Describe the at your pathogenesis and morphology feature of tuberculosis including type primary secondary progressive
Tuberculosis: Pathogenesis and Morphology
Overview
Pathogenesis
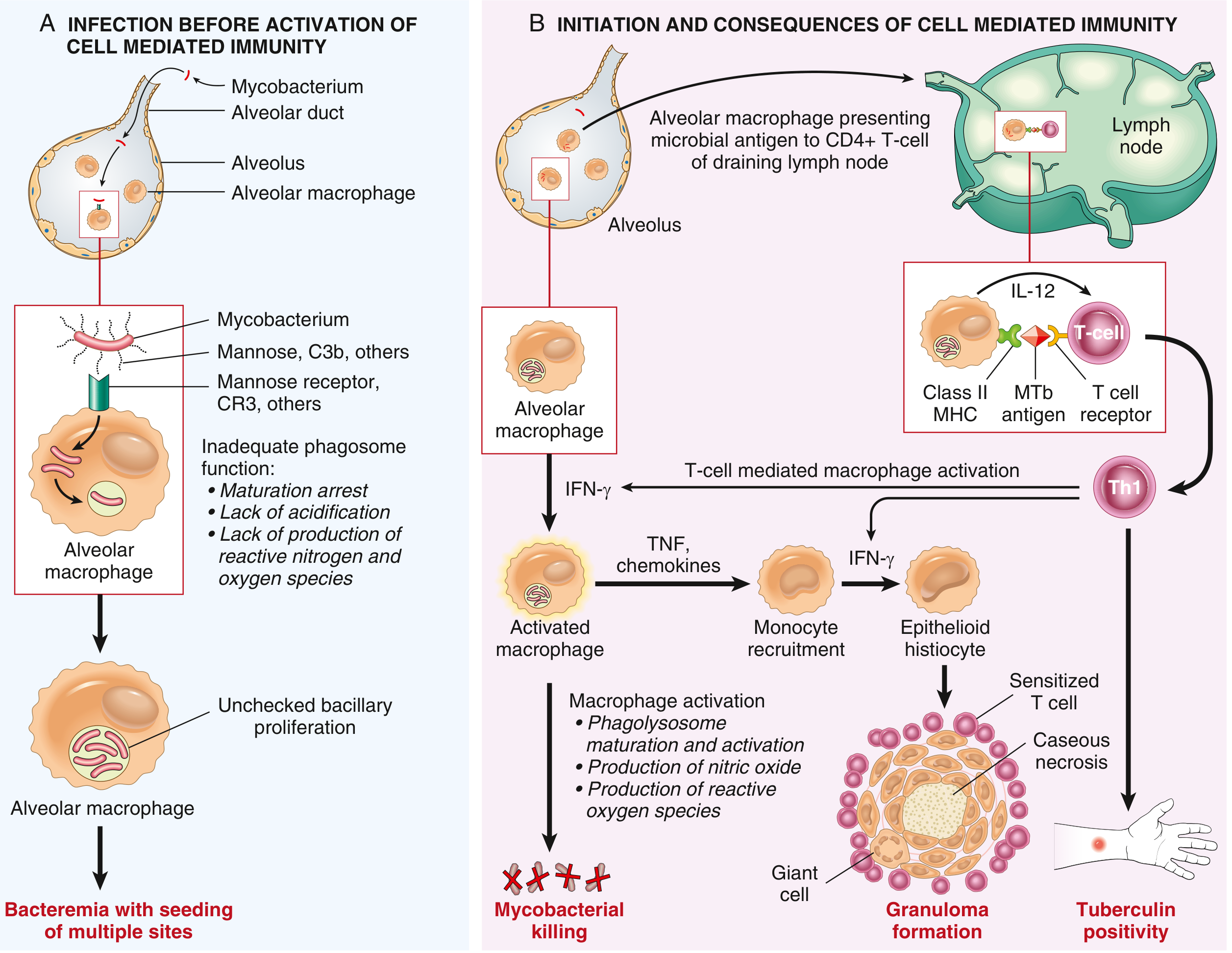
Step 1 - Entry into macrophages (First 3 weeks)
Step 2 - Unchecked early bacillary proliferation
Step 3 - Development of cell-mediated immunity (~3 weeks post-exposure)
Step 4 - T cell-mediated macrophage activation and killing
- TNF - recruits monocytes that differentiate into the macrophages forming granulomas
- Inducible nitric oxide synthase (iNOS) - produces NO and reactive nitrogen intermediates that kill mycobacteria
- Antimicrobial peptides (defensins) - directly toxic to the organisms
Step 5 - Granulomatous inflammation and tissue damage
| Molecule | Role |
|---|---|
| IL-12 | Drives Th1 differentiation |
| IFN-γ | Activates macrophages |
| TNF | Monocyte recruitment, granuloma maintenance |
| iNOS / NO | Mycobacterial killing |
| Defensins | Direct antimycobacterial toxicity |
Types of Tuberculosis and Their Morphology
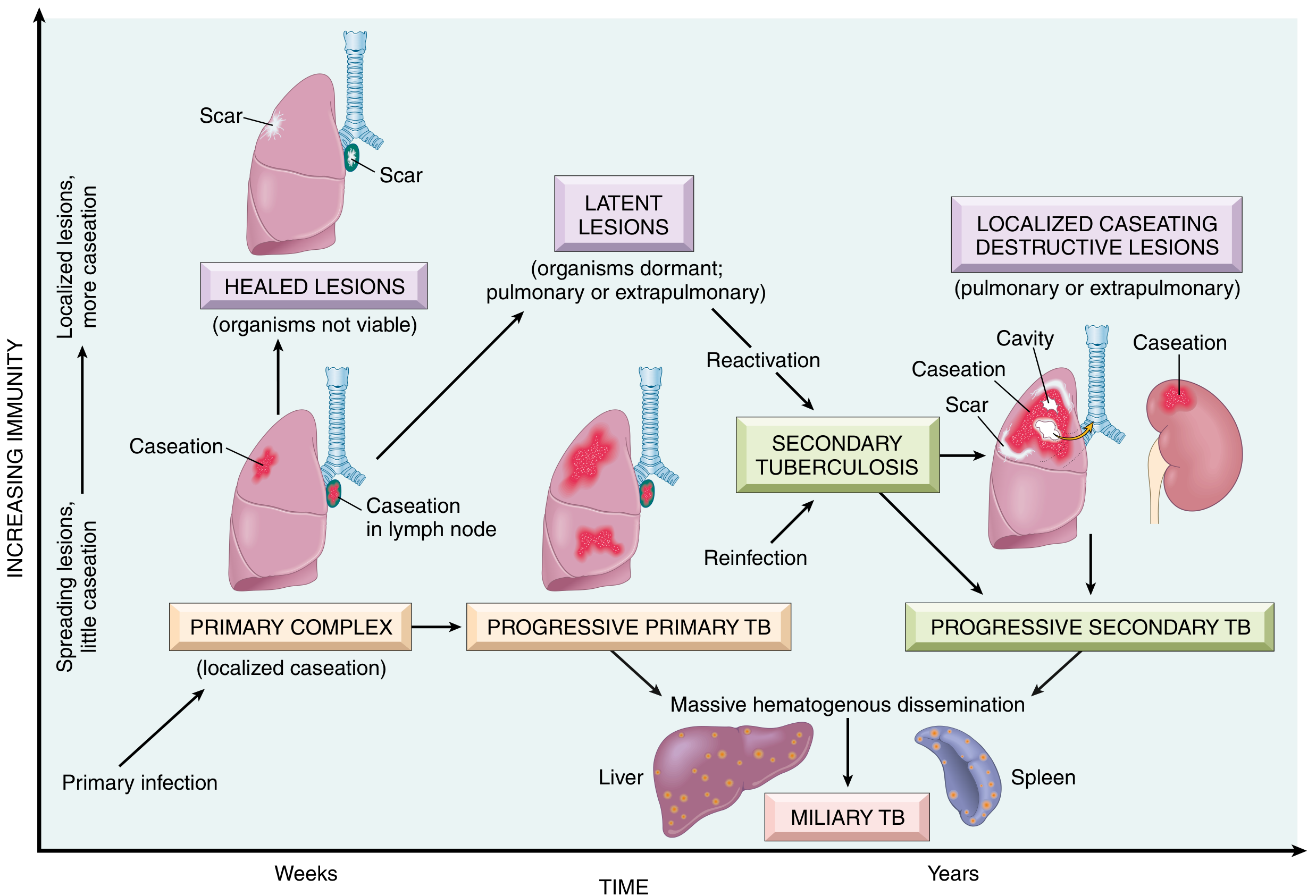
1. Primary Tuberculosis
- Inhaled bacilli implant in the distal air spaces of the lower part of the upper lobe or upper part of the lower lobe, typically near the pleura.
- A 1-1.5 cm gray-white consolidation appears called the Ghon focus. Its center undergoes caseous necrosis.
- Bacilli travel via lymphatics to the regional (hilar) lymph nodes, which also often caseate.
- The combination of the parenchymal Ghon focus + involved lymph nodes = Ghon complex (also called Ranke complex when calcified on x-ray).
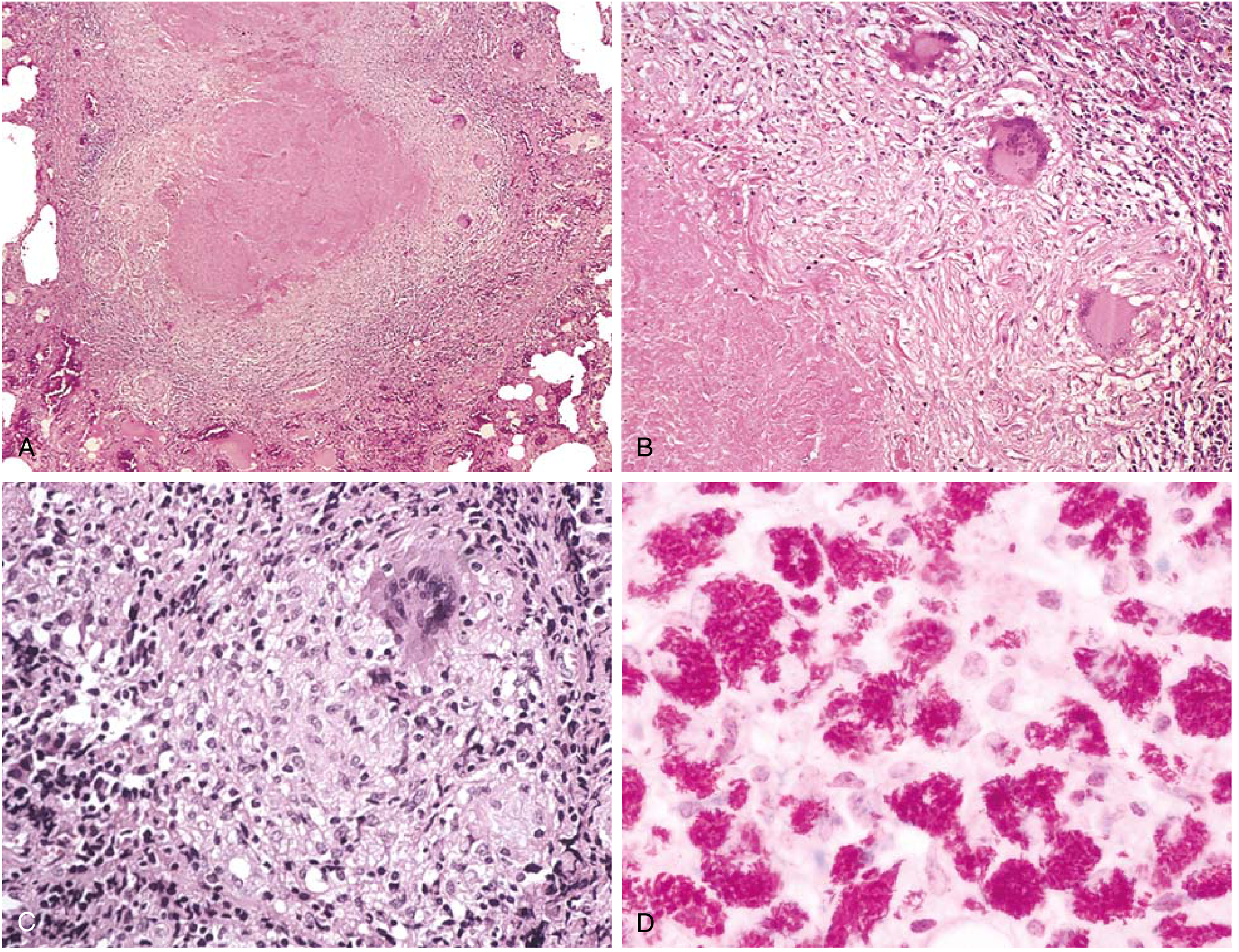
- Caseating and non-caseating granulomas with epithelioid macrophages and Langhans giant cells (multinucleate, peripheral nuclei)
- Central granular caseous (cheese-like) necrosis surrounded by a collar of epithelioid cells, lymphocytes, and giant cells
- In immunocompromised patients without effective CMI: granulomas are absent; instead, sheets of macrophages packed with numerous bacilli are seen (acid-fast stain positive)
2. Progressive Primary Tuberculosis
- The primary focus fails to be contained and continues to enlarge
- Granulomatous reaction is absent or poorly formed
- Hematogenous dissemination is extensive, potentially leading to miliary TB
- Histologically: sheets of macrophages with numerous bacilli instead of organized granulomas
- Clinically mimics a severe pneumonia; hilar lymphadenopathy is prominent
- Often presents with lower and middle lobe consolidation rather than apical disease
3. Secondary (Reactivation) Tuberculosis
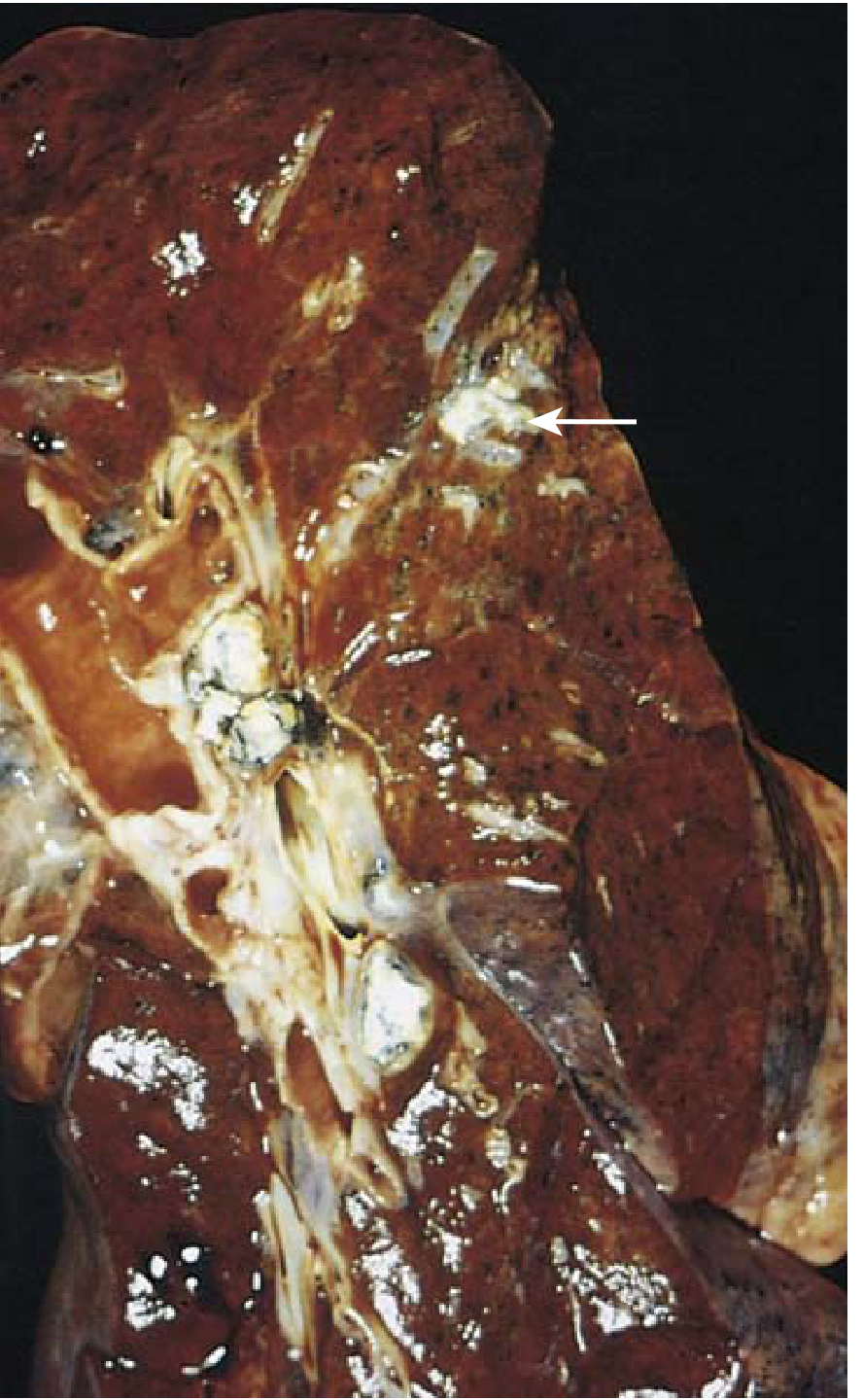
- Initial lesion: Small (<2 cm), firm, gray-to-yellow consolidation focus within 1-2 cm of the apical pleura, with variable central caseation and peripheral fibrosis
- Healing: Progressive fibrous encapsulation → fibrocalcific scars
- Active lesions: Characteristic coalescent caseating granulomatous nodules
- Bacilli are demonstrable in early exudative and caseous phases but cannot usually be found in fibrocalcific stages
- A ragged, irregular cavity is formed, lined by caseous material, poorly walled off by fibrous tissue
- Erosion of blood vessels → hemoptysis
- Cavities may remain open (source of ongoing infectivity via sputum) or collapse and become fibrotic
| Pathway | Result |
|---|---|
| Via airways (endobronchial spread) | Endobronchial/endotracheal/laryngeal TB; mucosal granulomas |
| Via lymphatics | Lymphadenitis (most frequent extrapulmonary form; cervical = "scrofula") |
| Via pulmonary arteries (hematogenous) | Miliary pulmonary disease: 2-mm yellow-white foci resembling millet seeds throughout the lung |
| Systemic hematogenous | Systemic miliary TB: liver, bone marrow, spleen, adrenals, meninges, kidneys, fallopian tubes, epididymis |
| Direct extension to pleura | Serous effusion, tuberculous empyema, fibrous pleuritis |
| Vertebral seeding | Pott disease (cold abscess may track to present as abdominal/pelvic mass) |
| Swallowed infected sputum | Intestinal TB (ileum most common; mucosal ulceration over lymphoid aggregates) |
- Mildly immunocompromised (CD4+ >300): typical apical cavitary disease
- Severely immunocompromised (CD4+ <200): mimics progressive primary TB (lower lobe consolidation, hilar lymphadenopathy, no cavities)
- Extrapulmonary involvement rises from 10-15% (mild immunosuppression) to >50% (severe immunodeficiency)
Summary Table
| Feature | Primary TB | Progressive Primary TB | Secondary (Reactivation) TB |
|---|---|---|---|
| Host | Naive, previously unexposed | Immunocompromised, HIV with CD4 <200 | Previously sensitized host |
| Location | Lower upper lobe / upper lower lobe, subpleural | Diffuse / lower lobes | Apices of upper lobes |
| Gross lesion | Ghon focus + hilar lymph node caseation (Ghon complex) | No clear walling off; extensive consolidation | Small apical focus → cavity formation |
| Histology | Caseating granulomas + epithelioid cells + giant cells | Sheets of macrophages filled with bacilli; no granulomas | Coalescent caseating granulomas; cavitation |
| Lymph nodes | Prominently involved, caseating | Often involved | Less prominent |
| Cavitation | Absent | Absent | Characteristic, apical |
| Outcome | 95% heal (Ranke complex); 5% progress | High morbidity; miliary dissemination | Variable; may heal or progress |
| Infectivity | Low (no cavity) | High (hematogenous) | High (cavities → infectious sputum) |
Aetiopathogenesis is for exam of 2 marks how to present clearly and get whole mask in diagramatic form
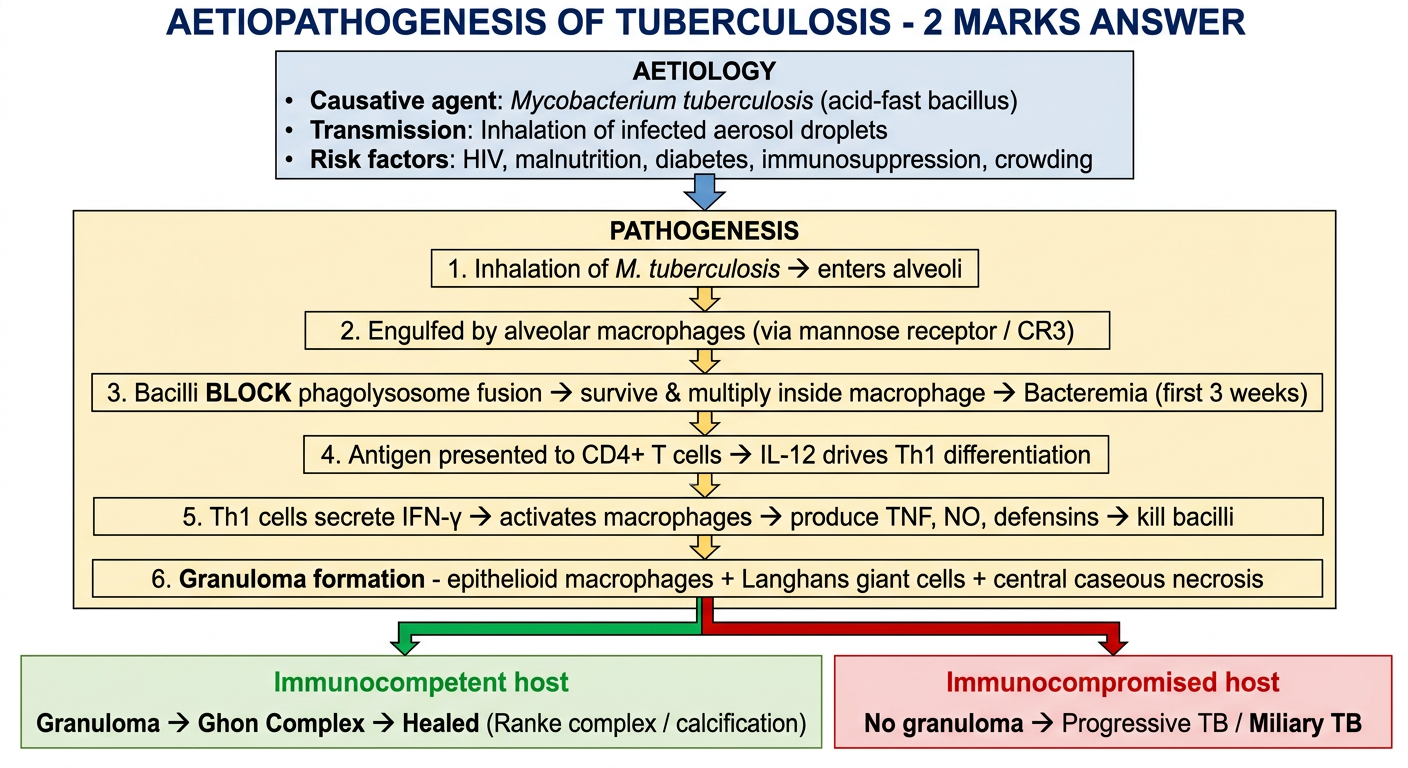
A clean, exam-ready flowchart diagram titled "Aetiopathogenesis of Tuberculosis - 2 Marks Answer" showing: Top section - AETIOLOGY box: - Causative agent: Mycobacterium tuberculosis (acid-fast bacillus) - Transmission: Inhalation of infected aerosol droplets - Risk factors: HIV, malnutrition, diabetes, immunosuppression, crowding Then a downward arrow to PATHOGENESIS section as a numbered sequential flowchart: Step 1: Inhalation of M. tuberculosis → enters alveoli Step 2: Engulfed by alveolar macrophages (via mannose receptor / CR3) Step 3: Bacilli BLOCK phagolysosome fusion → survive & multiply inside macrophage → Bacteremia (first 3 weeks) Step 4: Antigen presented to CD4+ T cells → IL-12 drives Th1 differentiation Step 5: Th1 cells secrete IFN-γ → activates macrophages → produce TNF, NO, defensins → kill bacilli Step 6: Granuloma formation - epithelioid macrophages + Langhans giant cells + central caseous necrosis Two outcome boxes at the bottom connected by arrows: LEFT (green): Immunocompetent host → Granuloma → Ghon Complex → Healed (Ranke complex / calcification) RIGHT (red): Immunocompromised host → No granuloma → Progressive TB / Miliary TB The diagram should use color-coded boxes, clean arrows, bold key terms, white background, professional medical exam style, easy to memorize layout
How to Write a Perfect 2-Mark Answer in Exams
- Caused by Mycobacterium tuberculosis (acid-fast bacillus)
- Spread by inhalation of infected aerosol droplets from active cases
- Inhaled bacilli engulfed by alveolar macrophages
- Bacilli block phagolysosome fusion → survive and multiply → bacteremia
- After ~3 weeks: CD4+ T cells activated → Th1 response → IFN-γ secreted
- IFN-γ activates macrophages → produce TNF + nitric oxide → kill bacilli
- Granuloma forms (epithelioid cells + Langhans giant cells + caseous necrosis)
- Outcome: Immunocompetent → Ghon complex → healing; Immunocompromised → progressive/miliary TB
| Tip | Why it works |
|---|---|
| Name the organism in italics | Shows precision |
| Use the word "cell-mediated immunity (CMI)" | Examiner's expected term |
| Mention IL-12 → Th1 → IFN-γ axis | Shows depth in 1 line |
| End with the two outcomes | Shows complete understanding |
| Write 1 box or arrow flow if time allows | Visual = instant marks |
Generate a PDF quick reference for TB exam prep
mkdir -p /home/daytona/workspace/tb-exam-prep && ls /home/daytona/workspace/tb-e…
~/tb-exam-prep/generate_tb_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import cm, mm
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether
)
from reportlab.platypus.flowables import Flowable
from reportlab.graphics.shapes import Drawing, Rect, String, Line, Arrow
from reportlab.graphics import renderPDF
import io
OUTPUT = "/home/daytona/workspace/tb-exam-prep/TB_Exam_Quick_Reference.pdf"
# ── Color palette ──────────────────────────────────────────────────────────────
C_DARK_RED = colors.HexColor("#8B1A1A")
C_MID_RED = colors.HexColor("#C0392B")
C_ORANGE = colors.HexColor("#E67E22")
C_TEAL = colors.HexColor("#1A6B6B")
C_GREEN = colors.HexColor("#1E8449")
C_BLUE = colors.HexColor("#1A4B8B")
C_PURPLE = colors.HexColor("#6C3483")
C_LIGHT_GREY = colors.HexColor("#F4F6F7")
C_HEADER_BG = colors.HexColor("#1A1A2E")
C_ACCENT = colors.HexColor("#E74C3C")
C_YELLOW_BG = colors.HexColor("#FEF9E7")
C_GREEN_BG = colors.HexColor("#EAFAF1")
C_RED_BG = colors.HexColor("#FDEDEC")
C_BLUE_BG = colors.HexColor("#EBF5FB")
C_PURPLE_BG = colors.HexColor("#F5EEF8")
C_WHITE = colors.white
C_BLACK = colors.black
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
leftMargin=1.5*cm, rightMargin=1.5*cm,
topMargin=1.5*cm, bottomMargin=1.5*cm
)
W = A4[0] - 3*cm # usable width
story = []
# ── Styles ─────────────────────────────────────────────────────────────────────
base = getSampleStyleSheet()
def S(name, **kw):
return ParagraphStyle(name, **kw)
title_style = S("Title",
fontSize=22, fontName="Helvetica-Bold", textColor=C_WHITE,
alignment=TA_CENTER, spaceAfter=4, leading=28)
subtitle_style = S("Subtitle",
fontSize=11, fontName="Helvetica", textColor=colors.HexColor("#BDC3C7"),
alignment=TA_CENTER, spaceAfter=2)
section_style = S("Section",
fontSize=12, fontName="Helvetica-Bold", textColor=C_WHITE,
spaceBefore=6, spaceAfter=4, leftIndent=6)
body_style = S("Body",
fontSize=8.5, fontName="Helvetica", textColor=C_BLACK,
spaceAfter=3, leading=13, alignment=TA_LEFT)
bold_body = S("BoldBody",
fontSize=8.5, fontName="Helvetica-Bold", textColor=C_BLACK,
spaceAfter=3, leading=13)
small_style = S("Small",
fontSize=7.5, fontName="Helvetica", textColor=colors.HexColor("#444444"),
leading=11, spaceAfter=2)
small_bold = S("SmallBold",
fontSize=7.5, fontName="Helvetica-Bold", textColor=C_BLACK,
leading=11, spaceAfter=2)
bullet_style = S("Bullet",
fontSize=8.5, fontName="Helvetica", textColor=C_BLACK,
spaceAfter=2, leading=13, leftIndent=10, firstLineIndent=-10)
key_style = S("Key",
fontSize=8, fontName="Helvetica-Bold", textColor=C_MID_RED,
spaceAfter=2, leading=12)
mnemonic_style = S("Mnemonic",
fontSize=9, fontName="Helvetica-Bold", textColor=C_PURPLE,
spaceAfter=3, leading=14)
footer_style = S("Footer",
fontSize=7, fontName="Helvetica-Oblique",
textColor=colors.HexColor("#888888"), alignment=TA_CENTER)
# ── Helper functions ────────────────────────────────────────────────────────────
def section_header(text, bg=C_DARK_RED, text_col=C_WHITE):
data = [[Paragraph(f"<b>{text}</b>", ParagraphStyle("SH",
fontSize=11, fontName="Helvetica-Bold", textColor=text_col,
alignment=TA_LEFT, leading=16))]]
t = Table(data, colWidths=[W])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), bg),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 10),
("RIGHTPADDING", (0,0), (-1,-1), 8),
("ROUNDEDCORNERS", [4]),
]))
return t
def colored_table(data, col_widths, header_bg=C_TEAL, row_bg1=C_WHITE, row_bg2=C_LIGHT_GREY,
header_text=C_WHITE, font_size=8):
cell_style = ParagraphStyle("CT", fontSize=font_size, fontName="Helvetica",
textColor=C_BLACK, leading=11, spaceAfter=0)
hdr_style = ParagraphStyle("CTH", fontSize=font_size, fontName="Helvetica-Bold",
textColor=header_text, leading=11, spaceAfter=0)
table_data = []
for ri, row in enumerate(data):
styled_row = []
for ci, cell in enumerate(row):
st = hdr_style if ri == 0 else cell_style
styled_row.append(Paragraph(str(cell), st))
table_data.append(styled_row)
t = Table(table_data, colWidths=col_widths, repeatRows=1)
style_cmds = [
("BACKGROUND", (0,0), (-1,0), header_bg),
("TEXTCOLOR", (0,0), (-1,0), header_text),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,-1), font_size),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#CCCCCC")),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 5),
("RIGHTPADDING", (0,0), (-1,-1), 5),
]
for i in range(1, len(data)):
bg = row_bg1 if i % 2 == 1 else row_bg2
style_cmds.append(("BACKGROUND", (0,i), (-1,i), bg))
t.setStyle(TableStyle(style_cmds))
return t
def highlight_box(content_paras, bg=C_YELLOW_BG, border=C_ORANGE, label=None):
inner = []
if label:
inner.append(Paragraph(f"<b>{label}</b>",
ParagraphStyle("HL", fontSize=9, fontName="Helvetica-Bold",
textColor=border, spaceAfter=4, leading=13)))
inner.extend(content_paras)
data = [[inner]]
t = Table(data, colWidths=[W])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), bg),
("BOX", (0,0), (-1,-1), 1.5, border),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING", (0,0), (-1,-1), 8),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 6),
]))
return t
def two_col(left_content, right_content, left_w=None, right_w=None):
lw = left_w or W * 0.49
rw = right_w or W * 0.49
data = [[left_content, right_content]]
t = Table(data, colWidths=[lw, rw])
t.setStyle(TableStyle([
("VALIGN", (0,0), (-1,-1), "TOP"),
("LEFTPADDING", (0,0), (-1,-1), 0),
("RIGHTPADDING", (0,0), (-1,-1), 0),
("TOPPADDING", (0,0), (-1,-1), 0),
("BOTTOMPADDING", (0,0), (-1,-1), 0),
("LINEAFTER", (0,0), (0,-1), 0.5, colors.HexColor("#DDDDDD")),
]))
return t
def sp(h=4):
return Spacer(1, h)
def hr(col=colors.HexColor("#DDDDDD")):
return HRFlowable(width="100%", thickness=0.5, color=col, spaceAfter=4, spaceBefore=4)
# ═══════════════════════════════════════════════════════════════════════════════
# COVER / HEADER BANNER
# ═══════════════════════════════════════════════════════════════════════════════
banner_data = [[
Paragraph("TUBERCULOSIS", title_style),
Paragraph("Quick Reference for Medical Exams", subtitle_style),
Paragraph("Pathology · Microbiology · Clinical Features · Exam Answers", subtitle_style),
]]
banner = Table([[
Paragraph("TUBERCULOSIS", ParagraphStyle("T2", fontSize=24, fontName="Helvetica-Bold",
textColor=C_WHITE, alignment=TA_CENTER, spaceAfter=3, leading=30)),
Paragraph("Quick Reference for Medical Exams", ParagraphStyle("S2", fontSize=11,
fontName="Helvetica", textColor=colors.HexColor("#E8E8E8"), alignment=TA_CENTER,
spaceAfter=2)),
Paragraph("Pathology · Microbiology · Clinical Features · Model Exam Answers",
ParagraphStyle("S3", fontSize=9, fontName="Helvetica-Oblique",
textColor=colors.HexColor("#BDC3C7"), alignment=TA_CENTER)),
]], colWidths=[W])
banner.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), C_HEADER_BG),
("TOPPADDING", (0,0), (-1,-1), 14),
("BOTTOMPADDING", (0,0), (-1,-1), 14),
("LEFTPADDING", (0,0), (-1,-1), 10),
("RIGHTPADDING", (0,0), (-1,-1), 10),
]))
story.append(banner)
story.append(sp(8))
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 1 AETIOLOGY
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_header("1. AETIOLOGY", bg=C_DARK_RED))
story.append(sp(4))
aet_left = [
Paragraph("<b>Causative organism:</b>", small_bold),
Paragraph("Mycobacterium tuberculosis (M. hominis)", small_style),
sp(3),
Paragraph("<b>Morphology:</b>", small_bold),
Paragraph("• Slender, straight/slightly curved rod", small_style),
Paragraph("• Acid-fast bacillus (AFB) — Ziehl-Neelsen stain", small_style),
Paragraph("• Non-motile, non-spore forming, aerobic", small_style),
Paragraph("• High lipid content cell wall (mycolic acids)", small_style),
sp(3),
Paragraph("<b>Other species:</b>", small_bold),
Paragraph("• M. bovis — unpasteurized milk (rare now)", small_style),
Paragraph("• M. avium complex — immunocompromised (AIDS)", small_style),
]
aet_right = [
Paragraph("<b>Transmission:</b>", small_bold),
Paragraph("Inhalation of infected <b>aerosol droplet nuclei</b>", small_style),
Paragraph("(person-to-person; active pulmonary TB case)", small_style),
sp(3),
Paragraph("<b>Risk Factors:</b>", small_bold),
Paragraph("• HIV infection (dominant risk factor)", small_style),
Paragraph("• Malnutrition / underweight", small_style),
Paragraph("• Diabetes mellitus", small_style),
Paragraph("• Silicosis, chronic lung disease", small_style),
Paragraph("• Crowding, poverty, poor ventilation", small_style),
Paragraph("• Hodgkin lymphoma, CRF, alcohol use disorder", small_style),
Paragraph("• Anti-TNF therapy, immunosuppressants", small_style),
Paragraph("• Age extremes (elderly, infants)", small_style),
]
# wrap each side in a transparent table so they stack
def col_wrap(items, width):
data = [[i] for i in items]
t = Table(data, colWidths=[width])
t.setStyle(TableStyle([
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING", (0,0), (-1,-1), 4),
("TOPPADDING", (0,0), (-1,-1), 1),
("BOTTOMPADDING", (0,0), (-1,-1), 1),
]))
return t
story.append(two_col(col_wrap(aet_left, W*0.49), col_wrap(aet_right, W*0.49)))
story.append(sp(6))
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 2 PATHOGENESIS FLOWCHART
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_header("2. PATHOGENESIS (Step-by-Step)", bg=C_BLUE))
story.append(sp(5))
def path_step(num, title, detail, bg, border):
content = [
Paragraph(f"<b>Step {num}: {title}</b>",
ParagraphStyle("PS", fontSize=8.5, fontName="Helvetica-Bold",
textColor=border, leading=13, spaceAfter=2)),
Paragraph(detail,
ParagraphStyle("PD", fontSize=8, fontName="Helvetica",
textColor=C_BLACK, leading=12)),
]
data = [[content]]
t = Table(data, colWidths=[W])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), bg),
("BOX", (0,0), (-1,-1), 1, border),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING", (0,0), (-1,-1), 8),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
]))
return t
def arrow_down():
data = [[Paragraph("▼", ParagraphStyle("ARR", fontSize=10, fontName="Helvetica",
textColor=colors.HexColor("#777777"), alignment=TA_CENTER))]]
t = Table(data, colWidths=[W])
t.setStyle(TableStyle([
("TOPPADDING", (0,0), (-1,-1), 1),
("BOTTOMPADDING", (0,0), (-1,-1), 1),
]))
return t
steps = [
(1, "Inhalation of M. tuberculosis",
"Bacilli carried in aerosol droplet nuclei (<5 µm) reach alveoli of lower upper lobe / upper lower lobe.",
colors.HexColor("#EBF5FB"), C_BLUE),
(2, "Phagocytosis by Alveolar Macrophages",
"Bacilli engulfed via mannose receptor and complement receptor (CR3). Inside phagosome, M. tuberculosis BLOCKS phagolysosome fusion → prevents acidification → blocks reactive oxygen/nitrogen species.",
colors.HexColor("#FEF9E7"), C_ORANGE),
(3, "Unchecked Bacillary Proliferation (First 3 weeks)",
"No cell-mediated immunity yet. Bacilli multiply freely within macrophages → bacteremia → seeding of multiple organs (lung, lymph nodes, liver, spleen, kidneys, meninges). Most are asymptomatic at this stage.",
colors.HexColor("#FDEDEC"), C_MID_RED),
(4, "Development of Cell-Mediated Immunity (~3 weeks)",
"Dendritic cells/macrophages present mycobacterial antigens (via MHC class II) to CD4+ T cells in draining lymph nodes. Macrophage-secreted IL-12 drives Th1 differentiation → Th1 cells secrete IFN-γ.",
colors.HexColor("#F5EEF8"), C_PURPLE),
(5, "Macrophage Activation & Bacterial Killing",
"IFN-γ activates macrophages → upregulate: (1) TNF — recruits monocytes for granuloma; (2) iNOS — produces NO and reactive nitrogen intermediates (kill mycobacteria); (3) Defensins — direct bactericidal action.",
colors.HexColor("#EAFAF1"), C_GREEN),
(6, "Granuloma Formation",
"IFN-γ drives macrophage → epithelioid histiocyte differentiation. Epithelioid cells aggregate; some fuse → Langhans giant cells (peripheral horseshoe nuclei). TNF + chemokines recruit more monocytes. Result: CASEATING GRANULOMA (central cheese-like necrosis + epithelioid cells + lymphocytes + giant cells).",
colors.HexColor("#FEF9E7"), C_ORANGE),
]
for i, (num, title, detail, bg, border) in enumerate(steps):
story.append(path_step(num, title, detail, bg, border))
if i < len(steps)-1:
story.append(arrow_down())
story.append(sp(5))
# Outcome box
outcome_data = [
["OUTCOME", "IMMUNOCOMPETENT HOST", "IMMUNOCOMPROMISED HOST"],
["Granuloma", "Well-formed caseating granuloma", "Absent or poorly formed"],
["Histology", "Epithelioid cells + Langhans giant cells + caseous necrosis", "Sheets of macrophages packed with bacilli (AFB+)"],
["Result", "Ghon complex → fibrosis → calcification (Ranke complex) → LATENT TB", "Progressive primary TB / Miliary TB"],
["CD4+ count", "Normal", "<200 cells/µL (HIV)"],
]
story.append(colored_table(outcome_data,
col_widths=[W*0.18, W*0.42, W*0.4],
header_bg=C_TEAL, font_size=7.5))
story.append(sp(6))
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 3 TYPES + MORPHOLOGY
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_header("3. TYPES AND MORPHOLOGY", bg=C_DARK_RED))
story.append(sp(5))
types_data = [
["FEATURE", "PRIMARY TB", "PROGRESSIVE PRIMARY TB", "SECONDARY (REACTIVATION) TB"],
["Host", "Previously unexposed, unsensitized", "Immunocompromised (HIV CD4 <200)", "Previously sensitized; waning immunity"],
["Timing", "First infection", "Shortly after primary (no containment)", "Decades after primary (reactivation) or reinfection"],
["Location", "Lower upper lobe / upper lower lobe, subpleural", "Diffuse / lower & middle lobes", "APEX of upper lobe (bilateral)"],
["Gross lesion", "1–1.5 cm Ghon focus (grey-white consolidation) + hilar LN caseation = Ghon complex", "Extensive consolidation, no walling off", "Small (<2 cm) apical focus → cavitation"],
["Histology", "Caseating & non-caseating granulomas; epithelioid cells + Langhans giant cells", "Sheets of macrophages filled with bacilli; NO granulomas", "Coalescent caseating granuloma nodules; eventually cavity with caseous lining"],
["Lymph nodes", "Prominently involved (caseating)", "Often involved", "Less prominent (pre-existing hypersensitivity walls off quickly)"],
["Cavitation", "Absent", "Absent", "CHARACTERISTIC — bronchial erosion → ragged irregular cavity → hemoptysis"],
["Sputum AFB", "Negative (no cavity)", "Positive (dissemination)", "POSITIVE — major source of infection"],
["Outcome", "95%: Ranke complex (calcified). 5%: progress", "Miliary TB, high morbidity", "Heal with fibrosis OR progress to miliary/extrapulmonary TB"],
]
story.append(colored_table(types_data,
col_widths=[W*0.16, W*0.27, W*0.27, W*0.3],
header_bg=C_DARK_RED, font_size=7))
story.append(sp(6))
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 4 SPREAD / PROGRESSIVE SECONDARY TB
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_header("4. PROGRESSIVE SECONDARY TB — SPREAD PATHWAYS", bg=C_TEAL))
story.append(sp(4))
spread_data = [
["PATHWAY", "MECHANISM", "LESION / RESULT"],
["Endobronchial / airway", "Caseous material erodes into bronchus", "Cavity + sputum infectivity; endobronchial / laryngeal TB"],
["Lymphatic", "Lymphatic drainage from lung", "Lymphadenitis — cervical (scrofula) most common extrapulmonary form"],
["Pulmonary arterial (hematogenous)", "Via pulmonary arteries → lung", "Miliary pulmonary TB — 2 mm yellow-white foci (millet seeds)"],
["Systemic hematogenous", "Via blood to all organs", "Systemic miliary TB: liver, bone marrow, spleen, adrenals, meninges, kidneys, fallopian tubes, epididymis"],
["Pleural extension", "Direct spread", "Serous effusion, tuberculous empyema, fibrous pleuritis"],
["Vertebral seeding", "Hematogenous to vertebrae", "Pott disease; paraspinal cold abscess"],
["Swallowed sputum", "Infected material ingested", "Intestinal TB (ileum >> colon; mucosal ulceration over lymphoid aggregates)"],
]
story.append(colored_table(spread_data,
col_widths=[W*0.23, W*0.35, W*0.42],
header_bg=C_TEAL, font_size=7.5))
story.append(sp(6))
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 5 GRANULOMA — KEY HISTOLOGY
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_header("5. GRANULOMA — HISTOLOGICAL FEATURES", bg=C_PURPLE))
story.append(sp(4))
gran_left = [
Paragraph("<b>Composition (centre → periphery):</b>", small_bold),
Paragraph("1. Central caseous necrosis (cheese-like, amorphous eosinophilic)", small_style),
Paragraph("2. Epithelioid macrophages (activated, pale pink cytoplasm)", small_style),
Paragraph("3. Langhans giant cells (peripheral/horseshoe arrangement of nuclei)", small_style),
Paragraph("4. Rim of lymphocytes (CD4+ T cells predominant)", small_style),
Paragraph("5. Outer fibrous capsule (in healing lesions)", small_style),
sp(4),
Paragraph("<b>Special stain for organisms:</b>", small_bold),
Paragraph("Ziehl-Neelsen (ZN) stain → bright red acid-fast bacilli on blue background", small_style),
Paragraph("Auramine-rhodamine fluorescence stain (more sensitive)", small_style),
sp(4),
Paragraph("<b>Note on granuloma absence:</b>", small_bold),
Paragraph("In immunocompromised (HIV CD4 <200), granulomas are absent → sheets of macrophages + abundant AFB (ZN stain +++)", small_style),
]
gran_right = [
Paragraph("<b>Outcomes of granuloma:</b>", small_bold),
Paragraph("1. Healing with fibrosis → calcification", small_style),
Paragraph("2. Liquefaction of caseous material → cavity", small_style),
Paragraph("3. Progressive enlargement (if immunity fails)", small_style),
sp(4),
Paragraph("<b>Key molecular mediators in granuloma:</b>", small_bold),
Paragraph("• IL-12 → Th1 induction", small_style),
Paragraph("• IFN-γ → macrophage activation", small_style),
Paragraph("• TNF → monocyte recruitment + granuloma integrity", small_style),
Paragraph("• NO (nitric oxide) → mycobacterial killing", small_style),
sp(4),
Paragraph("<b>Clinical relevance of TNF:</b>", small_bold),
Paragraph("Anti-TNF drugs (infliximab, etanercept) used in RA/IBD → RISK of TB reactivation. Screen before starting anti-TNF!", small_style),
]
story.append(two_col(col_wrap(gran_left, W*0.49), col_wrap(gran_right, W*0.49)))
story.append(sp(6))
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 6 DIAGNOSTIC TESTS
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_header("6. DIAGNOSTIC TESTS", bg=C_BLUE))
story.append(sp(4))
diag_data = [
["TEST", "PRINCIPLE", "POSITIVE RESULT", "LIMITATION"],
["Tuberculin (Mantoux/PPD)", "Delayed hypersensitivity (Type IV); intradermal injection of PPD", "≥10 mm induration at 48–72 hrs (≥5 mm if HIV+)", "False-negative: HIV, malnutrition, sarcoidosis, overwhelming TB. False-positive: BCG, atypical mycobacteria"],
["IGRA (IFN-γ Release Assay)", "In vitro: T cells stimulated with MTB antigens; IFN-γ measured", "Elevated IFN-γ response", "Cannot differentiate latent vs active. Not affected by BCG"],
["Sputum AFB smear (ZN)", "Acid-fast staining of sputum", "Bright red bacilli", "Low sensitivity (~60%); needs 10,000 bacilli/mL"],
["Sputum culture (Lowenstein-Jensen)", "Growth of M. tuberculosis", "Buff/rough colonies in 3–8 weeks", "Slow (weeks). Gold standard for sensitivity"],
["GeneXpert MTB/RIF (PCR)", "Molecular detection of MTB + rifampicin resistance", "MTB detected ± RIF resistance", "Rapid (2 hrs). Best for resource-limited settings"],
["CXR", "Imaging", "Primary: Ghon complex, hilar LN. Secondary: apical cavitation, fibrosis", "Not specific; overlap with other diseases"],
]
story.append(colored_table(diag_data,
col_widths=[W*0.18, W*0.27, W*0.22, W*0.33],
header_bg=C_BLUE, font_size=7))
story.append(sp(6))
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 7 EXAM MNEMONICS
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_header("7. HIGH-YIELD MNEMONICS & EXAM TRICKS", bg=C_ORANGE))
story.append(sp(4))
mnem_data = [
[
Paragraph("<b>🔑 PATHOGENESIS KEY CHAIN</b>\n\nInhale → Macrophage → Block lyso-fusion → Multiply →\nBacteremia → IL-12 → Th1 → IFN-γ → Activate Mφ →\nTNF + NO + Defensins → Kill / Granuloma → Caseous necrosis",
ParagraphStyle("MN", fontSize=8.5, fontName="Helvetica", textColor=C_DARK_RED,
leading=14, spaceAfter=3)),
],
[
Paragraph("<b>🔑 GRANULOMA LAYERS mnemonic — \"Caseous Epithelioid Giants Like Fibrosis\"</b>\n"
"C - Central caseous necrosis\n"
"E - Epithelioid macrophages\n"
"G - Giant cells (Langhans)\n"
"L - Lymphocytes (rim)\n"
"F - Fibrous capsule (healed)",
ParagraphStyle("MN2", fontSize=8.5, fontName="Helvetica", textColor=C_PURPLE,
leading=14, spaceAfter=3)),
],
[
Paragraph("<b>🔑 PRIMARY TB sites — \"Lower Upper or Upper Lower\"</b>\n"
"Lower part of UPPER lobe OR Upper part of LOWER lobe — always near pleura\n"
"Secondary TB → APEX of upper lobe (bilateral)",
ParagraphStyle("MN3", fontSize=8.5, fontName="Helvetica", textColor=C_TEAL,
leading=14, spaceAfter=3)),
],
[
Paragraph("<b>🔑 Extrapulmonary sites — \"MALES BIKE\"</b>\n"
"M - Meninges A - Adrenals L - Liver E - Epididymis S - Spleen\n"
"B - Bone marrow I - Intestines K - Kidneys E - (Fallopian) tubEs",
ParagraphStyle("MN4", fontSize=8.5, fontName="Helvetica", textColor=C_GREEN,
leading=14, spaceAfter=3)),
],
]
mnem_table = Table(mnem_data, colWidths=[W])
mnem_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (0,0), colors.HexColor("#FDEDEC")),
("BACKGROUND", (0,1), (0,1), colors.HexColor("#F5EEF8")),
("BACKGROUND", (0,2), (0,2), colors.HexColor("#EBF5FB")),
("BACKGROUND", (0,3), (0,3), colors.HexColor("#EAFAF1")),
("BOX", (0,0), (-1,-1), 0.5, colors.HexColor("#DDDDDD")),
("LINEBELOW", (0,0), (0,2), 0.5, colors.HexColor("#DDDDDD")),
("TOPPADDING", (0,0), (-1,-1), 7),
("BOTTOMPADDING", (0,0), (-1,-1), 7),
("LEFTPADDING", (0,0), (-1,-1), 10),
("RIGHTPADDING", (0,0), (-1,-1), 10),
]))
story.append(mnem_table)
story.append(sp(6))
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 8 MODEL EXAM ANSWERS
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_header("8. MODEL EXAM ANSWERS", bg=C_DARK_RED))
story.append(sp(4))
# 2-mark answer
q2_content = [
Paragraph("<b>Q: Write the aetiopathogenesis of tuberculosis. (2 marks)</b>",
ParagraphStyle("Q", fontSize=9, fontName="Helvetica-Bold", textColor=C_DARK_RED,
spaceAfter=4, leading=13)),
Paragraph("<b>Aetiology:</b> Caused by <i>Mycobacterium tuberculosis</i> (acid-fast bacillus). "
"Transmitted by inhalation of infected aerosol droplet nuclei from an active case.", body_style),
Paragraph("<b>Pathogenesis:</b>", body_style),
Paragraph("1. Inhaled bacilli engulfed by alveolar macrophages via mannose receptor / CR3.", bullet_style),
Paragraph("2. Bacilli block phagolysosome fusion → survive and multiply → bacteremia (first 3 weeks).", bullet_style),
Paragraph("3. ~3 weeks: CD4+ T cells activated → IL-12 → Th1 → IFN-γ secretion.", bullet_style),
Paragraph("4. IFN-γ activates macrophages → TNF + nitric oxide + defensins → kill bacilli.", bullet_style),
Paragraph("5. Granuloma forms: epithelioid cells + Langhans giant cells + caseous necrosis.", bullet_style),
Paragraph("6. Immunocompetent → Ghon complex → healing; Immunocompromised → progressive/miliary TB.", bullet_style),
]
story.append(highlight_box(q2_content, bg=C_RED_BG, border=C_MID_RED))
story.append(sp(5))
# 5-mark answer outline
q5_content = [
Paragraph("<b>Q: Describe the morphology of primary and secondary tuberculosis. (5 marks)</b>",
ParagraphStyle("Q5", fontSize=9, fontName="Helvetica-Bold", textColor=C_BLUE,
spaceAfter=4, leading=13)),
Paragraph("<b>Primary TB Morphology (2 marks):</b>", bold_body),
Paragraph("• Site: Lower part of upper lobe / upper part of lower lobe, near pleura", bullet_style),
Paragraph("• Ghon focus: 1–1.5 cm grey-white consolidation with central caseous necrosis", bullet_style),
Paragraph("• Ghon complex: Ghon focus + caseating hilar lymph nodes + lymphangitis", bullet_style),
Paragraph("• Histology: Caseating granulomas with epithelioid cells, Langhans giant cells, lymphocytes", bullet_style),
Paragraph("• Outcome: 95% fibrosis + calcification (Ranke complex)", bullet_style),
sp(3),
Paragraph("<b>Secondary TB Morphology (3 marks):</b>", bold_body),
Paragraph("• Site: Apex of upper lobes (bilateral) — due to high O2 tension", bullet_style),
Paragraph("• Initial lesion: <2 cm firm, grey-yellow apical focus with variable caseation + peripheral fibrosis", bullet_style),
Paragraph("• Progressive disease: Caseation liquefies → erodes bronchus → CAVITY (ragged, irregular)", bullet_style),
Paragraph("• Cavity complications: Hemoptysis (vessel erosion), endobronchial spread, miliary TB", bullet_style),
Paragraph("• Histology: Coalescent caseating granuloma nodules; bacilli visible in early phases", bullet_style),
Paragraph("• Spread: Airways → endobronchial TB; lymphatics → lymphadenitis (scrofula); blood → miliary TB; pleura → empyema", bullet_style),
]
story.append(highlight_box(q5_content, bg=C_BLUE_BG, border=C_BLUE))
story.append(sp(5))
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 9 RAPID-FIRE HIGH-YIELD FACTS
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_header("9. RAPID-FIRE HIGH-YIELD FACTS", bg=C_TEAL))
story.append(sp(4))
hiy_left = [
Paragraph("<b>Stain for M. tuberculosis:</b>", small_bold),
Paragraph("Ziehl-Neelsen (carbol fuchsin) → bright RED on blue background", small_style),
sp(3),
Paragraph("<b>Gold standard culture medium:</b>", small_bold),
Paragraph("Lowenstein-Jensen (LJ) medium — colonies in 3–8 weeks", small_style),
sp(3),
Paragraph("<b>Gold standard diagnosis:</b>", small_bold),
Paragraph("Culture of M. tuberculosis", small_style),
sp(3),
Paragraph("<b>Fastest diagnostic test:</b>", small_bold),
Paragraph("GeneXpert MTB/RIF (PCR) — result in 2 hours", small_style),
sp(3),
Paragraph("<b>Tuberculin test peak induration:</b>", small_bold),
Paragraph("48–72 hours (Type IV delayed hypersensitivity)", small_style),
sp(3),
Paragraph("<b>Ghon focus location:</b>", small_bold),
Paragraph("Lower part of upper lobe OR upper part of lower lobe", small_style),
sp(3),
Paragraph("<b>Ghon complex =</b>", small_bold),
Paragraph("Ghon focus + hilar lymph node + lymphangitis", small_style),
sp(3),
Paragraph("<b>Ranke complex =</b>", small_bold),
Paragraph("Calcified Ghon complex on x-ray (healed primary TB)", small_style),
]
hiy_right = [
Paragraph("<b>Most common extrapulmonary TB:</b>", small_bold),
Paragraph("Lymphadenitis (cervical = scrofula)", small_style),
sp(3),
Paragraph("<b>Vertebral TB name:</b>", small_bold),
Paragraph("Pott disease (cold abscess may present as abdominal mass)", small_style),
sp(3),
Paragraph("<b>Miliary TB:</b>", small_bold),
Paragraph("2 mm yellow-white foci scattered in lung (millet seeds)", small_style),
sp(3),
Paragraph("<b>Cell that KILLS mycobacteria:</b>", small_bold),
Paragraph("Activated macrophage (via IFN-γ → NO + defensins)", small_style),
sp(3),
Paragraph("<b>Key cytokine for Th1 induction:</b>", small_bold),
Paragraph("IL-12 (from macrophages/dendritic cells)", small_style),
sp(3),
Paragraph("<b>Key cytokine for macrophage activation:</b>", small_bold),
Paragraph("IFN-γ (from Th1 cells)", small_style),
sp(3),
Paragraph("<b>Anti-TNF therapy → risk:</b>", small_bold),
Paragraph("TB reactivation (TNF critical for granuloma integrity)", small_style),
sp(3),
Paragraph("<b>Langhans giant cell nucleus arrangement:</b>", small_bold),
Paragraph("Peripheral / horseshoe pattern", small_style),
]
story.append(two_col(col_wrap(hiy_left, W*0.49), col_wrap(hiy_right, W*0.49)))
story.append(sp(8))
# ── Footer ─────────────────────────────────────────────────────────────────────
story.append(hr())
story.append(Paragraph(
"Source: Robbins & Kumar Basic Pathology (Robbins Pathology) | Generated for Medical Exam Preparation",
footer_style))
# ── Build ──────────────────────────────────────────────────────────────────────
doc.build(story)
print(f"PDF created: {OUTPUT}")
cd /home/daytona/workspace/tb-exam-prep && python generate_tb_pdf.py 2>&1
~/tb-exam-prep/generate_tb_pdf.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/tb-exam-prep/generate_tb_pdf.py'
cd /home/daytona/workspace/tb-exam-prep && python generate_tb_pdf.py 2>&1
ls -lh /home/daytona/workspace/tb-exam-prep/TB_Exam_Quick_Reference.pdf
TB Exam Quick Reference
PDF Document · PDF
What's inside the PDF (9 sections):
| Section | Content |
|---|---|
| 1. Aetiology | Organism, morphology, transmission, risk factors in two-column layout |
| 2. Pathogenesis flowchart | 6 color-coded sequential steps from inhalation → granuloma, with outcome table |
| 3. Types & Morphology | Full comparison table: Primary / Progressive Primary / Secondary TB across 10 features |
| 4. Spread Pathways | All routes (airway, lymphatic, hematogenous, pleural, vertebral, intestinal) |
| 5. Granuloma Histology | Composition layers, special stains, molecular mediators, clinical relevance |
| 6. Diagnostic Tests | Mantoux, IGRA, ZN smear, culture, GeneXpert, CXR — principles, results, limitations |
| 7. Mnemonics | 4 exam mnemonics including "MALES BIKE" for extrapulmonary sites |
| 8. Model Exam Answers | Ready-to-use 2-mark and 5-mark model answers formatted for exam writing |
| 9. Rapid-Fire Facts | 16 high-yield one-liners for quick last-night revision |
Defining of- Could you go back to thinking? Uh, can you do the thinking in 999 program? Definition of critical thinking critical thinking in nursing program why it is important skills of critical thinking about 15 points characteristics of critical thinking in our 15 points nor with thinking and respect thinking difference between about
critical thinking in nursing definition skills characteristics 2024
https://www.pearson.com/content/dam/one-dot-com/one-dot-com/…
Critical Thinking in Nursing
1. Definition of Critical Thinking
2. Critical Thinking in Nursing Programs
| Nursing Process Step | Critical Thinking Application |
|---|---|
| Assessment | Collect and verify data; observe, listen, interpret |
| Diagnosis | Analyze data patterns; identify actual/risk problems |
| Planning | Set priorities; select evidence-based interventions |
| Implementation | Apply knowledge; adapt care to individual patient |
| Evaluation | Reflect on outcomes; revise the care plan |
- Nursing is a dynamic environment where conditions change rapidly
- Students must shift from rote memorization to active reasoning
- Clinical simulations, case studies, concept mapping, and reflective journals are all tools used to build critical thinking
- Programs require students to question assumptions, not just follow protocols
3. Why Critical Thinking is Important in Nursing
- Patient safety - Roughly 400,000 hospitalized patients experience preventable harm yearly due to medical errors. Critical thinking is the primary defense
- Sound clinical decision-making - Nurses make dozens of patient-care decisions per shift; not all have clear textbook answers
- Early recognition of deterioration - Critical thinkers notice subtle changes in patient status before a crisis develops
- Prioritization - Multiple patients, multiple problems; critical thinking determines who needs care first
- Evidence-based practice - Evaluating research and applying it correctly requires analytical skill
- Avoiding "groupthink" - Prevents blindly following others' decisions without independent evaluation
- Ethical decision-making - Weighing benefits vs. harm in complex moral situations
- Effective communication - Organizing clinical findings logically for handoffs (SBAR) and documentation
- Adaptability - Handling unexpected complications requires flexibility and rapid re-assessment
- Professional accountability - Nurses are legally and ethically responsible for their judgments
4. Skills of Critical Thinking (15 Points)
- Critical analysis - Applying systematic questions to a situation to identify what is essential and what is not
- Inductive reasoning - Drawing general conclusions from specific patient observations ("this patient's pattern suggests...")
- Deductive reasoning - Applying a general principle to a specific case ("patients with these ABG values need oxygen")
- Making valid inferences - Drawing logical conclusions from available data without jumping to unwarranted conclusions
- Differentiating facts from opinions - Separating objective clinical data from subjective impressions or assumptions
- Evaluating credibility of information - Assessing the reliability of sources, lab reports, and patient/family statements
- Clarifying concepts - Ensuring shared understanding of terms and ideas between nurse, patient, and team
- Recognizing assumptions - Identifying unstated beliefs that may bias assessment or care planning
- Applying standards - Comparing care actions to established professional, ethical, and legal standards
- Discriminating - Distinguishing relevant from irrelevant data; recognizing inconsistencies in clinical findings
- Information seeking - Actively searching for the most current, complete, and relevant data before deciding
- Logical reasoning - Using rational, step-by-step thinking to connect assessments to interventions
- Predicting - Anticipating likely outcomes or complications based on current data and clinical knowledge
- Transforming knowledge - Converting theoretical knowledge into practical, patient-specific action
- Reflective thinking - Looking back on decisions made, honestly evaluating outcomes, and adjusting future practice
5. Characteristics of Critical Thinking (15 Points)
- Independence of thought - Thinks for oneself; not swayed by authority or peer pressure without evidence
- Intellectual curiosity - Asks "why?" and seeks understanding beyond surface-level facts
- Intellectual humility - Acknowledges own limitations, gaps in knowledge, and potential for error
- Open-mindedness - Considers multiple perspectives and alternative explanations without bias
- Fair-mindedness - Applies the same standards of evidence to all views; avoids double standards
- Intellectual integrity - Consistent application of standards; does not rationalize or cut corners
- Perseverance - Continues to work through difficult problems even when the answer is not obvious
- Confidence - Trusts in well-reasoned conclusions; acts decisively when evidence supports it
- Contextual perspective - Considers the full context - patient history, culture, environment, and values
- Creativity - Generates novel, individualized solutions when standard approaches are insufficient
- Flexibility - Adjusts thinking and care plans as new information emerges
- Intuition - Recognizes patterns from experience; uses "gut sense" grounded in knowledge (not guesswork)
- Reflection - Deliberately and honestly evaluates one's own thinking processes and actions
- Inquisitiveness - Desires to learn continuously; not satisfied with "we've always done it this way"
- Self-awareness - Recognizes when emotions, biases, or fatigue are affecting judgment and corrects accordingly
6. Difference Between Critical Thinking, Normal (Ordinary) Thinking, and Reflective Thinking
| FEATURE | NORMAL (ORDINARY) THINKING | CRITICAL THINKING | REFLECTIVE THINKING |
|---|---|---|---|
| Definition | Automatic, routine thought based on habit and immediate impression | Purposeful, disciplined analysis and evaluation of information to reach a reasoned judgment | Deliberate looking back at past experiences/decisions to learn from them |
| Process | Passive, spontaneous, unreflective | Active, intentional, structured | Retrospective and introspective |
| Basis | Personal assumption, emotion, routine | Evidence, logic, standards, and reasoned analysis | Past experience and self-examination |
| Goal | Satisfy immediate needs; follow the familiar path | Reach the best possible decision or solution | Improve future thinking and practice |
| Questioning | Rarely questions assumptions | Constantly questions assumptions, sources, and conclusions | Questions what was done and why it worked or failed |
| Bias | Often influenced by bias, emotion, shortcuts | Actively identifies and counters bias | Recognizes how past bias affected outcomes |
| Flexibility | Rigid; resistant to change | Highly flexible; adapts to new evidence | Flexible in learning from past errors |
| Creativity | Low; defaults to what is known | High; generates new solutions | Moderate; applies lessons creatively going forward |
| Depth | Shallow and surface-level | Deep, multi-layered analysis | Moderate - focused on the meaning of a specific past event |
| In Nursing | Following a protocol without thinking why | Adapting care based on individual patient assessment and evidence | Reviewing a medication error to prevent future recurrence |
| Time orientation | Present only | Present and future (anticipatory) | Past (but aimed at future improvement) |
| Example | Giving a patient pain medication because it is "time" | Assessing whether the current pain score, medication history, and vitals actually indicate this is the right medication and dose now | After a patient deteriorated, reviewing the assessment findings that were missed and why they were overlooked |
Summary Triangle to Remember:
NORMAL THINKING → "I do what I always do"
REFLECTIVE THINKING → "Why did I do that? What did I learn?"
CRITICAL THINKING → "What is the best action based on all available evidence right now?"
Generate a practice exam with 10 critical thinking-based NCLEX questions
No difference between norvic and expert thinking about 18 points
Benner novice to expert nursing theory differences stages 2024
PART A: Novice vs Expert Thinking in Nursing - 18-Point Comparison
Background: Benner's 5 Stages of Nursing Development
| Stage | Who | Experience |
|---|---|---|
| 1. Novice | Nursing student | No clinical experience |
| 2. Advanced Beginner | New graduate nurse | 0-2 years |
| 3. Competent | Developing nurse | 1-3 years same area |
| 4. Proficient | Experienced nurse | 3-5 years |
| 5. Expert | Master clinician | 5+ years + deep pattern recognition |
18-Point Difference: Novice vs Expert Thinking
| # | FEATURE | NOVICE THINKING | EXPERT THINKING |
|---|---|---|---|
| 1 | Basis of decisions | Follows textbook rules, protocols, and checklists rigidly | Uses intuition grounded in deep experience; goes beyond rules |
| 2 | Clinical judgment | Slow, step-by-step, requires deliberate effort for every decision | Rapid, fluid, automatic - pattern recognition kicks in instantly |
| 3 | Perception of situation | Sees isolated facts and tasks ("I need to give this medication at 8am") | Sees the whole clinical picture holistically ("something is off with this patient") |
| 4 | Use of guidelines | Depends heavily on policies and written protocols as a crutch | Uses guidelines as a reference point, not a rigid script |
| 5 | Patient assessment | Collects data systematically but may miss subtle cues | Notices subtle abnormalities early; reads between the lines of vital signs and behavior |
| 6 | Prioritization | Struggles to prioritize; may treat all tasks as equally urgent | Instantly prioritizes based on patient acuity and anticipated needs |
| 7 | Response to unexpected events | Anxious, overwhelmed; needs supervisor guidance | Calm, decisive; draws on past similar experiences quickly |
| 8 | Knowledge application | Theoretical - applies textbook knowledge mechanically | Practical wisdom (phronesis) - integrates theory with real-world nuance |
| 9 | Recognition of deterioration | May miss early warning signs; acts only on obvious objective data | Senses "something is not right" before data confirms it (situational awareness) |
| 10 | Confidence | Low self-confidence; seeks frequent validation and reassurance | High, earned confidence; acts decisively within their scope |
| 11 | Error handling | May hide or be paralyzed by mistakes; fear-based response | Acknowledges errors openly; uses them as learning opportunities for the team |
| 12 | Time management | Task-focused; may fall behind because each task requires full attention | Goal-focused; manages time efficiently because tasks are automatized |
| 13 | Communication | Communicates facts but may lack clinical reasoning when reporting | Uses structured, confident clinical communication (SBAR) with clear rationale |
| 14 | Patient individuality | Treats patients as "cases" matching textbook descriptions | Treats each patient as a unique person; adjusts care to individual context |
| 15 | Critical thinking depth | Surface-level; analyzes one problem at a time | Multi-layered; considers several problems simultaneously with their interactions |
| 16 | Teaching ability | Cannot easily explain why they do what they do | Can articulate reasoning clearly; serves as a mentor and resource for team |
| 17 | Use of intuition | Distrusts intuition; only acts on measurable, written evidence | Trusts refined intuition developed through years of pattern recognition |
| 18 | Professional growth orientation | Focused on surviving and completing tasks correctly | Focused on improving outcomes, mentoring others, and advancing the profession |
Key Summary - The Core Difference in One Line:
Novice nurses ask: "What are the rules?" Expert nurses ask: "What does THIS patient need right now?"
PART B: 10 NCLEX-Style Critical Thinking Practice Questions
Question 1
✅ Answer: B Rationale: This patient is showing classic signs of hypovolemic shock (hypotension, tachycardia, tachypnea, oliguria <0.5 mL/kg/hr, altered mentation). This is a life-threatening emergency requiring immediate physician notification and fluid resuscitation. Pain medication (A) could worsen hypotension. Repositioning and waiting (C) wastes critical time. Standing orders alone (D) are insufficient for a deteriorating patient. CT Skill tested: Recognizing a life-threatening pattern from multiple data points simultaneously
Question 2
✅ Answer: C Rationale: SpO2 93% with visible accessory muscle use and tripod positioning (sitting upright) signals respiratory distress and impending failure. In children, respiratory failure precedes cardiac arrest. This requires immediate oxygen supplementation and reassessment. Fever and tachycardia (A, B) are expected with pneumonia. Poor intake (D) is important but secondary to the airway emergency. CT Skill tested: Discriminating most urgent from important findings; pediatric respiratory distress recognition
Question 3
✅ Answer: B Rationale: A blood glucose of 62 mg/dL with symptoms (shakiness) constitutes active hypoglycemia. Administering insulin would be dangerous and potentially fatal. The nurse's priority is to hold the insulin, treat with 15-20g fast-acting carbohydrate (Rule of 15), and notify the physician. Giving half a dose (C) is outside nursing scope. Waiting to recheck (D) delays treatment. CT Skill tested: Applying standards; differentiating safe from unsafe actions; questioning orders when evidence demands it
Question 4
✅ Answer: C Rationale: Acute onset confusion (new change from baseline) with normal vitals could indicate a stroke, sepsis, pulmonary embolism, or other emergency - many of which present before vital sign changes. Family is often the first to detect subtle changes. Immediate bedside assessment and neurological evaluation are required. Reassurance without assessment (A) is dangerous. Deferring documentation (B) delays care. CT Skill tested: Using family as a source of data; acting on subtle cues; recognizing that normal vitals do not rule out an emergency
Question 5
✅ Answer: B Rationale: These are classic signs of an acute hemolytic transfusion reaction (most dangerous type - ABO incompatibility). Immediate priorities: stop transfusion, keep IV access with NS (not the blood tubing), notify physician, check blood bag labels, and monitor for renal failure/shock. Slowing the rate (A) continues the harmful transfusion. Removing the IV (C) eliminates access for emergency treatment. Continuing (D) is life-threatening. CT Skill tested: Pattern recognition; emergency prioritization; safe transfusion management
Question 6
✅ Answer: C Rationale: The inability to demonstrate understanding reveals that teach-back has failed and the patient has not truly learned - nodding alone does not confirm comprehension. The nurse must assess for health literacy, language barriers, cognitive ability, or emotional readiness. A different approach (pictures, demonstration, return demonstration) should be used. Documenting false understanding (A) is dishonest and unsafe. Louder repetition (B) does not address the root cause. CT Skill tested: Evaluating credibility of information (teach-back); adapting patient education strategies
Question 7
✅ Answer: B Rationale: In COPD with chronic CO2 retention, patients rely on hypoxic drive (low O2 as the stimulus to breathe). Excessive oxygen can suppress this drive, cause hypercapnia, and lead to respiratory failure. The target SpO2 for COPD is 88-92%, not 95-100%. This is a teaching moment about disease-specific oxygen management. Answer C is partially correct but misses the educational opportunity. CT Skill tested: Applying disease-specific standards; teaching using clinical reasoning; differentiating general vs disease-specific norms
Question 8
✅ Answer: B Rationale: Acute drop in SpO2 from 96% to 89% in 30 minutes in an elderly pneumonia patient signals rapidly deteriorating oxygenation - the most immediately life-threatening change. This is a CHANGE from baseline, which always takes priority over stable abnormalities. Pain (A) is important but not life-threatening. Hyperglycemia at 210 (C) requires attention but is not an emergency. Discharge (D) is lowest acuity. CT Skill tested: Prioritization using acuity + change from baseline; applying ABC framework
Question 9
✅ Answer: B Rationale: Metformin must be held 48 hours before and after contrast CT due to risk of contrast-induced nephropathy leading to metformin-induced lactic acidosis (a life-threatening complication). Simply giving the drug because it is on the MAR (A) fails to apply clinical reasoning. The nurse must hold the dose, notify the physician, and get a clarification order. Documentation alone (C) is insufficient. Advising the patient to refuse a procedure (D) is outside nursing scope. CT Skill tested: Applying pharmacological standards; recognizing drug-procedure interactions; advocating for patient safety by questioning orders
Question 10
✅ Answer: B Rationale: The patient has primary post-partum hemorrhage (PPH) - the leading cause of maternal mortality. A boggy uterus indicates uterine atony (most common cause of PPH). Signs: hypotension, tachycardia, dizziness, heavy bleeding, boggy fundus. Immediate action: uterine massage to stimulate contraction, activate emergency response (call for help), establish large-bore IV access for fluid/blood products, and notify the obstetric team. Waiting (C, D) allows hemorrhage to progress to shock. CT Skill tested: Recognizing obstetric emergency patterns; acting on multiple simultaneous warning signs; prioritizing life-threatening maternal bleeding
Answer Key Summary
| Q | Answer | Topic |
|---|---|---|
| 1 | B | Post-op hypovolemic shock |
| 2 | C | Pediatric respiratory distress |
| 3 | B | Hypoglycemia + insulin safety |
| 4 | C | Acute onset confusion |
| 5 | B | Acute hemolytic transfusion reaction |
| 6 | C | Ineffective patient teaching |
| 7 | B | COPD oxygen management |
| 8 | B | Prioritization / triage |
| 9 | B | Metformin + contrast CT interaction |
| 10 | B | Post-partum hemorrhage |
Score interpretation: 9-10 correct = Strong clinical reasoning | 7-8 = Good foundation, review rationales | Below 7 = Focus on pathophysiology and priority-setting frameworks (ABCs, Maslow, change from baseline)