Hypothalamic pituitary acis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed to write a comprehensive response. Let me compile everything.
The Hypothalamic-Pituitary Axis (HPA)
The hypothalamic-pituitary axis is the central command-and-control system of the endocrine body. The hypothalamus integrates neural signals and secretes hormones that regulate the pituitary, which in turn controls virtually all other endocrine glands.
Anatomy
The pituitary gland (hypophysis) sits in the sella turcica of the anterior cranial fossa, in close proximity to the optic chiasm. It connects to the hypothalamus via the pituitary stalk (infundibulum).
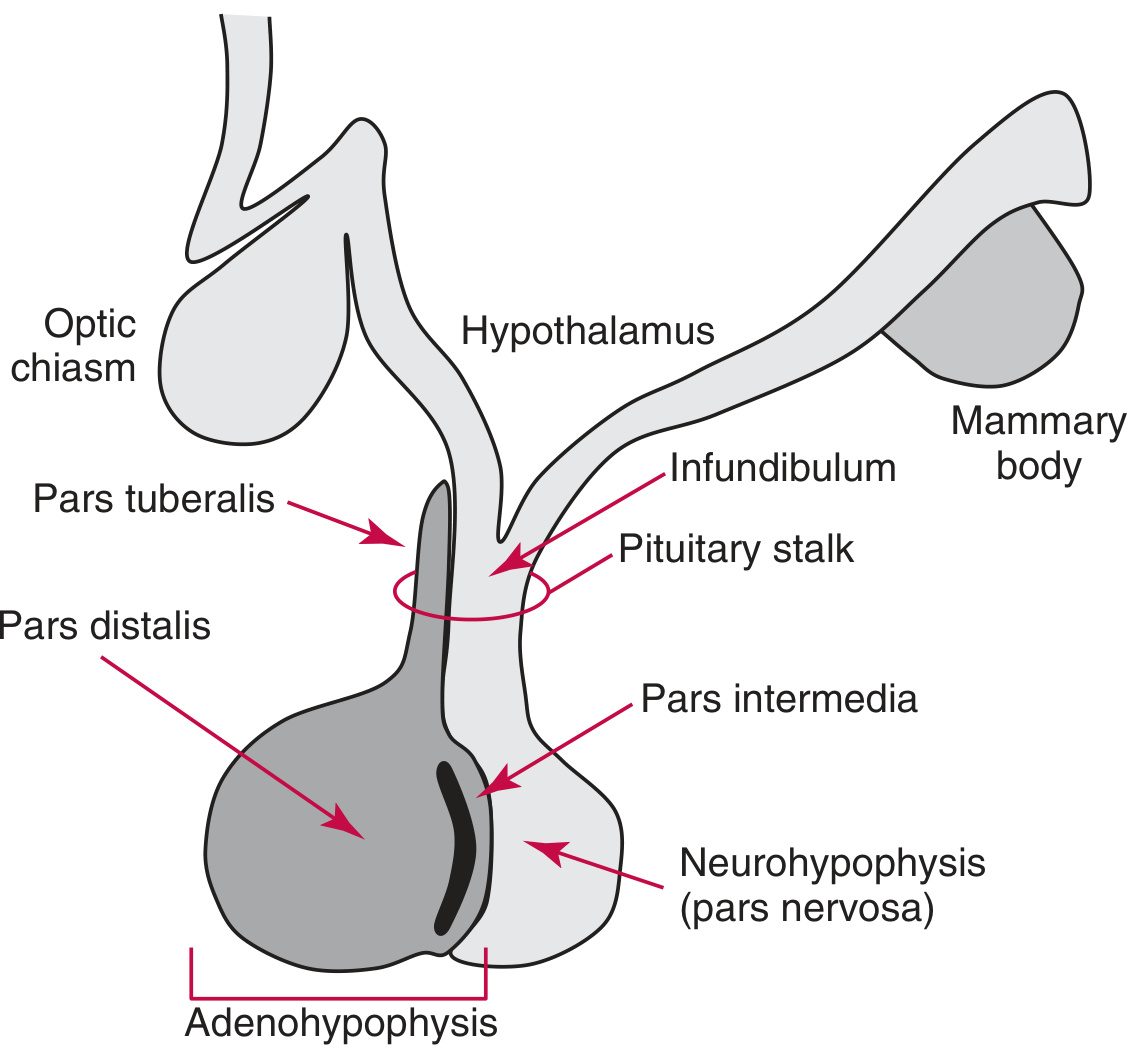
The pituitary has two distinct lobes:
1. Adenohypophysis (Anterior Pituitary) - ~75% of mass
Has three subdivisions:
- Pars distalis - where most hormone-producing cells reside
- Pars tuberalis - part of the pituitary stalk
- Pars intermedia - intermediate lobe
2. Neurohypophysis (Posterior Pituitary) - ~25% of mass
- Also called the pars nervosa
- Derived from brain neuroectoderm (a downward extension of the third ventricle floor)
- Functions as a reservoir, not a true endocrine organ - the cell bodies are actually in the hypothalamus
The Hypothalamic-Pituitary Portal System
The link between hypothalamus and anterior pituitary is the hypophyseal portal system: a network of blood vessels that carries hypothalamic-releasing and inhibitory hormones directly from the median eminence of the hypothalamus down the pituitary stalk into the anterior pituitary sinuses. This portal arrangement delivers very high concentrations of regulatory hormones directly to the target cells.
The hypothalamic neurons project axons to the median eminence, release hormones into portal vessels, and those hormones are then transported directly to gonadotrophs, thyrotrophs, corticotrophs, somatotrophs, and lactotrophs in the anterior pituitary.
- Medical Physiology (Boron & Boulpaep)
Anterior Pituitary - Hormones and Regulation
The anterior pituitary produces 6 key hormones, controlled by hypothalamic-releasing or inhibitory hormones:
| Hypothalamic Hormone | Structure | Effect on Anterior Pituitary |
|---|---|---|
| TRH (Thyrotropin-releasing hormone) | Tripeptide (pyroGlu-His-Pro) | Stimulates TSH release by thyrotrophs |
| GnRH (Gonadotropin-releasing hormone) | 10 amino acid peptide | Stimulates LH and FSH release by gonadotrophs |
| CRH (Corticotropin-releasing hormone) | 41 amino acid peptide | Stimulates ACTH release by corticotrophs |
| GHRH (Growth hormone-releasing hormone) | 44 amino acid peptide | Stimulates GH release by somatotrophs |
| Somatostatin (GHIH) | 14 amino acid peptide | Inhibits GH (and to a lesser extent, TSH) |
| Dopamine (PIH) | Catecholamine | Inhibits prolactin synthesis and secretion |
Source: Guyton and Hall Textbook of Medical Physiology, Table 76.2
The six anterior pituitary hormones and their roles:
- GH (Growth Hormone) - promotes growth and metabolism; regulated by GHRH/somatostatin
- TSH (Thyroid-stimulating hormone) - regulates thyroid hormone synthesis
- ACTH (Adrenocorticotropic hormone) - drives cortisol secretion from adrenal cortex
- FSH (Follicle-stimulating hormone) - spermatogenesis (male); follicle development (female)
- LH (Luteinizing hormone) - testosterone in Leydig cells (male); ovulation & progesterone (female)
- Prolactin - stimulates lactation; uniquely under tonic inhibition by dopamine
Posterior Pituitary - Hormones
The posterior pituitary secretes 2 hormones (actually synthesized in the hypothalamus and transported down axons):
| Hormone | Synthesized In | Function |
|---|---|---|
| ADH (Vasopressin/AVP) | Supraoptic nucleus | Water reabsorption (V2 receptor in renal collecting ducts); vasoconstriction (V1a) |
| Oxytocin | Paraventricular nucleus | Uterine contractions; milk let-down; social bonding |
Both are nonapeptides with a cyclic hexapeptide ring and differ in only 2 amino acid positions. They are transported down axons as complexes with neurophysins and released from the nerve terminals in the posterior pituitary into systemic circulation.
Feedback Control Loops
The HPA operates through three feedback mechanisms:
1. Long-loop Negative Feedback
The most important mechanism - peripheral hormones (cortisol, thyroid hormones, sex steroids) feed back on both the hypothalamus and the pituitary to suppress releasing hormone and tropic hormone secretion. Example: rising plasma T3/T4 suppresses both TRH (hypothalamus) and TSH (pituitary).
2. Short-loop Feedback
Pituitary hormones travel retrograde through the portal system back to the hypothalamus to inhibit their own releasing hormones.
3. Ultrashort-loop Feedback
Hypothalamic releasing hormones can act on the hypothalamic neurons themselves.
The Three Major Axes in Detail
HP-Thyroid Axis (HPT)
- Hypothalamus → TRH → Anterior pituitary → TSH → Thyroid → T3/T4
- T3/T4 feed back to suppress TRH and TSH
- TSH binds Gs-coupled receptor on thyroid follicular cells → cAMP → hormone synthesis
- Clinical note: The advent of ultrasensitive TSH assays (detection limit ≤0.01 mIU/L) has made TRH stimulation testing obsolete in assessing thyroid function.
- Tietz Textbook of Laboratory Medicine, 7th Ed.
HP-Adrenal Axis (HPA)
- Hypothalamus → CRH → Anterior pituitary → ACTH → Adrenal cortex → Cortisol
- Cortisol feeds back to suppress both CRH and ACTH
- Has a prominent diurnal rhythm - cortisol peaks in the morning (~5-23 µg/dL at 8 AM)
- The cosyntropin (Synacthen) stimulation test (250 µg IV/IM) evaluates adrenal reserve
- The insulin tolerance test (ITT) is the gold standard for assessing entire HPA axis integrity but carries seizure risk
- Tietz Textbook of Laboratory Medicine, 7th Ed.
HP-Gonadal Axis (HPG)
- Hypothalamus → GnRH (pulsatile) → Anterior pituitary → LH + FSH → Gonads → sex steroids + gametes
- GnRH neurons originate in the olfactory placode embryologically, then migrate to the hypothalamus
- GnRH is encoded on chromosome 8 and is synthesized as a 69-amino-acid prohormone, cleaved to give the 10-amino-acid active peptide
- Pulsatile GnRH is essential - continuous GnRH (as with GnRH agonist therapy) desensitizes gonadotrophs and suppresses the axis
- Kisspeptin (encoded by KiSS-1 gene) is a key upstream stimulator of GnRH release; mutations in kisspeptin receptor GPR-54 cause idiopathic hypogonadotropic hypogonadism with absent/delayed puberty
- Medical Physiology (Boron & Boulpaep); Textbook of Family Medicine 9e
Other Regulatory Factors
- GABA - may play a role in GH secretion (an area of active research)
- GnRH-associated peptide (GAP) - co-secreted with GnRH; role unclear
- hCG - can be produced by the pituitary in peri/postmenopausal women (not just in pregnancy)
- Stress, diurnal light-dark cycles, and body fat stores all modulate GnRH/hypothalamic secretion via neuronal inputs from the limbic system and other brain regions
Non-endocrine Hypothalamic Functions (Beyond Pituitary Control)
The hypothalamus also regulates:
- Appetite and satiety
- Body temperature
- Sleep-wake cycles
- Autonomic nervous system activity
Clinical Summary
| Disorder | Mechanism |
|---|---|
| Central hypothyroidism | TRH or TSH deficiency → low T3/T4 |
| Central hypogonadism (Kallmann syndrome) | GnRH deficiency (often with anosmia) |
| Cushing's disease | ACTH-secreting pituitary adenoma (corticotroph) |
| Acromegaly | GH-secreting pituitary adenoma (somatotroph) |
| Hyperprolactinemia | Prolactinoma or dopamine pathway disruption (stalk effect) |
| Diabetes insipidus (central) | ADH deficiency - supraoptic nucleus destruction |
| SIADH | Excess ADH - excess water retention |
| Idiopathic hypogonadotropic hypogonadism | GPR-54 (kisspeptin receptor) mutation → no GnRH drive |
Sources:
- Guyton and Hall Textbook of Medical Physiology - Table 76.2, Hypothalamic Releasing/Inhibitory Hormones
- Textbook of Family Medicine 9e, Chapter 35 (Hypothalamic-Pituitary Axis)
- Medical Physiology (Boron & Boulpaep) - HPT and HPG axis chapters
- Tietz Textbook of Laboratory Medicine, 7th Ed. - Chapter 55 (Laboratory assessment of HPA, HPT, HPG axes)
This is a shared conversation. Sign in to Orris to start your own chat.