Details anatomy of oropharynx nashopharynx and tonsils in detail for the ENT posting
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have all the material needed to write a comprehensive, well-structured anatomy answer. Let me compile it:
Anatomy of the Nasopharynx, Oropharynx, and Tonsils
(Scott-Brown's Otorhinolaryngology, K.J. Lee's Essential Otolaryngology, Gray's Anatomy for Students, Pfenninger & Fowler's Procedures for Primary Care)
THE PHARYNX - Overview
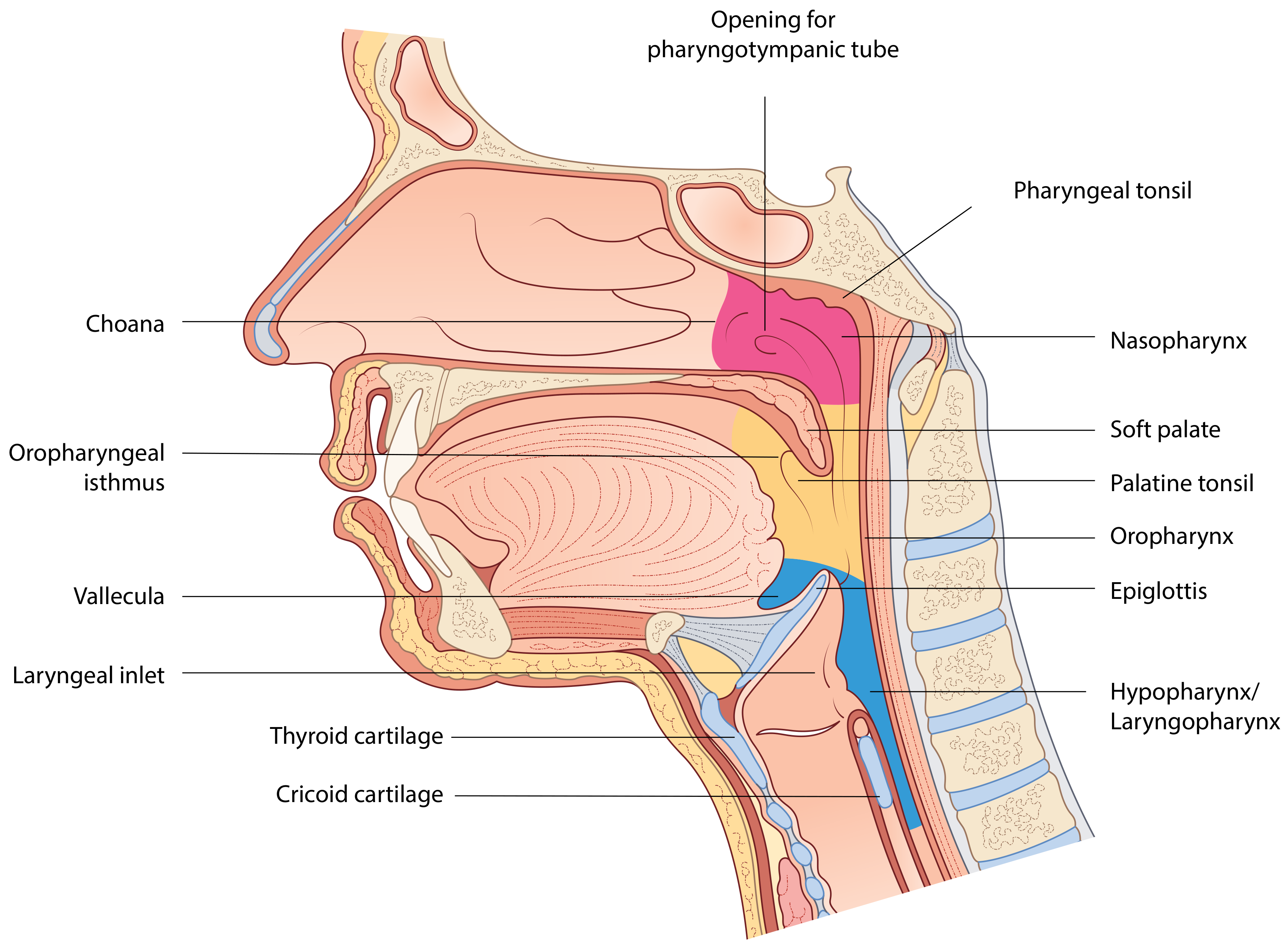
The pharynx is a 12-14 cm long musculofascial tube shaped like an inverted cone. It hangs from the pharyngeal tubercle at the skull base and fuses with the oesophagus at the lower border of the cricoid cartilage (C6 vertebra). It is the common aerodigestive pathway shared by respiration and digestion, and its mucosal lining is continuous with the nasal cavity, oral cavity, auditory tubes, and larynx.
Functions: directs air into the laryngeal inlet; directs food into the digestive tract; aids pressure equalization in the middle ear via the Eustachian tube; assists vocalization.
Subdivisions (boundaries arbitrary, based on anterior communications):
| Subdivision | Limits |
|---|---|
| Nasopharynx | Base of skull → level of soft palate |
| Oropharynx | Junction of hard/soft palate → upper margin of epiglottis (hyoid level) |
| Hypopharynx (laryngopharynx) | Level of hyoid → inferior border of cricoid |
1. NASOPHARYNX
Boundaries
- Superior/posterior wall (roof): Sloping basisphenoid and basal occipital bone (contiguous due to the slope - collectively the "basisphenoid"). The roof and posterior wall are often described together.
- Anterior: Right and left choanae (posterior nasal apertures), separated by the vomer; also the posterior ends of the inferior and middle conchae project into the choanae.
- Lateral walls: Bear the pharyngotympanic (Eustachian) tube openings and important recesses.
- Floor: Formed by the soft palate (the only mobile wall). When the soft palate is elevated, the nasopharynx is separated from the oropharynx.
- Communicates below with the oropharynx via the pharyngeal isthmus (posterior to soft palate, anterior to the posterior pharyngeal wall).
Key point: Unlike the oro- and laryngopharynx, the walls of the nasopharynx are rigid (except the soft palate), keeping the cavity always patent for airflow.
Key Structures on Lateral Wall
-
Pharyngotympanic (Eustachian) tube orifice - located approximately 1-1.5 cm from the posterior end of the inferior turbinate, at the level of the superior border of the palate (floor of the nose). It connects the middle ear to the nasopharynx and transiently opens and closes to equalize tympanic membrane pressure.
-
Torus tubarius - a cartilaginous projection covering the pharyngotympanic orifice, orientated posterosuperiorly, with a longer posterior extension giving it a comma-shaped appearance on endoscopy. It forms the anterior boundary of the fossa of Rosenmüller.
-
Fossa of Rosenmüller (pharyngeal recess) - a deep recess situated posterosuperior to the torus tubarius. Its floor is the superior constrictor and its superior/posterior border is the skull base. This is the most common site of origin for nasopharyngeal carcinoma (NPC) and should be targeted during biopsies of the nasopharynx when investigating carcinoma of unknown primary.
-
Salpingopharyngeal fold - a mucosal fold projecting inferiorly from the cartilaginous ridge of the pharyngotympanic tube orifice, overlying the salpingopharyngeus muscle and the levator veli palatini, both of which pass inferiorly and laterally to merge with the lateral pharyngeal wall.
-
Torus levatorius - a broad fold/elevation that appears to emerge from below the pharyngotympanic tube opening, continuing medially onto the upper surface of the soft palate, overlying the levator veli palatini.
-
Tubal tonsils (Gerlach's tonsils) - small lymphoid nodules at the lip of the fossa of Rosenmüller, posterior to the torus tubarius. They constitute an additional component of Waldeyer's ring when present.
Epithelium
- Anteriorly (near choanae): Respiratory epithelium - pseudostratified ciliated columnar with goblet cells.
- Posteriorly (towards oro-/laryngopharynx): Non-keratinized stratified squamous epithelium.
- At the transitional zone where the two meet, columnar (not ciliated) epithelium is found instead of cilia - this is the zone of highest carcinogenic risk in NPC.
2. OROPHARYNX
Boundaries
- Superior: Junction of hard and soft palate / pharyngeal isthmus
- Inferior: Upper margin of epiglottis / plane of hyoid bone / valleculae
- Anterior: Oropharyngeal isthmus (opening between palatoglossal folds), continuous with the oral cavity; base of tongue (posterior 1/3) forms the anterior wall below the isthmus
- Lateral walls: Bear the palatine tonsils between the tonsillar pillars
- Posterior wall: Upper part overlies C2-C3 vertebrae
Subunits (K.J. Lee)
- Soft palate and uvula
- Base of tongue (posterior 1/3, pharyngeal part)
- Palatine arch - includes tonsillar fossae, palatine tonsils, anterior and posterior pillars (palatoglossal and palatopharyngeal arches)
- Lateral and posterior oropharyngeal walls
- Valleculae and pharyngoepiglottic/glossoepiglottic folds
Oropharyngeal Isthmus
The palatoglossal folds (arches) on each side, overlying the palatoglossal muscles, mark the boundary between the oral cavity and oropharynx. The arched opening between them is the oropharyngeal isthmus.
Posterior and medial to these are the palatopharyngeal folds (arches), overlying the palatopharyngeal muscles.
- To hold food/liquid in mouth: Isthmus closed by depression of soft palate + elevation of back of tongue + medial movement of palatoglossal/palatopharyngeal folds - allows breathing while chewing.
- On swallowing: Isthmus opens, palate elevates (closing nasopharynx), laryngeal cavity closes - person cannot breathe and swallow simultaneously.
Tonsillar Fossa (Sinus Tonsillaris)
- Superior: Soft palate
- Inferior: Lingual tonsil
- Anterior (anterior pillar): Palatoglossus muscle
- Posterior (posterior pillar): Palatopharyngeus muscle
- Deep/medial wall: Superior constrictor muscle (covered by the pharyngobasilar fascia and tonsillar capsule)
Valleculae
Paired mucosal pouches between the base of tongue and the epiglottis, one on each side of the midline. Bounded by:
- Midline: glossoepiglottic fold
- Lateral: pharyngoepiglottic folds
3. TONSILS AND WALDEYER'S RING
Waldeyer's ring is a complete ring of lymphoid tissue surrounding the openings of the nasal and oral cavities - forming the first-line immunological defense of the upper respiratory tract.
Components of Waldeyer's Ring
| Component | Location |
|---|---|
| Pharyngeal tonsil (adenoids) | Midline roof/posterior wall of nasopharynx |
| Palatine tonsils | Lateral oropharynx, between palatoglossal and palatopharyngeal arches |
| Lingual tonsils | Posterior 1/3 (base) of tongue |
| Tubal tonsils (Gerlach's tonsils) | Posterior to torus tubarius, lip of fossa of Rosenmüller |
| Lateral pharyngeal bands | Lymphoid tissue behind posterior pillars |
Immunology: B lymphocytes proliferate in germinal centers. Tonsils produce IgG, IgA, IgM, IgD, complement components, interferon, lysozymes, and cytokines.
3a. Pharyngeal Tonsil (Adenoids)
| Feature | Detail |
|---|---|
| Size | Rapid growth in infancy; maximal at age 5; involutes at ages 8-10; atrophies in later life |
| Site | Roof and posterior wall of nasopharynx |
| Shape | Truncated pyramid with a vertically oriented median cleft; apex directed towards nasal septum; base at junction of roof and posterior wall |
| Surface | Free surface has anteriorly and laterally radiating folds from the bursa of Luschka (pharyngeal bursa) - a median blind recess extending posterosuperiorly into the tonsil |
| Epithelium | Predominantly respiratory (ciliated) on lateral/inferior parts; occasional patches of keratinized stratified squamous |
| Capsule | No clear plane of cleavage (unlike palatine tonsil) - attached via a connective tissue hemicapsule at the superior pole; this makes adenoidectomy less precise |
| Blood supply | Ascending pharyngeal artery, ascending palatine artery, tonsillar branch of facial artery, pharyngeal branch of maxillary artery, artery of pterygoid canal. Occasionally an emissary vessel from the inferior hypophysial artery supplies the nasopharyngeal bed (can cause persistent hemorrhage post-adenoidectomy) |
Clinical note on adenoidectomy: Blind curettage, suction diathermy, or suction microdebridement. During blind curettage, avoid hyperextending the cervical spine as the arch of the atlas (C1) may pierce through the prevertebral fascia and cause infection/instability.
3b. Palatine Tonsils
Large ovoid collections of lymphoid tissue on the lateral walls of the oropharynx, between the palatoglossal and palatopharyngeal arches, lying on the superior constrictor muscle. Visible through the open mouth posterior to the palatoglossal folds.
Structure: Covered by non-keratinized stratified squamous epithelium with deep crypts extending into the parenchyma. Has a well-defined fibrous capsule with a clear plane of cleavage from the superior constrictor, facilitating tonsillectomy - a key difference from the adenoid.
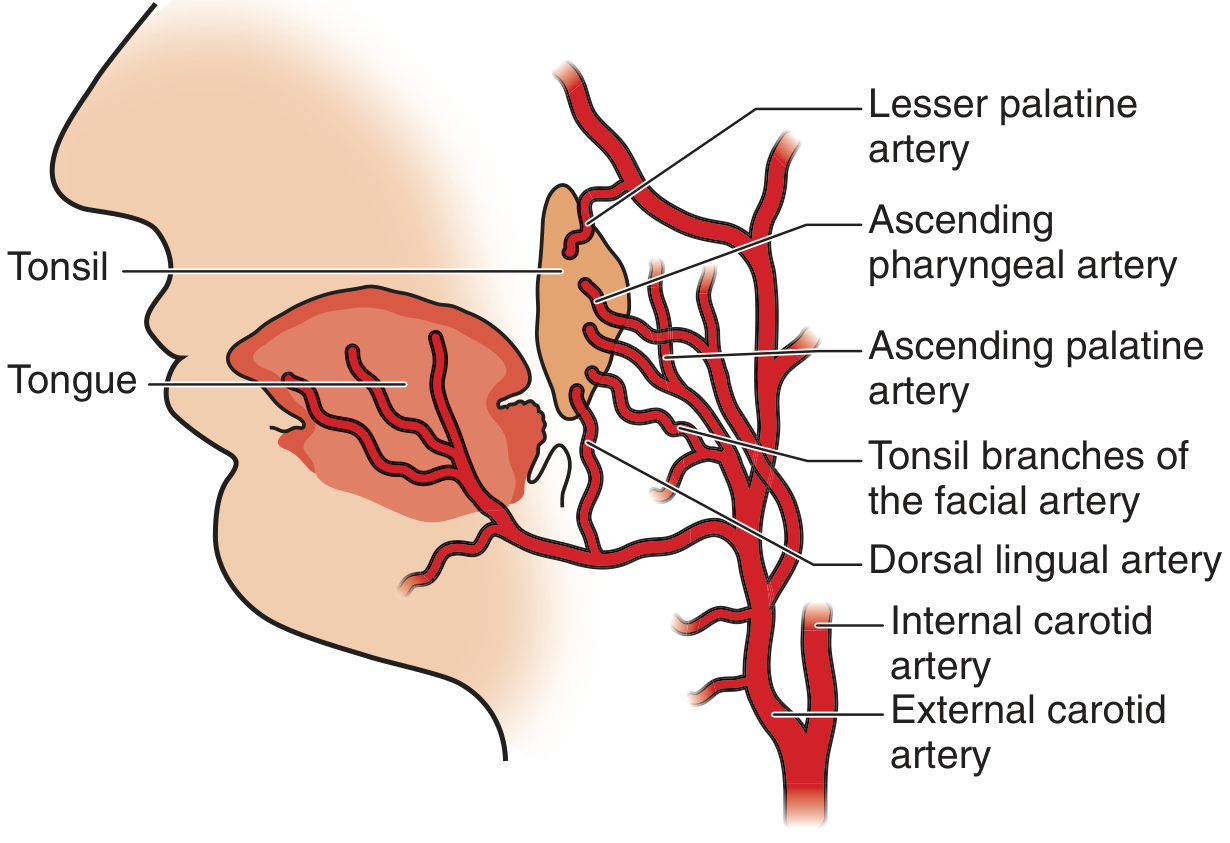
Arterial supply (5 branches from external carotid system):
| Artery | Pole Supplied |
|---|---|
| Tonsillar branch of facial artery (main branch) | Inferior pole |
| Ascending palatine artery (branch of facial) | Inferior pole |
| Dorsal lingual artery | Inferior pole |
| Ascending pharyngeal artery | Superior pole |
| Descending palatine → lesser palatine (from maxillary artery) | Superior pole |
Surgical note: The key to controlling brisk tonsillar bed bleeding is to direct efforts toward the superior or inferior poles first before trying to control every bleeder in the tonsillar bed, as the poles are the vascular points of entry.
Venous drainage: Paratonsillar vein (external palatine/paratonsillar vein) → pharyngeal plexus → internal jugular vein; also via facial vein.
Lymphatic drainage: Through the pharyngeal wall to jugulodigastric (tonsillar) nodes (the main nodes; part of deep cervical chain, at the level of the angle of the mandible, C2 vertebra).
Nerve supply (sensory): Glossopharyngeal nerve (CN IX) and lesser palatine nerve (V2 - branch of maxillary).
3c. Lingual Tonsils
Large collections of lymphoid tissue in the mucosa covering the pharyngeal part (posterior 1/3) of the tongue. Form the anterior wall of the oropharynx below the oropharyngeal isthmus.
4. SOFT PALATE
Muscles (5 muscles)
| Muscle | Origin | Action | Nerve |
|---|---|---|---|
| Palatoglossus (anterior pillar) | Palatine aponeurosis | Approximates palate to tongue; narrows oropharyngeal opening; involved in swallowing | CN X (vagus via pharyngeal plexus) |
| Palatopharyngeus (posterior pillar) | Palatine aponeurosis | Raises larynx and pharynx; closes oropharyngeal aperture; involved in breathing | CN X |
| Musculus uvulae | Posterior nasal spine | Shortens and elevates uvula | CN X |
| Levator veli palatini | Petrous temporal (inferior surface) + Eustachian tube cartilage | Raises soft palate to contact posterior pharyngeal wall during swallowing; closes pharyngeal isthmus | CN X |
| Tensor veli palatini | Scaphoid fossa + Eustachian tube cartilage | Pulls soft palate laterally, gives rigidity/firmness; opens Eustachian tube on swallowing | CN V3 (mandibular branch of trigeminal) - ONLY palatal muscle NOT supplied by CN X |
Function as a "flutter valve":
- Elevation (swallowing) → closes pharyngeal isthmus → seals nasopharynx from oropharynx (prevents reflux of food into nasopharynx).
- Depression → closes oropharyngeal isthmus → seals oral cavity from oropharynx (allows chewing and breathing simultaneously).
Blood supply of soft palate:
- Ascending palatine artery (from facial artery)
- Lesser palatine artery (from maxillary artery)
- Ascending pharyngeal artery
Venous drainage: Pharyngeal plexus → internal jugular vein; external palatine vein → tonsillar fossa → facial vein.
5. PHARYNGEAL MUSCLES
Outer Layer - Constrictors (3 overlapping constrictor muscles)
Function: narrow the pharyngeal cavity sequentially from top to bottom to move a food bolus into the esophagus. All supplied by CN X (vagus) via pharyngeal plexus.
| Muscle | Origin | Insertion | Key Notes |
|---|---|---|---|
| Superior constrictor | Pterygomandibular raphe + adjacent mandible and pterygoid hamulus | Median pharyngeal raphe | Forms deep wall of tonsil bed |
| Middle constrictor | Hyoid bone and stylohyoid ligament | Median raphe | |
| Inferior constrictor | Oblique line of thyroid cartilage + cricoid cartilage | Median raphe | Lower portion = cricopharyngeus (UES) |
Cricopharyngeus: Most inferior portion of inferior constrictor; acts as the upper esophageal sphincter (UES); under tonic contraction at rest and relaxes with swallowing.
Important gaps in pharyngeal walls (clinical relevance):
- Oropharyngeal triangle (Killian's dehiscence above): Gap between superior and middle constrictors and the posterior border of mylohyoid - allows passage of stylopharyngeus, styloglossus, hyoglossus, lingual artery/vein, lingual nerve, CN XII (hypoglossal), CN IX (glossopharyngeal), and lymphatics.
- Between middle and inferior constrictor: Internal laryngeal vessels and nerve pass to the thyrohyoid membrane.
- Below inferior constrictor: Recurrent laryngeal nerves and inferior laryngeal vessels.
- Killian's dehiscence: Triangular gap between the inferior constrictor and cricopharyngeus, through which a Zenker's (pharyngeal) diverticulum can herniate posteriorly.
- Killian-Jamieson space: Lateral dehiscence inferior to cricopharyngeus, through which branches of the inferior thyroid artery pass.
Inner Layer - Longitudinal Muscles (elevate the pharynx)
| Muscle | Origin | Insertion | Action | Nerve |
|---|---|---|---|---|
| Stylopharyngeus | Styloid process of temporal bone | Pharyngeal wall | Elevate pharynx | CN IX (glossopharyngeal) - only pharyngeal muscle by CN IX |
| Salpingopharyngeus | Cartilaginous pharyngotympanic tube | Pharyngeal wall | Elevate pharynx; opens tube | CN X |
| Palatopharyngeus | Upper surface of palatine aponeurosis | Pharyngeal wall; interdigitates with superior constrictor to create Passavant's ridge | Elevates pharynx; seals nasopharynx from oropharynx | CN X |
6. NERVE SUPPLY OF THE PHARYNX
| Region | Sensory Nerve |
|---|---|
| Nasopharynx | Pharyngeal branch of maxillary nerve (CN V2) |
| Oropharynx | Glossopharyngeal nerve (CN IX) via pharyngeal plexus - afferent limb of gag reflex |
| Laryngopharynx | Vagus (CN X) via internal laryngeal branch of superior laryngeal nerve |
Motor (all pharyngeal muscles except stylopharyngeus): Vagus nerve (CN X) via the pharyngeal plexus.
Stylopharyngeus: CN IX (glossopharyngeal).
7. BLOOD SUPPLY OF THE PHARYNX
Upper pharynx (branches of external carotid artery):
- Ascending pharyngeal artery
- Ascending palatine and tonsillar branches of facial artery
- Branches of maxillary and lingual arteries
Lower pharynx:
- Pharyngeal branches of inferior thyroid artery (from thyrocervical trunk of subclavian artery)
Venous drainage: Pharyngeal plexus → pterygoid plexus (infratemporal fossa) → facial and internal jugular veins.
8. LYMPHATIC DRAINAGE OF THE PHARYNX
- Nasopharynx: Retropharyngeal nodes → upper deep cervical nodes. The nasopharynx drains bilaterally, which explains the bilateral neck nodes often seen in NPC.
- Oropharynx/Tonsils: Jugulodigastric (tonsillar) nodes → deep cervical chain.
- Posterior pharyngeal wall: Retropharyngeal and paratracheal nodes → deep cervical nodes.
Key Clinical Correlates for ENT Posting
| Clinical Point | Anatomical Basis |
|---|---|
| Otitis media in children | Short, horizontal Eustachian tube at birth (half adult length) allows easier spread of infection between nasopharynx and middle ear |
| Nasopharyngeal carcinoma | Arises most commonly from the fossa of Rosenmüller; occurs at the transitional zone of squamous/respiratory epithelium |
| Adenoid hypertrophy | Blocks choanae → mouth breathing; Eustachian tube dysfunction → OME (glue ear) |
| Quinsy (peritonsillar abscess) | Pus collects between tonsillar capsule and superior constrictor; superior pole involvement common |
| Post-tonsillectomy hemorrhage | Superior and inferior poles are main vascular entry points; control poles first; internal carotid artery lies ~2.5 cm posterolateral (danger if superior constrictor violated) |
| Zenker's diverticulum | Herniation through Killian's dehiscence (gap between inferior constrictor and cricopharyngeus) |
| Gag reflex | Afferent: CN IX (oropharyngeal sensory); Efferent: CN X (motor to pharynx) |
| Passavant's ridge | Formed by palatopharyngeus interdigitating with superior constrictor; important in velopharyngeal closure |
| Adenoidectomy warning | No plane of cleavage in adenoid unlike palatine tonsil; avoid cervical hyperextension (C1 arch injury risk) |
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery (9781138094642, block 7) | K.J. Lee's Essential Otolaryngology (9781260122237, block 3) | Gray's Anatomy for Students (9780323934237, block 5) | Pfenninger & Fowler's Procedures for Primary Care (9780323052672, block 5)
This is a shared conversation. Sign in to Orris to start your own chat.