thiazide type diuretics can you tell me the meachanism of the action of the following drug in the managemnt of the hypertension in short simplified way
Thiazide Diuretics - Mechanism of Action in Hypertension
Step 1: Block the Na⁺/Cl⁻ Cotransporter
Result: More Na⁺ and Cl⁻ stay in the tubule and are excreted in urine.
Step 2: Short-term Effect - Volume Reduction
Result: Reduced blood volume (extracellular fluid) → lower cardiac output → lower blood pressure.
Step 3: Long-term Effect - Vasodilation
Result: Decreased peripheral vascular resistance (blood vessels relax).
Simple Summary
| Phase | Mechanism | Effect |
|---|---|---|
| Acute | Block Na⁺/Cl⁻ reabsorption in DCT | ↓ Blood volume → ↓ Cardiac output |
| Chronic | Sustained negative Na⁺ balance | ↓ Peripheral resistance → ↓ BP |
Common Thiazide Drugs
- Hydrochlorothiazide (HCTZ) - most commonly used
- Chlorthalidone - ~2x more potent than HCTZ, preferred by many guidelines
- Indapamide and metolazone - thiazide-like (same mechanism, slightly different structure)
What are the common adverse effects of thiazide diuretics?
Adverse Effects of Thiazide Diuretics
1. 🔽 Hypokalemia (Most Common)
- Thiazides increase Na⁺ delivery to the distal tubule, causing more K⁺ to be exchanged for Na⁺ - leading to continuous potassium loss
- Can cause muscle weakness, cramps, and dangerous cardiac arrhythmias
- Fix: Periodic K⁺ monitoring, potassium supplementation, or add a K⁺-sparing diuretic (e.g. amiloride)
- ⚠️ A low-sodium diet helps blunt K⁺ depletion
2. 🔽 Hyponatremia
- Due to elevated ADH levels, decreased diluting capacity of the kidney, and increased thirst
- Can cause fatigue, confusion, and in severe cases, seizures
3. 🔽 Hypomagnesemia
- Urinary magnesium loss can occur, which can worsen hypokalemia (low Mg makes K⁺ harder to correct)
4. 🔼 Hyperuricemia / Gout
- Thiazides compete with uric acid in the organic acid secretory system, reducing uric acid excretion
- Uric acid deposits in joints → can precipitate gout in susceptible patients
- Use with caution in gout patients
5. 🔼 Hyperglycemia / Worsening Diabetes
- Impaired insulin secretion (partly due to hypokalemia) raises blood glucose
- Can unmask latent diabetes mellitus
- Diabetic patients still benefit from thiazides but should monitor glucose more closely
6. 🔼 Hypercalcemia
- Thiazides inhibit Ca²⁺ excretion in the urine, so calcium accumulates in the blood
- (This effect is actually useful in treating kidney stones and osteoporosis)
7. 🔽 Hypotension / Hypovolemia
- Volume depletion can cause orthostatic hypotension (dizziness when standing up)
8. 🔼 Dyslipidemia
- May increase LDL cholesterol, total cholesterol, and triglycerides with long-term use
9. Erectile Dysfunction
- Incidence of erectile dysfunction is higher with thiazides compared to some other antihypertensive classes
10. Rare but Notable
- Photosensitivity and skin rashes
- Acute myopia and angle-closure glaucoma (especially in patients with sulfonamide allergy)
- Risk of lupus-like reactions (thiazides are sulfonamide derivatives)
- Potentially fatal: Hypokalemia-induced ventricular arrhythmias when combined with QT-prolonging drugs (e.g. quinidine, dofetilide)
Quick Reference Table
| Adverse Effect | Mechanism | Clinical Note |
|---|---|---|
| Hypokalemia | ↑ K⁺/Na⁺ exchange in DCT | Most common; monitor K⁺ |
| Hyponatremia | ↑ ADH + ↓ diluting capacity | Especially in elderly |
| Hyperuricemia | Competes with uric acid excretion | Avoid/caution in gout |
| Hyperglycemia | ↓ Insulin secretion via hypokalemia | Monitor glucose in diabetics |
| Hypercalcemia | ↓ Ca²⁺ excretion | Useful in nephrolithiasis |
| Dyslipidemia | Unknown | Long-term use |
| Orthostatic hypotension | Volume depletion | Start low, go slow |
hypertensive crisis '
Hypertensive Crisis
Definition
Classification
| Feature | Hypertensive Urgency | Hypertensive Emergency |
|---|---|---|
| BP | ≥ 180/120 mmHg | ≥ 180/120 mmHg |
| End-organ damage | ❌ Absent | ✅ Present (active, ongoing) |
| Symptoms | Asymptomatic or mild headache | Severe - encephalopathy, chest pain, vision loss |
| Setting | Outpatient / ED | ICU mandatory |
| Treatment | Oral agents | IV agents (titratable) |
| How fast to lower BP | Gradually over 24-48 hours | Controlled, not abruptly |
End-Organ Damage in Hypertensive Emergency
- 🧠 Brain: Hypertensive encephalopathy (headache, confusion, seizures, vision changes)
- ❤️ Heart: Acute left ventricular failure, acute MI, acute coronary syndrome
- 🫘 Kidney: Acute kidney injury, hematuria
- 🩸 Vessels: Acute aortic dissection
- 👁️ Eyes: Papilledema, retinal hemorrhages
- 🤰 Obstetric: Eclampsia / severe preeclampsia
- 🧪 Other: Pheochromocytoma crisis
Management
Step 1 - Assess Volume Status First
Step 2 - Rate of BP Reduction (Critical Rule)
⚠️ DO NOT lower BP too fast. Rapid or excessive reduction can cause cerebral, coronary, or renal ischemia due to impaired autoregulation.
- First hour: Reduce BP by no more than 25%
- Next 2-6 hours: Aim for BP ~160/100-110 mmHg
- Next 24-48 hours: Gradually normalize
| Condition | Target |
|---|---|
| Aortic dissection | SBP < 120 mmHg within 1 hour |
| Eclampsia / preeclampsia | SBP < 140 mmHg within 1 hour |
| Pheochromocytoma crisis | SBP < 140 mmHg within 1 hour |
Step 3 - IV Drugs for Hypertensive Emergency
| Drug | Class | Onset | Duration | Best Used In |
|---|---|---|---|---|
| Nicardipine | Ca²⁺ channel blocker | 5-15 min | 15-30 min | Most emergencies (except acute HF) |
| Clevidipine | Ca²⁺ channel blocker | 2-4 min | 5-15 min | Most emergencies |
| Labetalol | α+β blocker | 5-10 min | 3-6 h | Aortic dissection, pregnancy |
| Esmolol | β-blocker (ultra-short) | 1-2 min | 10-20 min | Aortic dissection, perioperative |
| Nitroglycerin | Nitrate vasodilator | 2-5 min | 5-10 min | Acute coronary ischemia, pulmonary edema |
| Sodium nitroprusside | Arteriolar + venous dilator | Immediate | 1-2 min | Caution - risk of cyanide toxicity; avoid in CNS emergencies |
| Fenoldopam | Dopamine-1 agonist | 5 min | 30 min | Protects renal perfusion; caution in glaucoma |
| Enalaprilat (IV) | ACE inhibitor | 15-30 min | 6 h | Acute HF, avoid in AKI |
| Hydralazine | Direct vasodilator | 10-20 min | 3-8 h | Eclampsia / pregnancy |
Step 4 - Hypertensive Urgency
- No IV drugs needed
- Restart, reinstate, or intensify oral antihypertensive agents
- Close outpatient follow-up
- Aggressive monitoring in this setting provides little added benefit
Key Points to Remember
- Urgency = no organ damage → oral drugs, outpatient
- Emergency = organ damage → IV drugs, ICU
- Never lower BP too fast - 25% max in the first hour
- Aortic dissection and eclampsia need faster, more aggressive control
- Avoid diuretics in most emergencies (patients are volume-depleted)
- Sublingual nifedipine is DANGEROUS - unpredictable BP drop can cause cerebral ischemia
dash diet for the hypertension'
DASH diet hypertension blood pressure reduction evidence 2024
DASH Diet for Hypertension
What is the DASH Diet?
What Does the DASH Diet Emphasize?
✅ EAT MORE of these:
| Food Group | Why it Helps |
|---|---|
| Fruits & Vegetables | High potassium content lowers BP |
| Whole grains | Fiber, nutrients, lowers cardiovascular risk |
| Low-fat dairy | Provides calcium and potassium |
| Nuts, seeds, legumes | Magnesium, potassium, healthy fats |
| Lean protein (fish, poultry) | Replaces red/processed meats |
❌ EAT LESS of these:
| Avoid | Reason |
|---|---|
| Sodium (salt) | Directly raises blood pressure |
| Saturated & trans fats | Worsens cardiovascular risk |
| Red & processed meats | High sodium + saturated fat |
| Sugary drinks & sweets | Empty calories, weight gain |
| Alcohol | Raises BP with excess intake |
Sodium Targets
- Optimal goal: < 1,500 mg sodium/day
- Minimum goal: Reduce by at least 1,000 mg/day from current intake
- WHO/Guidelines recommend: < 5 g of salt (90 mmol Na) per day
- Choose fresh foods over packaged/processed foods (>75% of sodium comes from processed/restaurant food)
- Use "no added salt" labels when shopping
- Avoid adding salt during cooking or at the table
- Control portion sizes when eating out
How Much Does DASH Lower Blood Pressure?
| Intervention | Expected SBP Reduction (Hypertensive) |
|---|---|
| DASH diet alone (feeding study) | -5.5/3.0 mmHg |
| DASH + behavior change | ~-4 mmHg SBP |
| DASH + low sodium (SBP ≥150) | Up to -20.8 mmHg SBP |
| Combined lifestyle package | ≥-10 mmHg SBP |
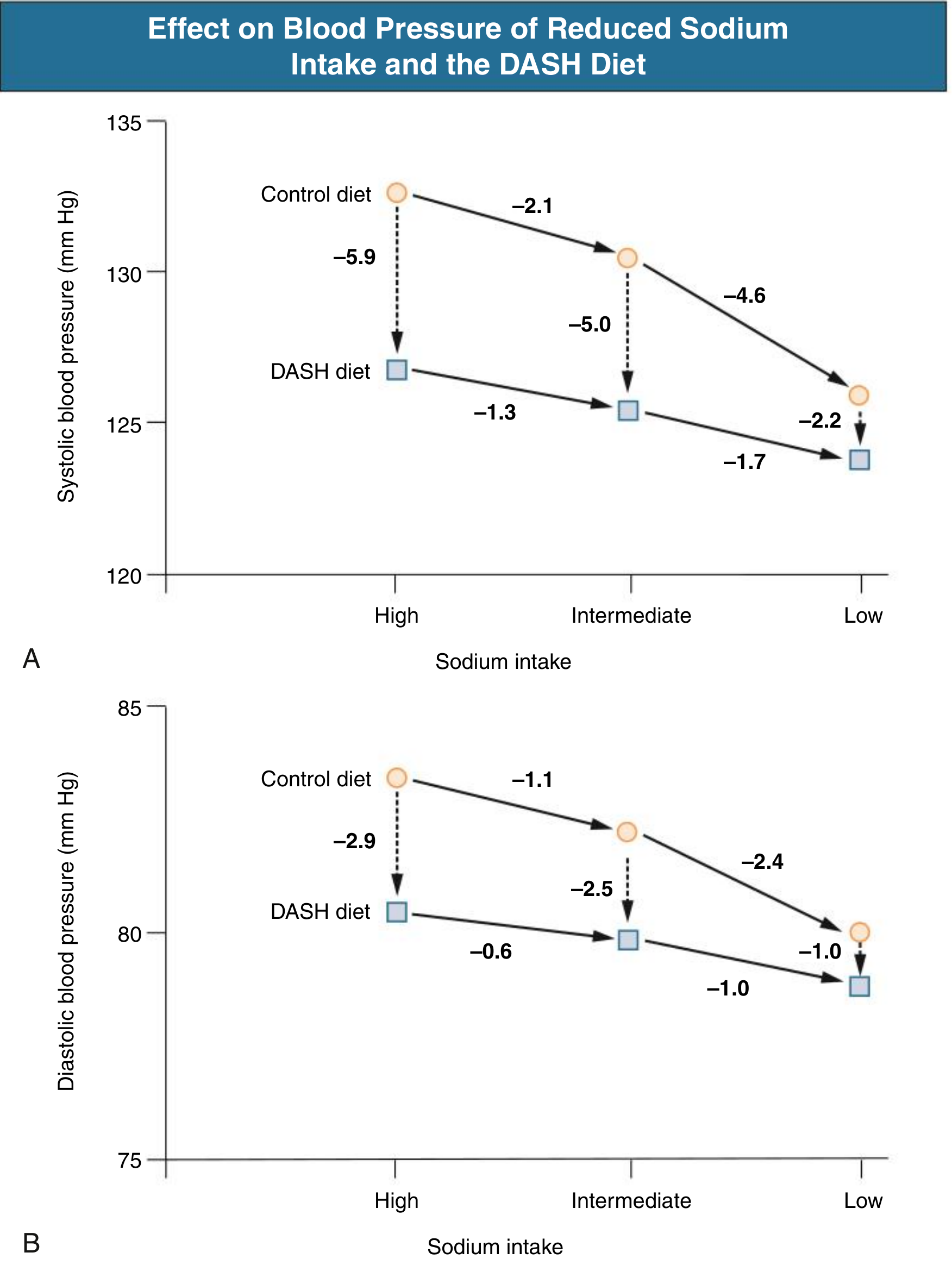
- Switching from Control diet → DASH diet at high sodium: SBP drops -5.9 mmHg
- DASH diet + Low sodium vs Control diet + High sodium: the greatest combined reduction
- The DASH diet is effective at all sodium levels, but combining with sodium restriction amplifies the benefit
The Role of Potassium
- In hypertensive patients on diuretics or with low K⁺ intake, potassium supplementation alone lowers BP by ~4-5 mmHg
- Adequate potassium intake goal: > 3,400 mg/day
- Low potassium stimulates intrarenal angiotensin II, oxidants, and endothelin - all of which raise BP
DASH Diet vs. Other Diets
- Mediterranean diet
- Vegetarian / vegan diets
- Low-carbohydrate diets
DASH Diet as Part of a Full Lifestyle Package
| Lifestyle Change | Expected SBP Reduction |
|---|---|
| DASH / healthy diet | -4 to -11 mmHg |
| Sodium restriction | -5 to -6 mmHg |
| Weight loss (1 kg = ~1 mmHg) | -5 mmHg |
| Potassium ↑ | -4 to -5 mmHg |
| Aerobic exercise (90-150 min/week) | -5 to -7 mmHg |
| Limit alcohol | -4 mmHg |
Combinations of these changes (e.g. DASH + sodium restriction + weight loss) can produce SBP reductions ≥ 10 mmHg - comparable to a single antihypertensive drug.
Special Populations
- Black/African American patients: Sodium reduction and potassium supplementation are especially effective in this group
- Patients on diuretics: Monitor potassium closely; DASH diet helps replenish K⁺
- Patients with CKD: High potassium foods in DASH may need modification if eGFR is low
- Elderly: DASH still effective; benefit is greatest at higher baseline BP
Bottom Line
The DASH diet is first-line, non-drug therapy for hypertension. It lowers BP, cholesterol, and blood glucose simultaneously. Combined with sodium restriction and other lifestyle changes, it can delay or even eliminate the need for medications in mild-moderate hypertension.
does formaiton of lactic acid means the cell start dead in spite of being on ventilarot with fio2 100
Does Lactic Acid Formation Mean Cells Are Dying Despite Ventilator + FiO₂ 100%?
Short Answer: No - not automatically. But it is a serious warning sign.
First - Understand How Lactic Acid Forms
Glucose → Pyruvate → (mitochondria) → Acetyl-CoA → Krebs cycle → ATP (energy)
Glucose → Pyruvate → (no oxygen) → LACTATE + H⁺
The Critical Concept: The Ventilator Fixes the Lungs - NOT Necessarily Oxygen Delivery to Cells
| Step | Process | Can Fail Despite Good Ventilation? |
|---|---|---|
| 1 | Lungs absorb O₂ into blood | ✅ Fixed by ventilator + FiO₂ 100% |
| 2 | Heart pumps oxygenated blood to tissues (DO₂) | ❌ Yes - if cardiac output is low |
| 3 | Cells extract and use O₂ (VO₂) | ❌ Yes - if mitochondria are poisoned or microcirculation is blocked |
Lactic acid rises when Step 2 or Step 3 fails - the ventilator only fixes Step 1.
Two Types of Lactic Acidosis (Clinically Important Classification)
Type A - Tissue Hypoxia (oxygen not reaching cells)
| Cause | Mechanism |
|---|---|
| Cardiogenic shock (low cardiac output) | Heart not pumping enough blood to tissues |
| Septic/distributive shock | Microvascular shunting - blood bypasses cells |
| Hypovolemic shock (hemorrhage) | Not enough blood volume to carry O₂ |
| Severe anemia | Not enough hemoglobin to carry O₂ |
| Carbon monoxide poisoning | CO binds hemoglobin, blocks O₂ transport |
| Bowel ischemia | Local tissue not getting perfusion |
| Pulmonary embolism | Low cardiac output + right heart strain |
Type B - No Tissue Hypoxia (oxygen available but cells cannot use it)
| Cause | Example |
|---|---|
| Medications | Metformin, antiretrovirals (HIV drugs) |
| Toxins | Cyanide poisoning, alcohol, methanol |
| Mitochondrial dysfunction | Sepsis-induced mitochondrial damage |
| Malignancy | Lymphoma, leukemia (Warburg effect) |
| Thiamine (Vitamin B1) deficiency | Blocks pyruvate entry into Krebs cycle |
| Liver failure | Cannot clear lactate |
| Seizures | Massive muscular O₂ demand |
So Why Can Cells Be Producing Lactate Even on FiO₂ 100%?
-
Septic shock - the heart may be pumping fine, lungs are oxygenated, but the bacteria/toxins cause:
- Microvascular shunting (blood flows past cells without entering capillaries)
- Mitochondrial dysfunction (cells cannot use oxygen even if it arrives)
- This is called cytopathic hypoxia - one of the reasons sepsis is so deadly
-
Low cardiac output - the ventilator saturates the blood, but a failing heart delivers too little oxygenated blood to meet demand
-
Severe anemia - high SaO₂ but low hemoglobin means low total oxygen content (DO₂ = CO × CaO₂)
-
Cyanide or CO poisoning - specifically blocks mitochondrial cytochrome c oxidase (Step 3 of the electron transport chain fails completely)
-
Liver failure - lactate is normally cleared by the liver; if the liver fails, lactate accumulates even without excess production
Does Elevated Lactate Mean Cells Are Dead?
| Lactate Level | Interpretation |
|---|---|
| < 2 mmol/L | Normal |
| 2-4 mmol/L | Hyperlactatemia - warning, increased mortality risk |
| > 4 mmol/L | Severe - high mortality, urgent treatment needed |
| Rising lactate despite treatment | Very poor prognosis - ongoing cellular distress |
| Falling lactate with treatment | Cells are recovering - good sign |
Cells producing lactate = cells are in distress and switching to emergency energy production. Cells that are truly dead stop producing lactate entirely (they stop doing anything). A high lactate means the cell is still fighting but failing.
What to Look For / Fix When a Ventilated Patient Has High Lactate
✅ Lungs OK (ventilator + FiO2 100%)
❓ Check cardiac output → echocardiogram, CVP
❓ Check hemoglobin → is it low? Transfuse if Hb < 7-8
❓ Check perfusion pressure → MAP > 65 mmHg?
❓ Check for sepsis → source? Cultures? Vasopressors?
❓ Check for bowel ischemia → lactate rising without clear cause?
❓ Check medications → metformin? any toxins?
❓ Check thiamine levels → especially in alcoholics / malnourished
❓ Check liver function → is lactate being cleared?
Key Take-Home Message
A ventilator with FiO₂ 100% makes the blood oxygen-rich. It does NOT guarantee that oxygen reaches or is used by the cells. Lactic acid is produced when cells run out of oxygen at the cellular level - which can happen even when lungs are working perfectly, if the heart, blood vessels, hemoglobin, or mitochondria are failing.
Rising lactate = cells are in trouble. It is a call to action to find and fix the underlying cause - not a declaration that the patient is unsalvageable.
a patient with cabg pod1 having less glucose bsl with fio2 100 and lactric acid incease
Post-CABG Day 1: Low BSL + Rising Lactate + FiO₂ 100% - What's Happening?
This is a Medical Emergency - Act Immediately
Reading the Clinical Picture
| Finding | What It Tells You |
|---|---|
| Post-CABG Day 1 | Heart has just been operated on - at risk for pump failure |
| FiO₂ 100% | Lungs being maximally supported - oxygenation is not the primary problem |
| Low Blood Sugar (Hypoglycemia) | Cells are consuming glucose faster than it's being supplied - anaerobic glycolysis is burning through glucose at massive rates |
| Rising Lactate | Cells are not getting/using oxygen - anaerobic metabolism is occurring |
Why Is Glucose LOW While Lactate Is HIGH?
Under anaerobic conditions (no oxygen), cells desperately try to make energy by burning glucose:
Glucose → Pyruvate → LACTATE
(no oxygen, no Krebs cycle)
- Aerobic metabolism: 1 glucose → 36-38 ATP (efficient)
- Anaerobic metabolism: 1 glucose → only 2 ATP (very inefficient)
- Glucose is consumed at a dramatically accelerated rate → blood sugar falls
- Lactate builds up as the byproduct of this emergency fuel burning
- Even with FiO₂ 100%, the oxygen is not reaching or being used by the cells
Low glucose + high lactate together = cells burning glucose rapidly without oxygen = severe tissue hypoperfusion
Most Likely Cause in This Specific Patient
⚠️ LOW CARDIAC OUTPUT SYNDROME (LCOS) Post-CABG
| Cause | Mechanism |
|---|---|
| Myocardial stunning | Heart temporarily paralyzed after bypass, not pumping effectively |
| Early graft failure / occlusion | New bypass graft clots → fresh MI → pump failure |
| Perioperative myocardial infarction | Watershed ischemia during or after surgery |
| Cardiac tamponade | Blood collecting in pericardium, compressing the heart |
| Arrhythmia (AF, VT) | Loss of coordinated pumping → low output |
| Vasodilatory shock | SIRS from bypass circuit → low SVR |
| Hypovolemia | Post-op bleeding → inadequate preload |
Other Causes to Consider (Do Not Miss)
| Cause | Clue |
|---|---|
| Insulin overdose | Was insulin infusion running? Post-cardiac surgery hyperglycemia is often treated with insulin drips - this is a common iatrogenic cause |
| Liver hypoperfusion | Liver makes glucose (gluconeogenesis); if liver not perfused → glucose production stops + lactate not cleared |
| Sepsis | Post-op infection, sternotomy wound, line infection - septic shock causes both |
| Adrenal insufficiency | Rare but causes refractory hypoglycemia + shock |
| Cyanide toxicity | If sodium nitroprusside was used for BP control post-op → can accumulate → blocks mitochondria |
Immediate Management Steps
🔴 URGENT - Do These First:
- D50W IV bolus (25-50 mL) - correct glucose to 140-180 mg/dL (10-15 mmol/L)
- Check if insulin infusion is running - reduce or stop it
- Monitor BSL every 15-30 minutes
- Bedside echocardiogram (POCUS) urgently
- Check arterial line waveform / pulse pressure
- Check urine output (oliguria = low cardiac output)
- Check extremities: cold, mottled = peripheral shutdown
- Falling BP + rising CVP + muffled heart sounds = Beck's Triad
- Echo will show pericardial collection
- If tamponade → emergency re-exploration
- 12-lead ECG immediately
- ST changes → new MI / graft failure
- If low cardiac output confirmed:
- Inotropes: Dobutamine, milrinone (especially if low EF)
- Vasopressors: Norepinephrine if BP low
- Volume: Cautious fluid if hypovolemic
- IABP (Intra-aortic balloon pump) if cardiogenic shock
- ECMO if refractory - last resort
- Every 1-2 hours
- Target: lactate falling by >10-20% per hour with treatment
- Rising lactate despite treatment = very poor prognosis
- Drain output - if >200 mL/hr for 2 hours → surgical re-exploration
Why This Is So Dangerous - Summary Diagram
Post-CABG → Heart not pumping well (low CO)
↓
Less blood delivered to tissues
↓
Cells starved of oxygen
↓
Switch to anaerobic glycolysis
↓
┌───────────────────────────────────┐
│ Burns glucose RAPIDLY │ → LOW BLOOD SUGAR
│ Produces LACTATE as byproduct │ → HIGH LACTATE
└───────────────────────────────────┘
↓
Metabolic acidosis, organ failure
↓
DEATH if not corrected urgently
Key Point for ICU Management
Glucose falling + lactate rising in a post-CABG patient = the heart is not keeping up. Treat the glucose as an emergency, but the REAL problem is the pump. Every minute of inadequate cardiac output means more organs are running on anaerobic fuel, consuming glucose rapidly, and accumulating acid. This is a race against time.
The ventilator and FiO₂ 100% are keeping the blood saturated, but saturated blood sitting in a failing heart is not helping the tissues. It is the cardiac output - not the FiO₂ - that must be fixed.
doctor told like to give cpr shots
"CPR Shots" - What the Doctor Actually Means: Vasopressors & Inotropes
Important Clarification First
| Drug Type | Job |
|---|---|
| Inotropes | Make the heart pump stronger |
| Vasopressors | Squeeze the blood vessels to keep blood pressure up |
The Three Drugs Being Used
1. 💉 Adrenaline (Epinephrine)
| Dose | Effect |
|---|---|
| Low dose | Strengthens heartbeat (β1) + slightly dilates vessels (β2) |
| High dose | Squeezes vessels + increases heart rate and force |
- Used when the heart is very weak AND blood pressure is critically low
- Very powerful - used when other drugs are not enough
- ⚠️ Side effects: fast heart rate, arrhythmias, raises lactate at high doses
2. 💉 Dopamine
| Dose | Effect |
|---|---|
| Low dose (2-5 mcg/kg/min) | Dilates kidney/gut vessels (splanchnic), helps urine output |
| Medium dose (5-10 mcg/kg/min) | Strengthens heart (inotrope) + increases heart rate |
| High dose (>10-15 mcg/kg/min) | Squeezes vessels (vasopressor effect) |
- Helps both heart pumping AND blood pressure
- Can protect kidneys at low doses
- ⚠️ Side effects: arrhythmias (more than other drugs) - especially problematic in post-cardiac surgery patients
3. 💉 Noradrenaline (Norepinephrine / "Norad")
| Effect | Explanation |
|---|---|
| Squeezes blood vessels (↑ SVR) | Raises blood pressure |
| Mild heart strengthening | Slight inotropic effect |
| Redistributes blood | Pushes blood to vital organs |
- First-choice vasopressor - raises blood pressure by tightening blood vessels
- Used when blood pressure is dangerously low despite the heart trying to pump
- ⚠️ At very high doses, too much vasoconstriction can reduce blood flow to gut and limbs
Why All Three Together?
Low Blood Pressure ←→ Noradrenaline (squeeze vessels UP)
←→ Dopamine (squeeze + pump harder)
Weak Heart ←→ Adrenaline (pump STRONGER, FASTER)
←→ Dopamine (medium dose inotrope)
Low Kidney Perfusion ←→ Dopamine low dose (kidney protection)
Simple Analogy
- The heart = the pump (inotropes make the pump stronger)
- The blood vessels = the hose (vasopressors squeeze the hose so pressure builds up)
- The organs = the plants (they need the water/oxygen delivered under good pressure)
What the Doctor Is Watching For
| Target | Normal Goal in ICU |
|---|---|
| MAP (Mean Arterial Pressure) | ≥ 65 mmHg |
| Urine Output | > 0.5 mL/kg/hour |
| Lactate | Falling with treatment |
| Blood Sugar | 140-180 mg/dL |
| Heart Rate | 60-100 bpm (not too fast) |
Is This Situation Dangerous?
- A known complication of cardiac surgery (called Low Cardiac Output Syndrome)
- Treatable in many cases with the drugs listed
- Monitored closely - the team is adjusting doses based on BP, lactate, urine output every few minutes
- If drugs are not enough: IABP (balloon pump) or even ECMO (heart-lung machine) can be used
Summary
| Drug | Primary Role | Main Effect |
|---|---|---|
| Adrenaline | Emergency heart support | Stronger + faster heartbeat |
| Dopamine | Heart + pressure + kidneys | Inotrope at medium dose, vasopressor at high dose |
| Noradrenaline | Blood pressure support | Squeezes blood vessels, raises BP |
These are life-supporting infusions running continuously through the IV. They are buying time for the heart to recover after the stress of CABG surgery. They are not "CPR shots" - they are the ICU team doing everything possible to keep the organs perfused while the heart heals.
tell abi ankel brachial index
Ankle-Brachial Index (ABI)
What Is It?
The Formula
- Ankle systolic BP = 100 mmHg
- Brachial systolic BP = 120 mmHg
- ABI = 100 ÷ 120 = 0.83 → Abnormal (PAD present)
How to Measure ABI (Step-by-Step)
- Patient lies supine for 5-10 minutes (resting)
- Apply blood pressure cuff just above the ankle
- Use a hand-held Doppler probe over the dorsalis pedis and posterior tibial arteries
- Inflate cuff, then deflate slowly - record pressure when Doppler signal returns
- Repeat for the other ankle
- Measure both brachial artery pressures with the Doppler
- Use the highest ankle pressure ÷ highest brachial pressure for each leg
ABI Values and Interpretation
| ABI Value | Clinical Meaning |
|---|---|
| > 1.4 | ⚠️ Abnormal - calcified, stiff arteries (false elevation - common in diabetes, renal failure) |
| 1.0 - 1.4 | ✅ Normal |
| 0.9 - 0.99 | ⚠️ Borderline - watch closely |
| < 0.9 | ❌ PAD present (confirmed) |
| ~0.6 | 🦵 Intermittent claudication (leg pain on walking) |
| ~0.3 | 😣 Ischemic rest pain (pain even at rest) |
| ~0.1 | ☠️ Impending tissue necrosis / gangrene |
Why Is the Ankle Pressure Normally Higher Than the Arm?
Symptoms of PAD (What ABI Detects)
| Stage | Symptoms |
|---|---|
| Asymptomatic | No symptoms but narrowed arteries (most patients!) |
| Claudication | Leg pain/cramping when walking - relieved by resting 2-5 min |
| Rest pain | Burning/aching in foot at rest, especially at night |
| Chronic Limb-Threatening Ischemia (CLTI) | Non-healing ulcers, gangrene - limb at risk of amputation |
| Acute Limb Ischemia | Sudden blockage - 6 P's: Pain, Pallor, Pulselessness, Paresthesia, Paralysis, Poikilothermia |
Important Limitations of ABI
| Limitation | Why It Happens |
|---|---|
| Falsely HIGH ABI (>1.4) | Calcified arteries in diabetes/CKD cannot be compressed by cuff |
| Misses single vessel disease | If one tibial artery blocks but others are open, ABI may not change |
| Bilateral subclavian disease | Both brachial pressures low → falsely elevated ABI |
ABI + Exercise Testing
- ABI is measured before and after treadmill exercise
- In PAD: ankle pressure drops after exercise (>20% fall = positive)
- This unmasks significant stenosis that is not apparent at rest
Risk Factors for PAD (and Why ABI Screening Matters)
| Risk Factor | Comment |
|---|---|
| Smoking | Strongest risk factor - PAD diagnosed a decade earlier in smokers |
| Diabetes | More severe disease, higher amputation risk |
| Age > 65 | Prevalence 14-23% |
| Hypertension | Accelerates atherosclerosis |
| CKD | Also causes vessel calcification → falsely high ABI |
| Previous MI/stroke | PAD patients have 3x higher risk of heart attack and stroke |
PAD is not just a leg problem. Patients with ABI < 0.9 have a markedly increased risk of MI, stroke, and cardiovascular death - because the same atherosclerosis affects coronary and carotid arteries.
Treatment Overview Based on ABI
| Finding | Management |
|---|---|
| ABI 0.9-1.4 (normal/borderline) | Modify risk factors, lifestyle changes |
| ABI < 0.9 (PAD confirmed) | Statin, antiplatelet (aspirin/clopidogrel), BP control, smoking cessation, exercise program |
| Claudication symptoms | Add cilostazol, supervised exercise program |
| Rest pain / CLTI | Revascularization (angioplasty/stenting/bypass), wound care |
| Acute limb ischemia | Emergency revascularization + anticoagulation |
Quick Summary
ABI = Ankle BP ÷ Arm BP
Normal: 1.0 - 1.4
< 0.9 = PAD confirmed
< 0.5 = Severe ischemia
> 1.4 = Falsely elevated (calcified vessels)
What other tests diagnose peripheral artery disease (duplex ultrasound, CTA, MRA)?
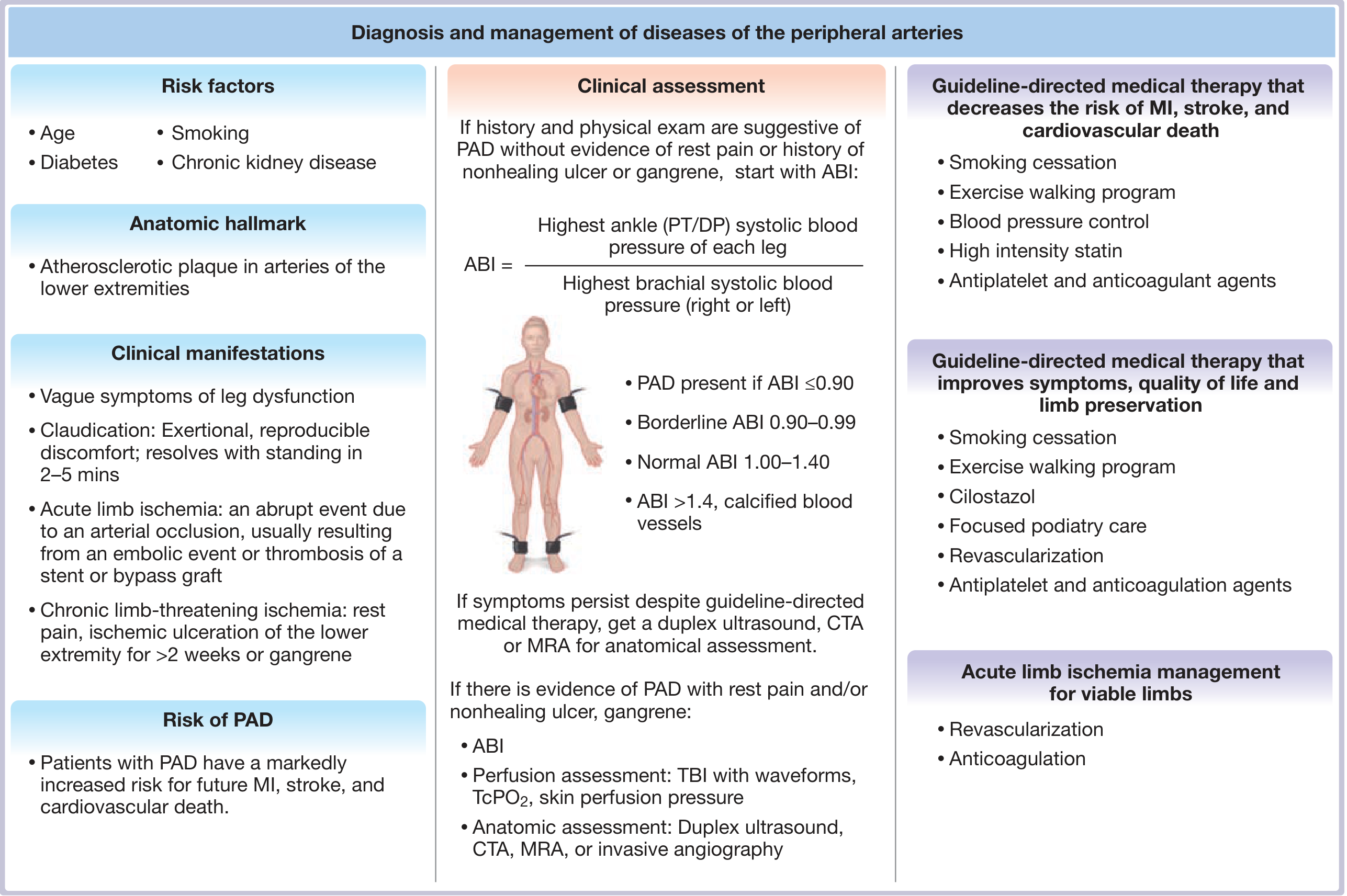
Imaging Tests for Peripheral Artery Disease (PAD)
The Diagnostic Pathway
1. Duplex Ultrasound
What It Is
How It Works
- The probe sends sound waves that bounce off moving red blood cells
- High velocity jet = narrowed (stenotic) segment
- Peak Systolic Velocity (PSV) ratio > 2.0 between stenosis and normal segment = ≥ 50% stenosis
- Aliasing (colour wrap-around) and turbulent flow on the waveform = severe stenosis
Advantages ✅
- No radiation, no contrast - completely safe
- Portable - can be done at bedside
- Real-time - shows anatomy AND blood flow simultaneously
- Cheap and widely available
- Excellent for monitoring bypass graft surveillance
Limitations ❌
- Operator-dependent - quality depends on sonographer skill
- Bowel gas and obesity interfere with imaging of aorto-iliac segments
- Difficult with multi-level disease (hard to trace long segments)
- Heavily calcified vessels scatter ultrasound
- Time-consuming for whole-leg survey
Sensitivity / Specificity
- Sensitivity: 85-90% | Specificity: >95%
2. Computed Tomography Angiography (CTA)
What It Is

How It Works
- Contrast fills the arterial lumen
- Computer reconstructs 3D images that can be rotated and viewed in any plane
- Stenoses appear as narrowing or filling defects
- Can measure exact lesion length - critical for planning angioplasty/stenting
Advantages ✅
- Superior resolution compared to MRA
- Fast - whole-leg imaging in minutes
- 3D reconstruction - shows exact anatomy for intervention planning
- Helps determine best access site for catheter procedures
- Shows vessel calcification clearly (important for surgical planning)
Limitations ❌
- Iodinated contrast - risk of contrast nephropathy (avoid if eGFR < 30)
- Ionizing radiation (X-ray dose)
- Heavy calcification can obscure the lumen (same problem as ABI)
- Allergic reactions to contrast (rare but serious)
Sensitivity / Specificity
- Sensitivity: 90-95% | Specificity: >90%
3. Magnetic Resonance Angiography (MRA)
What It Is
How It Works
- Gadolinium shortens relaxation time of blood, making vessels bright
- Multi-station technique images from aorta to feet
- Can also be done without contrast (Time-of-flight MRA) - less optimal quality
Advantages ✅
- No ionizing radiation
- No iodinated contrast - safer in patients with mild-moderate CKD (use gadolinium instead)
- Excellent sensitivity and specificity - highest of all non-invasive tests
- Good for patients with iodine allergy
- 3D images similar to CTA
Limitations ❌
- Gadolinium + eGFR < 30 → risk of Nephrogenic Systemic Fibrosis (NSF) - serious fibrotic condition (avoid)
- Implanted devices (pacemakers, stents, clips) may be incompatible - need screening
- In-stent restenosis poorly assessed (metal causes artifact)
- Longer scan time than CTA
- Claustrophobia can prevent scanning
- Overestimates stenosis severity (compared to CTA)
Sensitivity / Specificity
- Sensitivity: 93-100% | Specificity: 93-100% (highest of all)
4. Catheter-Based Angiography (Digital Subtraction Angiography - DSA)
What It Is
How It Works
- Iodinated contrast injected directly into the aorta or target vessel
- Digital subtraction removes bone/soft tissue background - only vessels visible
- Can image from aorta → iliac → femoral → popliteal → tibial → foot arteries
- Intervention can be performed in the same session (angioplasty + stenting)
Advantages ✅
- Gold standard - best spatial resolution of all tests
- Diagnostic + therapeutic in the same procedure
- Can measure pressure gradients across stenoses (functional significance)
- Best assessment of tibial/foot vessels (critical for limb salvage planning)
Limitations ❌
- Invasive - arterial puncture required
- Iodinated contrast - nephropathy risk
- Ionizing radiation
- Access site complications - haematoma, pseudoaneurysm, arterial injury
- Distal embolization (rare)
- 2D imaging only - may underestimate stenosis
- Not used for diagnosis alone any more - reserved for planned intervention
Sensitivity / Specificity
- Traditional gold standard (reference test against which others are compared)
Quick Comparison Table (from Fuster & Hurst's The Heart)
| Test | Sensitivity | Specificity | Key Limitation | Best Used For |
|---|---|---|---|---|
| Duplex US | 85-90% | >95% | Operator-dependent, calcified vessels | First-line anatomic test, graft surveillance |
| MRA | 93-100% | 93-100% | Gadolinium + CKD → NSF; implants | Best non-invasive option, iodine allergy |
| CTA | 90-95% | >90% | Iodinated contrast, radiation, calcification | Pre-intervention planning, best resolution |
| Catheter DSA | Gold standard | Gold standard | Invasive, contrast, radiation | When intervention planned in same session |
Additional Perfusion Tests (Beyond Anatomy)
| Test | What It Measures | When Used |
|---|---|---|
| Toe-Brachial Index (TBI) | Digital artery pressure | Calcified tibial vessels (diabetes/CKD) - TBI < 0.7 = PAD |
| TcPO₂ (transcutaneous oxygen) | Skin oxygen tension | Wound healing potential - TcPO₂ < 30 mmHg = poor healing |
| Skin Perfusion Pressure | Microvascular pressure | Critical limb ischemia assessment |
| Pulse Volume Recording (PVR) | Volume waveforms at each level | Complements segmental pressures |
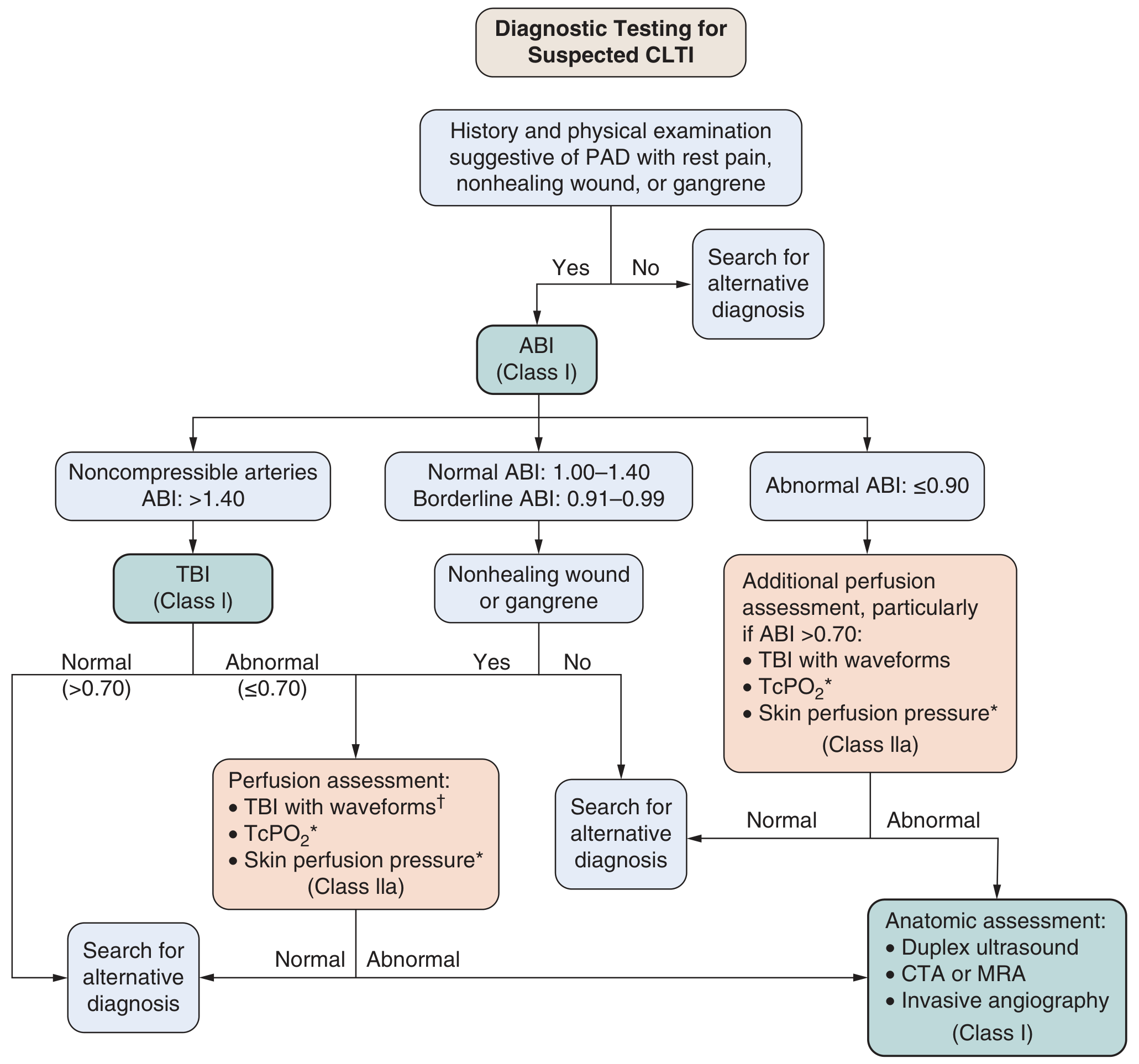
When to Use Each Test - Clinical Decision Guide
Suspected PAD → Start with ABI
ABI < 0.9 confirmed PAD
→ Medical treatment only? → No imaging needed
→ Revascularization being considered?
→ Duplex US first (no radiation/contrast)
→ Then CTA (if intervention planning needed, best resolution)
→ Or MRA (if CKD + iodine allergy)
→ Catheter DSA only when intervention will be done same day
ABI > 1.4 (non-compressible)
→ TBI instead
→ TcPO₂ for wound healing assessment
abi more than 1.40 asymptomatic means
ABI > 1.4 in an Asymptomatic Patient - What Does It Mean?
The Most Important Point First
ABI > 1.4 does NOT mean the patient is healthy or has normal arteries. It means the arteries are so rigid and calcified that a blood pressure cuff cannot compress them - giving a falsely high (suprasystolic) reading. This is called non-compressible arteries, and it is an abnormal result - even with zero symptoms.
Why Does ABI Go Above 1.4?
Normal Artery vs. Calcified Artery
Cuff inflated → artery compressed → blood flow stops → pressure recorded
→ ABI calculated accurately
Cuff inflated → artery CANNOT be compressed (rigid like a pipe)
→ Doppler signal never disappears
→ Cuff keeps inflating to very high pressures
→ Ankle "pressure" recorded is falsely very high
→ ABI > 1.4 (or even 2.0+)
Who Gets This? (Risk Factors for Non-Compressible Arteries)
| Condition | Why |
|---|---|
| Diabetes mellitus | Most common cause - autonomic neuropathy drives medial calcification |
| Chronic kidney disease (CKD) / Renal failure | Abnormal calcium-phosphate metabolism → calcium deposits in vessel walls |
| Advanced age (elderly) | Progressive medial calcification with aging |
| Long-standing hypertension | Accelerates arterial stiffening |
| Bilateral subclavian/axillary artery disease | Both brachial pressures falsely low → ratio falsely high |
Is Being Asymptomatic Reassuring?
1. The Arteries Are Severely Diseased
2. High Risk of Cardiovascular Death
3. PAD May Be Hidden
4. Symptoms May Be Absent Due to Neuropathy
What To Do When ABI > 1.4
First-Line Alternative: Toe-Brachial Index (TBI)
- Measures digital artery pressure at the big toe using a small cuff and photoplethysmography (PPG)
- Toe arteries are resistant to calcification (unlike tibial arteries)
- TBI < 0.7 = PAD confirmed
- TBI < 0.4 = severe ischemia / critical limb-threatening ischemia
Other Tests:
| Test | What It Assesses |
|---|---|
| Doppler waveform analysis | Shape of waveform - dampened/monophasic = stenosis |
| Pulse Volume Recording (PVR) | Volume changes in limb per heartbeat |
| TcPO₂ (transcutaneous oxygen) | Skin oxygen tension - TcPO₂ < 30 mmHg = poor tissue perfusion |
| Duplex ultrasound | Direct visualization of arterial lumen and flow velocity |
| MRA / CTA | Anatomic imaging if revascularization is planned |
Summary in Simple Terms
| ABI Value | What It Means |
|---|---|
| 1.0 - 1.4 | ✅ Normal |
| 0.9 - 0.99 | ⚠️ Borderline PAD |
| < 0.9 | ❌ PAD confirmed |
| > 1.4 | ⚠️ ABNORMAL - calcified/stiff arteries - ABI is unreliable |
Think of ABI > 1.4 like a thermometer stuck at maximum - it is not giving you a true reading. The pipe is too hard to squeeze. You need a different test (TBI) to find out what is really happening inside.
Even if the patient has NO leg symptoms, ABI > 1.4 demands:
- Risk factor control (diabetes, BP, cholesterol, smoking)
- Statin therapy
- TBI measurement
- Cardiovascular risk assessment (ECG, lipids, renal function)
- Close follow-up - symptoms may develop later once neuropathy or lumen narrowing progresses
sle symptomatic lupus erathymatous
Systemic Lupus Erythematosus (SLE)
What Is SLE?
- Relapsing-remitting course (flares and remissions)
- Highly variable - from mild skin/joint disease to life-threatening kidney or brain involvement
- Predominantly affects women of childbearing age (9:1 female to male ratio)
- Higher incidence in African, Asian, and Hispanic populations
The Classic Sign - Malar (Butterfly) Rash

Clinical Manifestations - Frequency Table
| Manifestation | Frequency |
|---|---|
| Cutaneous (skin) | 88% |
| Arthritis / arthralgias | 76% |
| Neuropsychiatric | 66% |
| Pleurisy / pericarditis | 63% |
| Anemia | 57% |
| Raynaud phenomenon | 44% |
| Vasculitis | 43% |
| Atherosclerosis | 37% |
| Nephritis (kidney) | 31% |
| Thrombocytopenia | 30% |
| Sensorimotor neuropathy | 28% |
| Cardiac valvular disease | 18% |
| Pulmonary alveolar hemorrhage | 12% |
| Pancreatitis | 10% |
| Myositis / Myocarditis | 5% |
System-by-System Symptoms
1. 🌡️ Constitutional (General)
- Fatigue (most common complaint - can be debilitating)
- Fever (often low-grade, especially during flares)
- Weight loss
- Anorexia, malaise, myalgia
2. 🩺 Skin (88%)
| Lesion | Description |
|---|---|
| Malar (butterfly) rash | Fixed red rash across cheeks + nose, sparing nasolabial folds |
| Discoid rash | Red plaques with thick scales, can scar - seen on scalp, face, ears |
| Photosensitivity | Rash or flare triggered by sun exposure (UV light) |
| Oral ulcers | Painless ulcers on palate or inside mouth |
| Alopecia | Diffuse hair loss (non-scarring) |
| Raynaud phenomenon | Fingers turn white → blue → red with cold/stress (44% of patients) |
3. 🦴 Musculoskeletal (76%)
- Arthritis - most commonly affects small joints of hands, wrists, knees
- Arthralgias (joint pain without swelling)
- Typically non-erosive (unlike rheumatoid arthritis - joints are not destroyed)
- Myositis (muscle inflammation) in 5%
- Jaccoud arthropathy - reducible deformities from ligament laxity (not bone erosion)
4. 🫘 Kidney - Lupus Nephritis (31%)
- Caused by immune complex deposition in glomeruli
- Presents with: proteinuria, haematuria, hypertension, oedema, rising creatinine
- Can progress to end-stage kidney disease if untreated
- Classified into ISN/RPS Class I-VI on kidney biopsy
- Class III and IV (proliferative nephritis) are the most severe
5. 🧠 Neuropsychiatric (66%)
- Cognitive dysfunction (brain fog, memory problems) - most common (17-66%)
- Headaches
- Seizures (6-51%)
- Psychosis or mood disorder (up to 8%)
- Cerebrovascular disease / stroke (5-18%)
- Peripheral neuropathy - asymmetrical, sensorimotor (28%)
- Rare but devastating: Transverse myelopathy → paraplegia
- Ocular: cotton-wool spots on retina from retinal ischemia
6. ❤️ Cardiovascular
- Pericarditis - chest pain, friction rub, effusion (most common cardiac feature)
- Libman-Sacks endocarditis - sterile vegetations on heart valves (associated with antiphospholipid antibodies)
- Myocarditis (5%) - heart failure, arrhythmia
- Premature atherosclerosis - major long-term risk; SLE accelerates coronary artery disease independent of other risk factors
7. 🫁 Pulmonary (63%)
- Pleuritis - most common lung manifestation; chest pain on breathing, exudative pleural effusion
- Alveolar haemorrhage (12%) - coughing blood, rapidly falling haemoglobin
- Pulmonary hypertension - shortness of breath, right heart failure
- Pulmonary embolism - especially with antiphospholipid antibodies
8. 🩸 Blood (Haematological)
- Anaemia (57%) - autoimmune haemolytic anaemia (positive Coombs test) or anaemia of chronic disease
- Leukopenia / lymphopenia - low white cells
- Thrombocytopenia (30%) - low platelets → bleeding risk
9. Antiphospholipid Syndrome (33%)
- Arterial and venous thrombosis (DVT, PE, stroke)
- Recurrent pregnancy loss
- Livedo reticularis (net-like skin pattern)
- Catastrophic antiphospholipid syndrome - multi-organ thrombosis, fatal in 30%
Diagnosis - ACR Criteria (Need 4 of 11)
| # | Criterion |
|---|---|
| 1 | Malar rash |
| 2 | Discoid rash |
| 3 | Photosensitivity |
| 4 | Oral ulcers |
| 5 | Arthritis (non-erosive, ≥2 joints) |
| 6 | Serositis (pleuritis or pericarditis) |
| 7 | Renal disorder (proteinuria >0.5g/day or cellular casts) |
| 8 | Neurologic disorder (seizures or psychosis) |
| 9 | Haematologic disorder (haemolytic anaemia, leukopenia, thrombocytopenia) |
| 10 | Positive ANA |
| 11 | Immunologic: anti-dsDNA, anti-Smith, antiphospholipid antibodies |
Key Antibodies in SLE
| Antibody | Sensitivity | Specificity | Clinical Use |
|---|---|---|---|
| ANA | >99% | Low | Best screening test (positive in nearly all SLE) |
| Anti-dsDNA | 70% | High | Most specific for SLE; tracks disease activity |
| Anti-Smith (anti-Sm) | 25-30% | Very high | Highly specific for SLE |
| Anti-Ro (SSA) | Moderate | Moderate | Neonatal lupus, skin disease |
| Antiphospholipid | 33% | - | Thrombosis, pregnancy loss |
| Low C3/C4 complement | - | - | Active nephritis indicator |
ESR is elevated in SLE but CRP is often surprisingly LOW (unless there is infection or serositis) - this is a unique feature of SLE that helps distinguish lupus flare from infection.
Treatment Summary
| Disease Activity | Treatment |
|---|---|
| Mild (skin, joints) | NSAIDs + Hydroxychloroquine (backbone of all SLE treatment) |
| Moderate | Add low-dose corticosteroids |
| Severe (nephritis, CNS, haematologic) | High-dose corticosteroids + Mycophenolate mofetil or Cyclophosphamide |
| Maintenance | Azathioprine or Mycophenolate |
| Refractory / Biologics | Belimumab (anti-BLyS) or Rituximab |
| Antiphospholipid syndrome | Long-term anticoagulation (warfarin) |
Hydroxychloroquine is given to virtually ALL SLE patients - it reduces flares, prevents organ damage, reduces clots, and improves survival.
Drug-Induced Lupus (Important to Know)
SLE in Pregnancy
- Lupus flares during pregnancy are rare if disease was stable at conception
- Increased risk of: gestational hypertension, fetal growth restriction, preeclampsia, fetal loss
- Anti-Ro/La antibodies → neonatal lupus and congenital heart block in baby
- Hydroxychloroquine is safe in pregnancy and should be continued
lung maturity test during gravida
Fetal Lung Maturity Tests During Pregnancy
Why Do We Test Fetal Lung Maturity?
- Alveoli collapse with every expiration
- Infant struggles to breathe → Respiratory Distress Syndrome (RDS) / Hyaline Membrane Disease
- Can be fatal if not treated
When Do Fetal Lungs Mature?
| Stage | Gestational Age | Event |
|---|---|---|
| Lung buds form | 4-6 weeks | Airways begin branching |
| Canalicular phase | 16-26 weeks | Airways and capillaries develop |
| Saccular phase | 26-36 weeks | Air sacs (saccules) form |
| Surfactant production | ~24 weeks | Type II pneumocytes begin producing surfactant |
| Lung maturity | ~34-36 weeks | Adequate surfactant for independent breathing |
| Full maturity | ≥ 39 weeks | Optimal - all systems ready |
Surfactant is made by Type II alveolar pneumocytes. The main component is phosphatidylcholine (lecithin), which is the basis of all lung maturity tests.
The Tests - How Each One Works
1. 🔬 Lecithin/Sphingomyelin (L/S) Ratio - The Classic Test
- Lecithin (phosphatidylcholine) is the main surfactant phospholipid - rises sharply after 34-35 weeks
- Sphingomyelin stays relatively constant throughout pregnancy
- As lungs mature, L/S ratio increases
| L/S Ratio | Interpretation |
|---|---|
| < 1.5 | Immature - high risk of RDS |
| 1.5 - 1.9 | Transitional - moderate risk |
| ≥ 2.0 | Mature - low risk of RDS |
| ≥ 3.5 | Definitely mature |
- In diabetic mothers, L/S ratio ≥ 2.0 may still be associated with RDS
- Need L/S ≥ 3.5 or positive phosphatidylglycerol (PG) for reassurance in diabetic pregnancies
- This is because diabetes alters surfactant composition even when L/S appears adequate
2. 🧪 Phosphatidylglycerol (PG) Test
- PG is a minor but critical phospholipid component of surfactant
- Appears in amniotic fluid only after ~36 weeks - very late in lung maturation
- Its presence = lungs are fully mature and functioning
| PG Result | Interpretation |
|---|---|
| Absent | Immature |
| Present (≥ 2% of phospholipids) | Mature - very reliable indicator |
- Not affected by blood or meconium contamination (unlike L/S ratio)
- Can be tested on vaginal pool fluid after membrane rupture (no amniocentesis needed)
- Most reliable test for diabetic pregnancies
3. 🔢 Lamellar Body Count (LBC) - Simplest Modern Test
- Lamellar bodies are the storage form of surfactant inside Type II pneumocytes - tiny packets of phospholipid ready for release
- They are the same size as platelets → measured on a standard automated blood cell counter!
- More lamellar bodies in amniotic fluid = more mature lungs
| LBC Value | Interpretation |
|---|---|
| < 10,000/µL | Immature |
| 10,000-50,000/µL | Transitional (indeterminate) |
| > 50,000/µL | Mature |
- Quick, cheap, simple - uses a standard platelet counter
- No special equipment needed
- Results in minutes
- Good sensitivity and specificity
4. 📊 Surfactant/Albumin Ratio (TDx FLM II)
- Measures total surfactant relative to albumin in amniotic fluid using fluorescence polarization
- ≥ 55 mg surfactant/g albumin = mature
- Used as a rapid automated test
- Discontinued by the manufacturer in 2008 - no longer widely available
5. 🧴 Foam Stability (Shake) Test
- Surfactant stabilizes foam in the presence of alcohol
- Mix amniotic fluid with ethanol and shake → observe for persistent foam ring at meniscus after 15 minutes
| Result | Meaning |
|---|---|
| Positive (foam persists) | Mature lungs |
| Negative (no foam) | Immature |
6. 🫁 Lung Profile (Full Profile)
7. 📡 Quantitative Ultrasound (QuantusFLM) - Newest Technique
- Fetal lung texture on ultrasound at the four-chamber cardiac view is analyzed
- Images uploaded to cloud database → computer algorithm predicts lung maturity
- Validated in large prospective multicenter studies
- Results comparable to invasive tests
- Future direction - may replace amniocentesis for lung maturity testing
Comparison Table of All Tests
| Test | Sample | What It Measures | Mature Value | Advantage | Limitation |
|---|---|---|---|---|---|
| L/S Ratio | Amniocentesis | Lecithin vs Sphingomyelin | ≥ 2.0 (≥ 3.5 in DM) | Gold standard historically | Affected by blood/meconium, needs special lab |
| PG | Amnio or vaginal pool | Phosphatidylglycerol | Present | Not affected by contamination, works in DM | Appears late (36 wks), misses some mature lungs |
| LBC | Amniocentesis | Lamellar body packets | > 50,000/µL | Quick, cheap, uses platelet counter | Borderline zone (10-50k) |
| TDx FLM | Amniocentesis | Surfactant/albumin ratio | ≥ 55 mg/g | Rapid automated | Discontinued |
| Foam/Shake | Amniocentesis | Foam stability | Foam at 15 min | Bedside, no lab needed | High false negative rate |
| QuantusFLM | Ultrasound | Lung texture | Algorithm result | Non-invasive | New - not universally available |
The Most Important Intervention: Antenatal Corticosteroids
Regimen:
- Betamethasone (Celestone): 12 mg IM x 2 doses, 24 hours apart ← preferred
- Dexamethasone: 6 mg IM x 4 doses, 12 hours apart (equally effective)
When to Give:
| Indication | Gestational Age |
|---|---|
| High risk of preterm delivery within 7 days | 24-34 weeks (standard) |
| Late preterm threatened birth | 34-37 weeks |
| Elective caesarean without labour | ≥ 37 weeks (reduces TTN) |
What They Do:
- Stimulate Type II pneumocytes to produce surfactant faster
- Reduce risk of RDS by 40-60%
- Also reduce: intraventricular hemorrhage, necrotizing enterocolitis, neonatal death
- A single rescue course is given if > 7 days have passed since the first course and preterm birth is still threatened
⚠️ Current Guideline Change:
- Tests do not reliably predict safety of delivery
- Late preterm babies (34-37 weeks) still at risk for RDS, hypoglycaemia, jaundice even with "mature" results
- Decision to deliver should be based on clinical indication, not test results alone
Why "Mature" Tests Can Still Be Wrong
- Diabetic mothers - surfactant qualitatively abnormal → RDS still possible
- Late preterm infants (34-37 wks) - increased risk of RDS, hypoglycaemia, and jaundice regardless of lung maturity result
- Tests measure phospholipid quantity but not functional surfactant activity
- That is why ACOG recommends delivery should not be delayed or accelerated based on these tests alone
vasospastic means
reaynauds disease