicine; Color Atlas of Human Anatomy)
| Organ | Where Pain Is Felt | Why |
|---|---|---|
| Heart (ischemia) | Left arm, jaw, neck, epigastrium | Shared T1-T4 dermatomes |
| Liver / Gallbladder | Right shoulder, right scapula | Phrenic nerve (C3-C5) via diaphragmatic irritation |
| Spleen | Left shoulder (Kehr's sign) | Same phrenic nerve pathway |
| Pancreas | Back (band-like), left shoulder | Retroperitoneal structure; coeliac plexus |
| Appendix (early) | Periumbilical (T10) | Visceral pain via T10 before somatic localization |
| Kidneys / Ureter | Loin → ipsilateral groin/testis/labia | T10-L1 dermatomal referral |
| Diaphragm irritation | Shoulder tip (ipsilateral) | Phrenic nerve C3-C5 |
| Aortic aneurysm | Back, loin, groin | Retroperitoneal pressure |
| Prostate/rectum | Perineum, thighs, low back | S2-S4 |
| Ectopic pregnancy | Shoulder tip (diaphragmatic blood) + ipsilateral LLQ/RLQ | Haemoperitoneum irritating diaphragm |
THE SOCRATES FRAMEWORK - How Pain Quality Narrows Diagnosis
Beyond location, these features are diagnostic gold:
| Feature | What to Ask | Diagnostic Implication |
|---|---|---|
| Site | Where exactly? Point with one finger | Localized = somatic; diffuse = visceral/peritonitis |
| Onset | Sudden vs. gradual? | Sudden = vascular (dissection, MI, rupture, torsion); gradual = inflammatory |
| Character | Burning, stabbing, cramping, tearing? | Burning = ulcer/GERD; tearing = dissection; cramping = colic/obstruction; stabbing = pleuritic/pericarditis |
| Radiation | Does it go anywhere? | Left arm = cardiac; back = dissection/pancreatitis; groin = renal colic; shoulder = diaphragm irritation |
| Associations | Vomiting, fever, sweating, jaundice? | Fever = infection/inflammation; jaundice = biliary; diaphoresis = cardiac/vascular |
| Time | Constant vs. colicky? Duration? | Colicky = hollow viscus (stone, bowel); constant = solid organ or peritonitis |
| Exacerbating/Relieving | Food, position, breathing, movement? | Worse with breathing = pleuritic/pericarditis; food relieves = duodenal ulcer; leaning forward relieves = pericarditis/pancreatitis |
| Severity | Score /10; "worst ever"? | 10/10 sudden = SAH, aortic dissection, testicular torsion - emergencies |
SUMMARY QUICK-REFERENCE MAP
LOCATION THINK OF
─────────────────────────────────────────────────────
Head (thunderclap) → SAH
Head (unilateral) → Migraine / Cluster
Temple (elderly) → GCA
Jaw/arm + chest → MI/Angina
Tearing chest→back → Aortic dissection
Sharp chest,posture → Pericarditis
Pleuritic chest → PE / Pleurisy / Pneumonia
Epigastric (meals) → PUD (gastric/duodenal ulcer)
Epigastric→back → Pancreatitis
RUQ + fat meal → Cholecystitis / Biliary
RUQ + right shoulder→ Liver / Gallbladder / subdiaphragmatic
LUQ + left shoulder → Splenic rupture (Kehr's sign)
Periumbilical→RLQ → Appendicitis
RLQ (young woman) → Ovarian torsion / Ectopic
LLQ (elderly) → Diverticulitis
Loin→groin (colicky)→ Ureteral calculus
Suprapubic + dysuria→ UTI
Shoulder tip → Diaphragmatic irritation (blood, pus, air)
Low back + legs → Disc prolapse / Cauda equina
Critical "Do Not Miss" Pain Presentations
- Worst headache of life → always rule out SAH (CT + LP)
- Tearing chest/back pain → aortic dissection until proven otherwise
- Epigastric pain in elderly/diabetic → may be silent MI - always do ECG
- Shoulder tip pain → free fluid/air under diaphragm (ruptured ectopic, perforated viscus, splenic rupture)
- Periumbilical → RLQ migration → appendicitis
- Pain out of proportion to examination → mesenteric ischemia
- Sudden severe testicular/scrotal pain → testicular torsion (6-hour window)
- Saddle anaesthesia + urinary retention + back pain → cauda equina emergency
Sources: Goldman-Cecil Medicine (25e); Textbook of Family Medicine (9e); Harrison's Principles of Internal Medicine (22e); Rosen's Emergency Medicine; Tintinalli's Emergency Medicine; Color Atlas of Human Anatomy
Acute coronary syndrom
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute coronary syndrome" management guidelines
Reading File
Reading File
Reading Article
PMID: 40014670
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I have rich, comprehensive material from Goldman-Cecil, Harrison's, and the 2025 ACC/AHA guidelines. Now let me compile the full, authoritative answer.
Acute Coronary Syndrome (ACS)
A complete clinical reference covering definition, pathophysiology, classification, diagnosis, risk stratification, and management - updated to the 2025 ACC/AHA guidelines (PMID: 40014670).
1. DEFINITION & CLASSIFICATION
Acute Coronary Syndrome describes the clinical continuum of myocardial ischemia and infarction caused by acute reduction in coronary blood flow.
ACS
┌────────┴────────┐
ST-Elevation No ST-Elevation
(STEMI) (NSTE-ACS)
┌────────┴────────┐
NSTEMI Unstable Angina
(troponin +) (troponin -)
| Type | ECG | Troponin | Mechanism |
|---|---|---|---|
| STEMI | Persistent ST elevation >20 min | Elevated | Complete occlusion of epicardial artery |
| NSTEMI | ST depression, T-wave changes, or normal | Elevated | Partial/subtotal occlusion |
| Unstable Angina | Variable, often normal | Normal | Plaque rupture without significant necrosis |
(Goldman-Cecil Medicine, 25e, Ch. 57)
2. PATHOPHYSIOLOGY
The sequence of events in Type 1 MI (the most common):
- Atherosclerotic plaque builds up in coronary artery wall over years
- Plaque rupture or erosion - thin fibrous cap tears, exposing lipid-rich core
- Platelet aggregation - platelets adhere to exposed collagen and lipids
- Thrombus formation - activation of coagulation cascade
- Partial occlusion → NSTEMI/UA; Complete occlusion → STEMI
- Myocardial ischemia → necrosis - begins at subendocardium, progresses outward (wavefront phenomenon)
Type 2 MI (oxygen supply-demand mismatch without plaque rupture):
- Supply reduced: severe hypotension, anemia, hypoxemia, coronary spasm (Prinzmetal angina), dissection
- Demand increased: tachycardia, severe hypertension, thyrotoxicosis
Risk Factors for Plaque Instability:
- Thin fibrous cap
- Large lipid core
- Inflammation (macrophage infiltration)
- Low shear stress zones (vessel bifurcations)
- Neovascularization of plaque
3. CLINICAL PRESENTATION
Typical Symptoms
- Retrosternal pressure, squeezing, or heaviness - often described as "elephant on chest"
- Radiation to left arm, neck, or jaw
- Duration: angina < 20 min; NSTEMI/STEMI ≥ 30 min (or persistent)
- Associated: diaphoresis, nausea, dyspnea, vomiting, syncope
Atypical Presentations (do NOT miss)
More common in women, elderly (>75 yrs), diabetics, and those with chronic kidney disease:
- Epigastric pain / indigestion
- Unexplained fatigue or weakness
- Dyspnea alone
- Jaw or arm pain without chest pain
- Sudden-onset dizziness or syncope
"Myocardial ischemia is highly likely if anginal symptoms are accompanied by ECG abnormalities or elevated troponin." - Goldman-Cecil Medicine
4. DIAGNOSIS
Step 1: ECG (within 10 minutes of presentation)
| ECG Finding | Significance |
|---|---|
| ST elevation ≥1 mm in ≥2 contiguous leads | STEMI - activate cath lab immediately |
| New LBBB | Treat as STEMI |
| ST depression | NSTEMI / ischemia |
| Deep T-wave inversion (≥3 mm), especially V1-V4 | Wellen's syndrome - proximal LAD stenosis |
| ST depression in V1-V3 + tall R waves | Posterior STEMI - mirror image |
| Normal ECG | Does not exclude ACS (seen in ~5% of MI) |
ECG Localization of Infarct:
| Leads Affected | Territory | Artery |
|---|---|---|
| V1-V4 | Anterior | LAD |
| I, aVL, V5-V6 | Lateral | LCx or Diagonal |
| II, III, aVF | Inferior | RCA (or LCx) |
| V1-V2 (tall R waves, ST depression) | Posterior | RCA or LCx |
| V1, V4R | Right ventricle | RCA (proximal) |
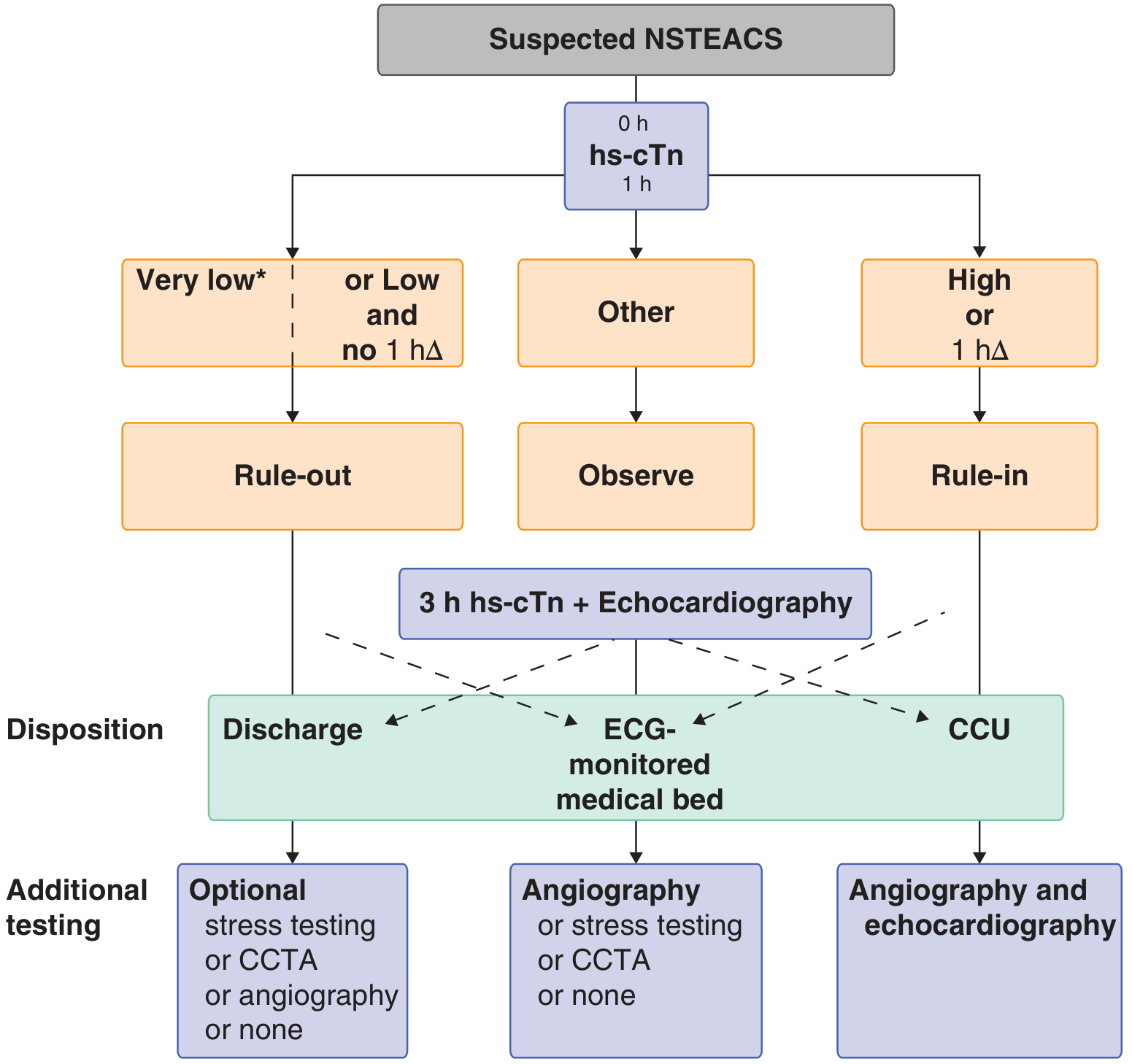
Step 2: Troponin (High-Sensitivity, hs-cTn)
- Measure at 0 h and 1 h (or 0 h and 3 h)
- Rule-in: hs-cTn very high at 0 h OR significant rise (delta) at 1 h
- Rule-out: hs-cTn very low at 0 h OR low + no delta at 1 h
Causes of elevated troponin that are NOT ACS (must differentiate):
Myocarditis, heart failure, cardiomyopathy, PE, stroke/SAH, sepsis, CKD, Takotsubo, cardiac contusion, ablation, defibrillator shocks, strenuous exercise
Step 3: Diagnostic Pathway - HEART Score
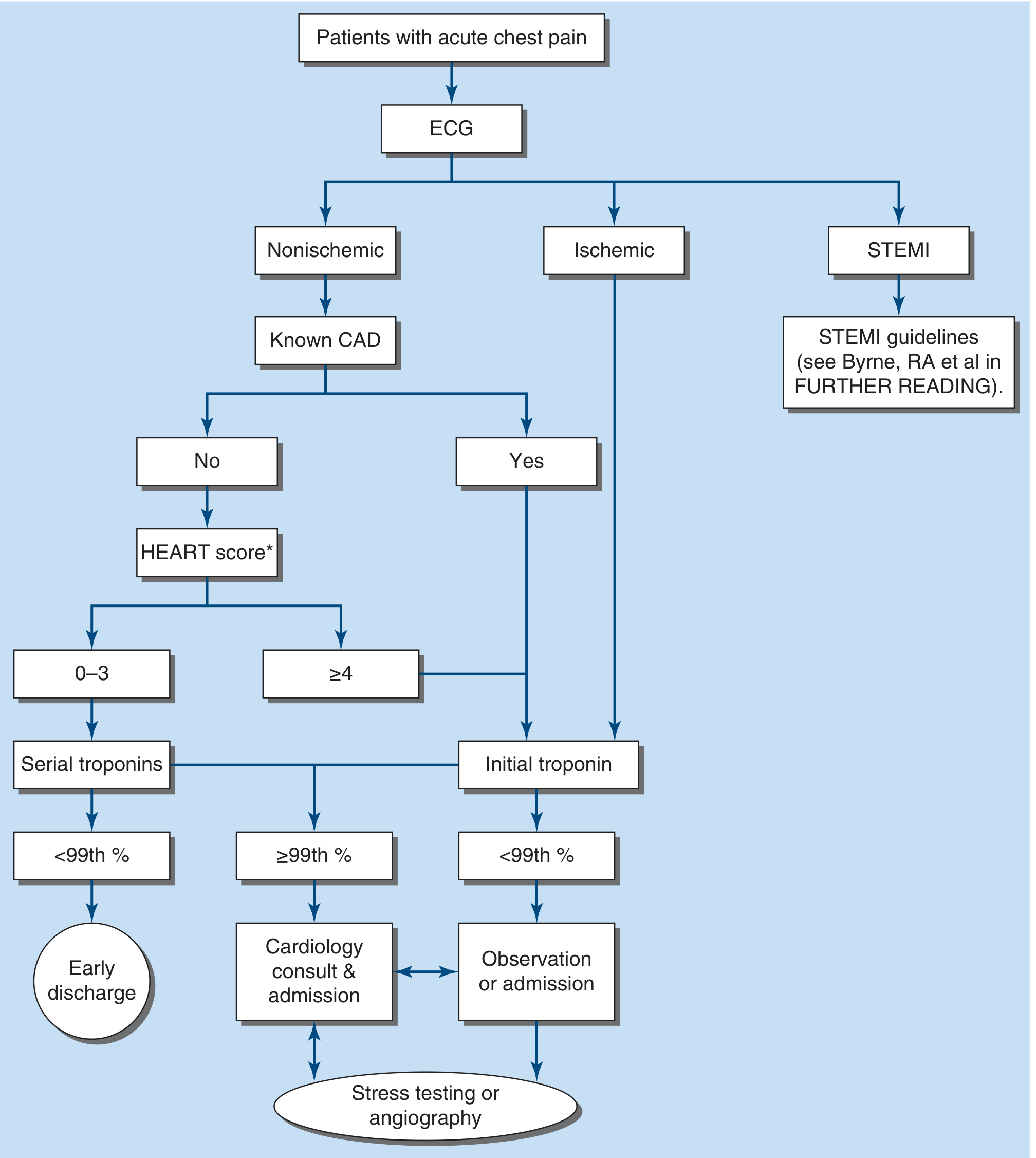
HEART Score (each 0-2 points):
- H - History (typical/atypical/non-cardiac features)
- E - ECG (normal / non-specific changes / ST deviation)
- A - Age (< 45 / 45-65 / > 65)
- R - Risk factors (none / 1-2 / ≥3 or known atherosclerosis)
- T - Troponin (normal / 1-3x / >3x ULN)
| Score | Risk | Action |
|---|---|---|
| 0-3 | Low | Serial troponins; early discharge if negative |
| ≥4 | High | Cardiology consult + admission |
Additional Tests
- Echo: Wall motion abnormalities, LV function, rule out pericarditis/PE
- CXR: Pulmonary congestion, widened mediastinum (dissection)
- Coronary CTA: In low-intermediate risk, no clear ECG changes
- Stress test: After ruling out ACS in intermediate-risk patients
5. RISK STRATIFICATION
(Harrison's 22e; Goldman-Cecil Medicine, Ch. 57)
TIMI Score for NSTE-ACS (0-7 points)
Each scores 1 point:
- Age ≥ 65 years
- ≥ 3 CAD risk factors (HTN, DM, hyperlipidaemia, smoking, family history)
- Known CAD (prior stenosis ≥ 50%)
- ST deviation > 0.5 mm on presenting ECG
- ≥ 2 anginal events in prior 24 hours
- Aspirin use in prior 7 days (suggests aspirin-resistant/refractory disease)
- Elevated cardiac markers (troponin or CK-MB)
| TIMI Score | 14-day Risk of MACE |
|---|---|
| 0-1 | 5% |
| 2 | 8% |
| 3 | 13% |
| 4 | 20% |
| 5 | 26% |
| 6-7 | 41% |
GRACE Score Variables
Age, heart failure (Killip class), heart rate, systolic BP, ST deviation, cardiac arrest at presentation, serum creatinine, elevated cardiac markers. Available at outcomes-umassmed.org/grace.
6. MANAGEMENT
A. IMMEDIATE GENERAL MEASURES (ALL ACS)
"MONA" - though oxygen use is now targeted:
- M - Morphine: 2-4 mg IV for severe unrelieved pain (use cautiously in NSTEMI - may delay P2Y12 absorption)
- O - Oxygen: Only if SpO2 < 90% or signs of heart failure; do NOT give routinely
- N - Nitrates: SL/buccal 0.3-0.6 mg q5 min x3, then IV if persistent (avoid if: hypotension, RV infarct, PDE5 inhibitor use)
- A - Aspirin: 300-325 mg chewed immediately (loading dose), then 75-100 mg/day
+ Monitoring: Continuous ECG, pulse oximetry, IV access, bed rest, cardiac monitoring unit
B. ANTI-ISCHEMIC THERAPY
(Harrison's 22e, Table 285-3)
| Drug | Indication | Avoid When |
|---|---|---|
| Nitrates (SL or IV) | Relief of angina, recurrent ischemia, hypertension, LVF | Hypotension, RV infarct, recent PDE5 inhibitor, severe AS |
| Beta-blockers (metoprolol, atenolol) | All ACS - reduce O2 demand | HR <50, SBP <90, PR >0.24s, 2nd/3rd degree AVB, acute severe HF (Killip III/IV), severe asthma |
| Calcium channel blockers (diltiazem, amlodipine) | Vasospastic angina; beta-blocker contraindicated | SBP <90, pulmonary oedema, LV dysfunction; avoid short-acting nifedipine |
C. ANTIPLATELET THERAPY
(Harrison's 22e, Table 285-4; 2025 ACC/AHA Guidelines - PMID: 40014670)
Dual Antiplatelet Therapy (DAPT) = Aspirin + P2Y12 inhibitor
| Drug | Loading Dose | Maintenance | Notes |
|---|---|---|---|
| Aspirin | 150-325 mg PO | 75-100 mg/day | Give to all; non-enteric-coated |
| Clopidogrel | 300 mg (conservative) or 600 mg (if PCI planned) | 75 mg/day | Prodrug; CYP2C19 variability; weaker |
| Ticagrelor | 180 mg | 90 mg BID | Preferred over clopidogrel; reversible; reduces mortality; can cause dyspnea |
| Prasugrel | 60 mg | 10 mg/day (5 mg if <60 kg or >75 yrs) | Only after coronary anatomy known; contraindicated if prior TIA/stroke |
| Cangrelor (IV) | 30 mcg/kg bolus | 4 mcg/kg/min infusion | At time of PCI; bridging |
DAPT Duration:
- ACS + PCI: minimum 12 months (can extend to 30 months in selected patients with low bleed risk)
- After 12 months, consider P2Y12 monotherapy (ticagrelor 60 mg BID) as per 2025 ACC/AHA guidelines
D. ANTICOAGULATION
| Drug | Dose | Use |
|---|---|---|
| Unfractionated heparin (UFH) | 60-70 units/kg IV bolus (max 5000 U), then 12-15 units/kg/h | All ACS; reversible with protamine |
| Enoxaparin (LMWH) | 1 mg/kg SC q12h | Preferred in NSTEMI managed conservatively; reduce dose in renal impairment |
| Fondaparinux | 2.5 mg SC daily | Low bleeding risk; caution - needs UFH during PCI (catheter thrombus risk) |
| Bivalirudin | 0.1 mg/kg bolus + 0.25 mg/kg/h | Preferred in high bleeding risk patients undergoing PCI |
E. REPERFUSION STRATEGY
STEMI - TIME IS MUSCLE
Target: Total ischemic time < 120 minutes from symptom onset
Primary PCI (preferred - if available):
- Door-to-balloon time: < 90 minutes (if PCI-capable center)
- Door-to-balloon time: < 120 minutes (if transfer needed)
- Preferred over thrombolysis in all settings where achievable within timeframes
Fibrinolysis (thrombolysis) - when PCI not available within 120 min:
- Give within 12 hours of symptom onset (best results < 3 hours)
- Preferred agents: Tenecteplase (weight-based single IV bolus), Alteplase, Streptokinase
- Contraindications to thrombolysis:
| Absolute | Relative |
|---|---|
| Prior intracranial hemorrhage | Severe uncontrolled HTN (>180/110) |
| Known structural cerebral vascular lesion | Prior ischemic stroke >3 months ago |
| Intracranial malignancy | Traumatic/prolonged CPR |
| Significant closed head trauma <3 months | Recent (< 2-4 weeks) internal bleed |
| Active internal bleeding | Pregnancy |
| Suspected aortic dissection | Active peptic ulcer |
| Anticoagulant therapy |
Post-thrombolysis: transfer for coronary angiography within 3-24 hours (pharmacoinvasive strategy)
NSTEMI - Timing of Invasive Strategy
| Risk Level | Strategy | Timing |
|---|---|---|
| Very high risk (hemodynamic instability, refractory ischemia, acute severe HF, cardiogenic shock, malignant arrhythmia) | Immediate PCI | < 2 hours |
| High risk (GRACE score >140, troponin rise, dynamic ECG changes, TIMI ≥ 3) | Early invasive | < 24 hours |
| Intermediate risk | Invasive | < 72 hours |
| Low risk | Conservative - stress test or CCTA | Before discharge |
F. ADDITIONAL MEDICAL THERAPY
| Drug | Indication | Dose |
|---|---|---|
| Statin (high-intensity) | All ACS - start immediately regardless of cholesterol | Atorvastatin 40-80 mg or Rosuvastatin 20-40 mg |
| ACE inhibitor / ARB | All ACS, especially if EF <40%, diabetes, hypertension | Ramipril, Lisinopril (start within 24h if stable) |
| Beta-blocker (long-term) | All post-MI, especially if EF <40% | Metoprolol succinate, Carvedilol, Bisoprolol |
| Aldosterone antagonist | EF <40% + HF symptoms or diabetes | Eplerenone or Spironolactone; monitor K+/renal function |
| Colchicine | Post-MI inflammation reduction (new - 2025 guidelines) | 0.5 mg BID |
7. COMPLICATIONS OF ACS
Mechanical
| Complication | Timing | Presentation |
|---|---|---|
| Acute MR (papillary muscle rupture) | Days 3-5 | Sudden pulmonary oedema + new murmur |
| VSD (ventricular septal defect) | Days 3-7 | Biventricular failure + new loud pansystolic murmur |
| Free wall rupture | Days 3-7 | Sudden cardiac death / tamponade |
| LV aneurysm | Weeks | Persistent ST elevation, HF, thrombus |
Electrical
- VF/VT: Most common cause of death in first hours (pre-hospital)
- Complete heart block: Inferior STEMI (RCA) - may need temporary pacing
- RBBB / LBBB: Anterior STEMI (LAD); new LBBB = poor prognosis
Haemodynamic
Killip Classification:
| Killip Class | Features | Mortality |
|---|---|---|
| I | No HF | ~5% |
| II | Mild HF (basal crackles, S3, elevated JVP) | ~10% |
| III | Acute pulmonary oedema | ~40% |
| IV | Cardiogenic shock (SBP <90 + poor perfusion) | ~50-80% |
Cardiogenic Shock: Norepinephrine (vasopressor) + Dobutamine (inotrope) + urgent PCI; consider IABP or Impella
8. SECONDARY PREVENTION (POST-ACS)
| Intervention | Target |
|---|---|
| Aspirin | 75-100 mg lifelong |
| P2Y12 inhibitor | ≥ 12 months post-ACS/PCI |
| High-intensity statin | LDL-C < 1.4 mmol/L (< 55 mg/dL) |
| ACE inhibitor/ARB | Blood pressure control + cardiac remodeling prevention |
| Beta-blocker | Minimum 1 year; longer if EF reduced |
| Cardiac rehabilitation | Structured exercise program |
| Smoking cessation | Reduces re-infarction risk by 50% |
| BP control | < 130/80 mmHg |
| Glucose control in DM | HbA1c target |
| Vaccination | Annual flu + COVID |
9. QUICK CLINICAL SUMMARY
STEMI → ECG in <10 min → Activate cath lab → PCI < 90 min
↓ (if PCI unavailable)
Thrombolysis < 12 h of onset
NSTEMI/UA → Risk stratify (TIMI/GRACE/HEART)
↓
Low risk → Serial troponin + stress test
High risk → PCI < 24-72 hours
↓
ALL ACS: Aspirin + P2Y12 + anticoagulation + beta-blocker + statin + ACEi
2025 Update: The landmark 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline (Rao SV et al., Circulation 2025 - PMID: 40014670) replaces all prior separate STEMI and NSTEMI guidelines into a single unified document, incorporating new evidence on colchicine, de-escalation strategies for DAPT, and P2Y12 monotherapy post-PCI.
Sources: Goldman-Cecil Medicine (25e), Ch. 57-58; Harrison's Principles of Internal Medicine (22e), Ch. 285; Rosen's Emergency Medicine (9e); 2025 ACC/AHA ACS Guideline (PMID: 40014670)
This is a shared conversation. Sign in to Orris to start your own chat.