Radical neck dissection import aspects for Neet pg
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a high-yield, NEET PG-focused summary of Radical Neck Dissection (RND) based on Cummings Otolaryngology, Scott-Brown's, and Sabiston Surgery:
Radical Neck Dissection - NEET PG High-Yield Notes
1. Definition & What is Removed
RND = en bloc removal of ALL ipsilateral cervical lymph node-bearing tissue (Levels I-V) PLUS three non-lymphatic structures:
| Structure Removed | Consequence if Removed |
|---|---|
| Spinal Accessory Nerve (CN XI / SAN) | Shoulder drop, inability to abduct arm >90°, trapezius palsy |
| Internal Jugular Vein (IJV) | Facial/cerebral venous congestion; bilateral removal is dangerous (raised ICP) |
| Sternocleidomastoid Muscle (SCM) | Loss of neck contour, cosmetic deformity |
Boundaries of dissection:
- Superior: Inferior border of mandible
- Inferior: Clavicle
- Medial: Contralateral anterior belly of digastric + lateral border of strap muscles
- Posterior/lateral: Anterior border of trapezius
NOT removed in RND (important for MCQ): Postauricular/suboccipital nodes, perifacial nodes, retropharyngeal nodes, paratracheal nodes.
2. Classification of Neck Dissections (High-Yield Table)
| Type | Levels Removed | Structures Preserved |
|---|---|---|
| RND (Radical) | I-V | None - SAN, IJV, SCM all sacrificed |
| MRND (Modified Radical) | I-V | 1 or more of: SAN / IJV / SCM |
| SND (Selective) | Selective levels based on primary | All 3 non-lymphatic structures preserved |
| ERND (Extended Radical) | I-V + additional structures (e.g., level VII, hypoglossal nerve, carotid) | - |
MRND Types:
- Type I - SAN preserved (IJV and SCM removed)
- Type II - SAN + IJV preserved (SCM removed)
- Type III - SAN + IJV + SCM all preserved (= Functional neck dissection)
3. Indications for RND
- Extensive nodal metastases with extracapsular spread (ECS)
- Tumor directly infiltrating or fixed to SAN and/or IJV
- Not indicated for node-negative (N0) disease
MRND indication: Grossly visible lymph node disease NOT directly infiltrating non-lymphatic structures (SAN not involved).
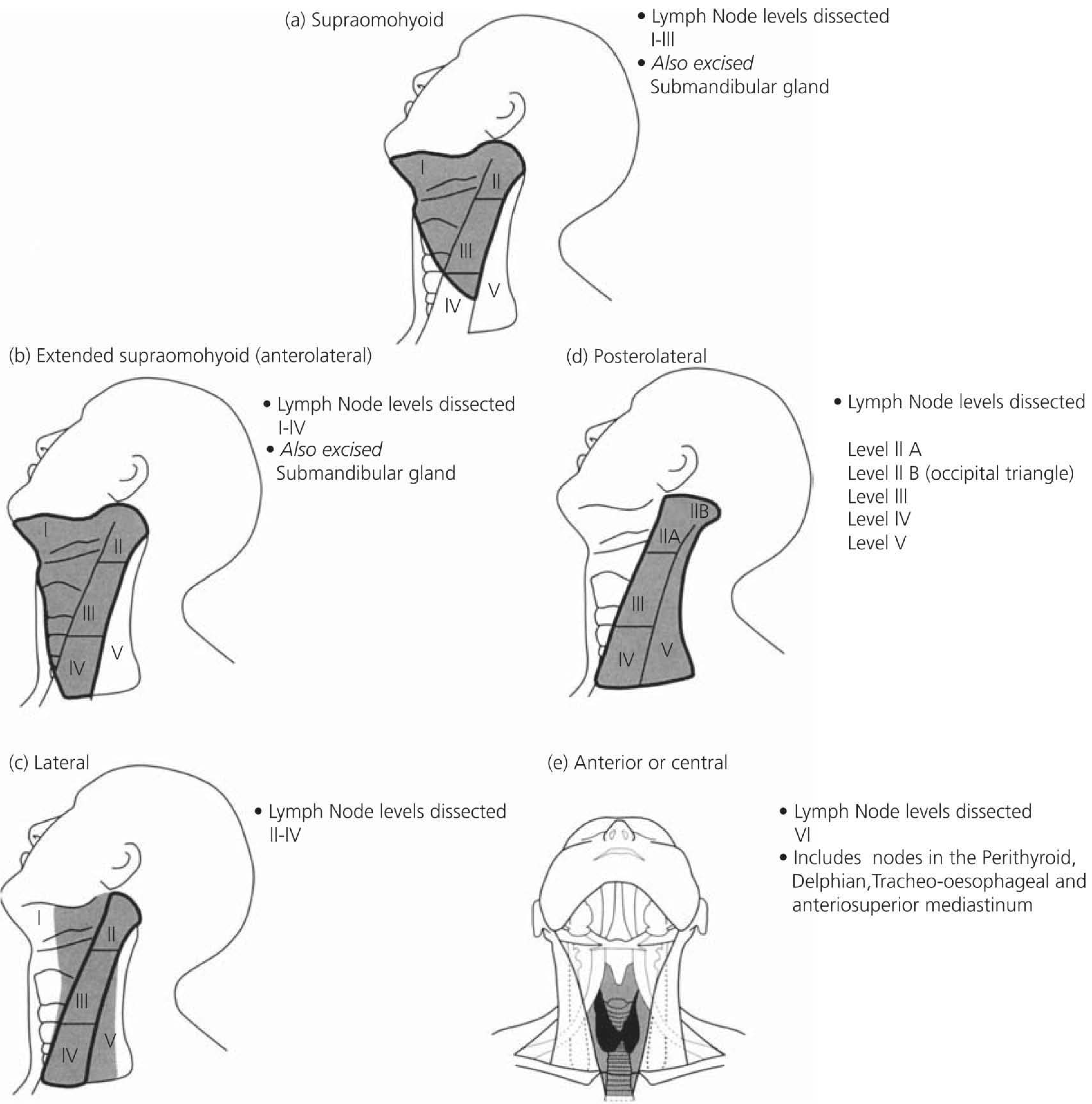
4. Selective Neck Dissection - Levels by Primary Site (High-Yield MCQ)
| Primary Site | SND Type | Levels Dissected |
|---|---|---|
| Oral cavity | Supraomohyoid | I, II, III |
| Oropharynx, Larynx, Hypopharynx | Lateral | II, III, IV |
| Thyroid / Larynx / Midline | Anterior/Central (paratracheal) | VI |
| Cutaneous/posterior scalp | Posterolateral | IIA, IIB, III, IV, V |
5. Neck Node Level Boundaries (NEET MCQ Favorite)
| Level | Name | Landmark |
|---|---|---|
| Ia | Submental | Between anterior bellies of digastric |
| Ib | Submandibular | Submandibular triangle |
| II | Upper Jugular | Skull base to hyoid |
| III | Mid Jugular | Hyoid to cricoid |
| IV | Lower Jugular | Cricoid to clavicle |
| V | Posterior Triangle | Behind SCM |
| VI | Central/Anterior | Between carotids, hyoid to sternum |
Important nodes:
- Jugulo-digastric node (level II) - "Tonsillar node" - first involved in oropharynx/oral cavity carcinoma
- Jugulo-omohyoid node (junction III/IV) - drains anterior tongue, floor of mouth
6. Complications of RND (High-Yield)
Most Important:
| Complication | Key Detail |
|---|---|
| Shoulder drop / Trapezius palsy | CN XI (SAN) sacrifice - most significant morbidity of RND |
| Chylous fistula | Left side more common; level IV dissection; 1.9-3% incidence; Rx: low-fat/medium-chain triglyceride diet, octreotide; surgery if >300 mL/day |
| Carotid artery blowout | Rare but life-threatening; risk factors: radiation, fistula, advanced disease; 50% mortality |
| Marginal mandibular nerve (CN VII branch) | Facial droop at corner of mouth; most common nerve injured in level I-II dissection |
| Greater auricular nerve | Sensory loss over parotid/posterior auricle; injured at Erb's point (exits posterior SCM at C2-C3) |
| Hemorrhage/Hematoma | Risk of airway compromise |
| Air leak | Most common early complication post-op |
| Raised ICP / facial edema | Bilateral simultaneous IJV sacrifice |
| Pneumothorax | Particularly with low-level IV dissection |
7. Key Anatomical Points for MCQs
- Erb's point: Junction of upper 1/3 and lower 2/3 of posterior SCM border - where SAN, great auricular nerve, lesser occipital nerve, transverse cervical, and supraclavicular nerves emerge
- SAN course: Exits jugular foramen → deep to digastric and stylohyoid → lateral/posterior to IJV → pierces SCM → exits at Erb's point → enters trapezius
- Thoracic duct: Opens at junction of left internal jugular vein and left subclavian vein - must be protected during left level IV dissection
- Hockey stick / Boomerang / McFee incisions - preferred incisions that avoid trifurcations overlying carotid sheath
8. Prognostic Factors (Post-RND)
- Extracapsular spread (ECS): Most important adverse prognostic factor
- Macroscopic ECS: 44% recurrence rate
- Microscopic ECS: 25% recurrence rate
- Number of nodes: 4+ positive nodes = dramatically worse 4-year survival
- Level of involvement: Multi-level positive nodes = 71% recurrence vs. 36.5% single level
- Adjuvant radiotherapy improves regional control significantly
9. One-Liners for Rapid Revision
- RND = Levels I-V + SAN + IJV + SCM removed
- Most significant morbidity of RND = Shoulder drop (SAN sacrifice)
- Most common nerve injured = Marginal mandibular branch of facial nerve
- Functional neck dissection = MRND Type III (all 3 structures preserved)
- Bilateral IJV sacrifice = risk of raised ICP and massive facial edema
- Chyle leak: Left-sided, level IV dissection, treat with medium-chain triglycerides and octreotide
- Jugulo-digastric node = "Tonsillar node" = 1st echelon for tonsil/oropharynx carcinoma
Sources: Cummings Otolaryngology Head and Neck Surgery; Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Sabiston Textbook of Surgery
Create a comparison chart: RND vs MRND vs SND with indications
Reading File
Reading File
Reading File
Reading File
Running Command
ls /home/daytona/workspace/ 2>/dev/null || mkdir -p /home/daytona/workspace/neck…
Running Command
mkdir -p /home/daytona/workspace/neck-dissection && ls /home/daytona/workspace/n…
Writing File
~/neck-dissection/chart.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_WIDE"; // 13.3" x 7.5"
pres.title = "Neck Dissection Comparison Chart";
// ─── COLOR PALETTE ───────────────────────────────────────────────
const C = {
bg: "0D1B2A", // Deep navy (dominant)
panel: "122236", // Slightly lighter navy for cards
rnd: "C0392B", // Bold red for RND
rndLight: "1A1010", // Dark red tint bg
mrnd: "E67E22", // Orange for MRND
mrndLight: "1A1308",
snd: "27AE60", // Green for SND
sndLight: "0C1A10",
gold: "F0C040", // Accent/highlight
white: "FFFFFF",
offWhite: "E8EDF3",
muted: "8FA3B8",
border: "1E3A5A",
};
// ═══════════════════════════════════════════════════════════════════
// SLIDE 1 - TITLE SLIDE
// ═══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.background = { color: C.bg };
// Top accent bar
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 13.3, h: 0.07, fill: { color: C.gold }, line: { color: C.gold } });
// Bottom accent bar
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 7.43, w: 13.3, h: 0.07, fill: { color: C.gold }, line: { color: C.gold } });
// Vertical accent bar
s.addShape(pres.shapes.RECTANGLE, { x: 0.5, y: 1.8, w: 0.08, h: 3.9, fill: { color: C.gold }, line: { color: C.gold } });
// Main title
s.addText("NECK DISSECTION", {
x: 0.8, y: 1.7, w: 11.5, h: 1.1,
fontSize: 52, bold: true, color: C.white,
fontFace: "Arial", charSpacing: 4, margin: 0,
});
// Subtitle
s.addText("RND vs MRND vs SND", {
x: 0.8, y: 2.9, w: 11, h: 0.7,
fontSize: 28, bold: false, color: C.gold,
fontFace: "Arial", charSpacing: 2, margin: 0,
});
// Tagline
s.addText("Comparison Chart with Indications — NEET PG Quick Reference", {
x: 0.8, y: 3.75, w: 10, h: 0.45,
fontSize: 14, color: C.muted, fontFace: "Arial", italic: true, margin: 0,
});
// Three colored pills for RND / MRND / SND
const pills = [
{ label: "RND", color: C.rnd, x: 0.8 },
{ label: "MRND", color: C.mrnd, x: 2.35 },
{ label: "SND", color: C.snd, x: 4.1 },
];
pills.forEach(p => {
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: p.x, y: 4.5, w: 1.35, h: 0.45,
fill: { color: p.color }, line: { color: p.color }, rectRadius: 0.08,
});
s.addText(p.label, {
x: p.x, y: 4.5, w: 1.35, h: 0.45,
fontSize: 13, bold: true, color: C.white,
align: "center", valign: "middle", margin: 0, fontFace: "Arial",
});
});
// Source note
s.addText("Source: Cummings Otolaryngology | Scott-Brown's | Sabiston Surgery", {
x: 0.8, y: 7.0, w: 11, h: 0.3,
fontSize: 9, color: C.muted, fontFace: "Arial", italic: true, margin: 0,
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 2 - MAIN COMPARISON TABLE (Wide)
// ═══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.background = { color: C.bg };
// Top bar
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 13.3, h: 0.07, fill: { color: C.gold }, line: { color: C.gold } });
// Slide title
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.07, w: 13.3, h: 0.65, fill: { color: C.panel }, line: { color: C.panel } });
s.addText("NECK DISSECTION — COMPARISON CHART", {
x: 0.2, y: 0.07, w: 13, h: 0.65,
fontSize: 16, bold: true, color: C.gold, fontFace: "Arial",
valign: "middle", charSpacing: 2, margin: 0,
});
// Table data
const hdr = { fill: { color: "1A3050" }, color: C.white, bold: true, fontSize: 10, fontFace: "Arial", align: "center", valign: "middle" };
const rndH = { fill: { color: C.rnd }, color: C.white, bold: true, fontSize: 11, fontFace: "Arial", align: "center", valign: "middle" };
const mrndH = { fill: { color: "B06010" }, color: C.white, bold: true, fontSize: 11, fontFace: "Arial", align: "center", valign: "middle" };
const sndH = { fill: { color: "1E7A44" }, color: C.white, bold: true, fontSize: 11, fontFace: "Arial", align: "center", valign: "middle" };
const rowStyle = (rndColor, mrndColor, sndColor) => [rndColor, mrndColor, sndColor];
const cell = (txt, clr, extraOpts = {}) => ({
text: txt,
options: {
fill: { color: clr },
color: C.offWhite,
fontSize: 9.5,
fontFace: "Arial",
valign: "middle",
align: "left",
margin: [3, 5, 3, 5],
...extraOpts,
}
});
const paramCell = (txt) => ({
text: txt,
options: {
fill: { color: "1A3050" },
color: C.gold,
fontSize: 9.5,
bold: true,
fontFace: "Arial",
valign: "middle",
align: "left",
margin: [3, 6, 3, 6],
}
});
const R = "161010"; // Dark red row bg
const O = "161008"; // Dark orange row bg
const G = "0C180E"; // Dark green row bg
const D = "0F1C2E"; // Default dark navy row
const tableRows = [
// Header row
[
{ text: "PARAMETER", options: { ...hdr, fill: { color: "0D2240" } } },
{ text: "RND\nRadical Neck Dissection", options: rndH },
{ text: "MRND\nModified Radical ND", options: mrndH },
{ text: "SND\nSelective Neck Dissection", options: sndH },
],
// Levels dissected
[
paramCell("Levels Dissected"),
cell("I – V (ALL levels)", R),
cell("I – V (ALL levels)", O),
cell("Specific levels based on primary site\n(e.g., I-III, II-IV, VI)", G),
],
// Non-lymphatic structures
[
paramCell("Non-Lymphatic\nStructures"),
cell("ALL THREE removed:\n• Spinal Accessory Nerve (SAN)\n• Internal Jugular Vein (IJV)\n• Sternocleidomastoid (SCM)", R),
cell("1 or more PRESERVED:\n• Type I: SAN preserved\n• Type II: SAN + IJV preserved\n• Type III: SAN + IJV + SCM\n (= Functional ND)", O),
cell("ALL THREE preserved:\n• SAN intact\n• IJV intact\n• SCM intact", G),
],
// Indications
[
paramCell("Indications"),
cell("• Extensive nodal metastases\n• Extracapsular spread (ECS)\n• Tumor fixed to / invading SAN or IJV\n• NOT for N0 disease", R),
cell("• Gross nodal disease NOT invading\n non-lymphatic structures\n• Multiple levels involved\n• Preferred over RND when SAN is free", O),
cell("• Clinically node-negative (N0) or early\n nodal disease at predictable levels\n• Based on primary tumor location\n• Same therapeutic value as RND/MRND\n for selected patients", G),
],
// Primary site mapping (SND specific)
[
paramCell("SND Subtypes by\nPrimary Site"),
cell("N/A", R, { align: "center" }),
cell("N/A", O, { align: "center" }),
cell("Oral cavity → Supraomohyoid (I-III)\nLarynx/Oropharynx/Hypopharynx → Lateral (II-IV)\nThyroid/Larynx/Midline → Anterior (VI)\nSkin/Scalp → Posterolateral (IIA, IIB, III, IV, V)", G),
],
// Morbidity
[
paramCell("Key Morbidity"),
cell("• Shoulder drop (trapezius palsy — SAN loss)\n• Facial/cerebral venous congestion (IJV loss)\n• Neck contour deformity (SCM loss)\n• Bilateral IJV: raised ICP!", R),
cell("• Reduced vs. RND\n• Shoulder morbidity if SAN sacrificed\n• Bilateral IJV loss: raised ICP\n (avoid simultaneous bilateral IJV sacrifice)", O),
cell("• Minimal — all 3 structures preserved\n• Residual disease risk if wrong levels\n selected\n• Often combined with adjuvant RT", G),
],
// Contraindications / not indicated
[
paramCell("NOT Indicated For"),
cell("• N0 (node-negative) disease\n• Nodes not fixed to non-lymphatic\n structures", R),
cell("• Nodes directly infiltrating/fixed\n to SAN or IJV\n (→ upgrade to RND)", O),
cell("• Extensive multinodal disease\n• ECS present\n• Not for nodes fixed to non-\n lymphatic structures", G),
],
// Recurrence rates
[
paramCell("Regional Recurrence\nRate (Therapeutic)"),
cell("Varies by ECS:\n• Macro ECS: ~44%\n• Micro ECS: ~25%\n• Multi-level +nodes: 71%", R),
cell("0 – 20%\n(with/without adjuvant RT)", O),
cell("N0 neck: 4–6%\nN+ (single node, no ECS): ~10%\nN+ (multiple/ECS): ~24%\n→ Adjuvant RT reduces to ~15%", G),
],
];
s.addTable(tableRows, {
x: 0.15, y: 0.78,
w: 12.95,
colW: [1.85, 3.65, 3.65, 3.8],
rowH: [0.42, 0.32, 0.85, 0.85, 0.78, 0.78, 0.55, 0.7],
border: { type: "solid", pt: 0.5, color: C.border },
});
// Bottom source
s.addText("Cummings Otolaryngology | Scott-Brown's Otorhinolaryngology | Sabiston Surgery", {
x: 0.2, y: 7.3, w: 12.9, h: 0.18,
fontSize: 7.5, color: C.muted, fontFace: "Arial", italic: true, margin: 0,
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 3 - INDICATIONS DEEP DIVE (3 COLUMNS)
// ═══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.background = { color: C.bg };
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 13.3, h: 0.07, fill: { color: C.gold }, line: { color: C.gold } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.07, w: 13.3, h: 0.6, fill: { color: C.panel }, line: { color: C.panel } });
s.addText("INDICATIONS — DETAILED BREAKDOWN", {
x: 0.2, y: 0.07, w: 13, h: 0.6,
fontSize: 16, bold: true, color: C.gold, fontFace: "Arial", valign: "middle", charSpacing: 2, margin: 0,
});
const cards = [
{
title: "RND – Radical Neck Dissection",
color: C.rnd,
darkBg: "1A0A08",
x: 0.15,
sections: [
{
heading: "Primary Indication",
body: "Extensive cervical lymph node metastases with EXTRACAPSULAR SPREAD (ECS) — the #1 indication",
},
{
heading: "Specific Criteria",
bullets: [
"Tumor directly invading or fixed to SAN (CN XI)",
"Tumor invading or encasing the Internal Jugular Vein",
"Multiple matted nodes across several levels",
"Salvage surgery after failed RT/CRT",
"Extended RND: + skin, hypoglossal nerve, carotid",
],
},
{
heading: "NOT Indicated",
bullets: [
"N0 (clinically node-negative) disease",
"Nodes not fixed to non-lymphatic structures",
],
},
{
heading: "Prognostic Note",
body: "ECS is the strongest prognostic factor. Macroscopic ECS → 44% recurrence. Adjuvant RT strongly recommended post-RND.",
},
],
},
{
title: "MRND – Modified Radical ND",
color: C.mrnd,
darkBg: "1A1005",
x: 4.55,
sections: [
{
heading: "Primary Indication",
body: "Grossly visible multilevel nodal disease NOT directly infiltrating or fixed to non-lymphatic structures (SAN, IJV, SCM)",
},
{
heading: "Types & When",
bullets: [
"Type I (SAN preserved): SAN not involved, IJV/SCM invaded",
"Type II (SAN+IJV preserved): IJV uninvolved but SCM invaded",
"Type III / Functional ND: all 3 structures free — best functional outcome",
"Sacrifice of 1-2 structures allowed if grossly invaded intraop",
],
},
{
heading: "Key Point",
body: "Cannot justify sacrificing SAN if it is not involved, since hypoglossal + vagus nerves (in equal proximity) are routinely spared.",
},
{
heading: "Bilateral Caution",
body: "Simultaneous bilateral IJV sacrifice = severe facial edema + raised ICP. Avoid or stage procedures.",
},
],
},
{
title: "SND – Selective Neck Dissection",
color: C.snd,
darkBg: "081508",
x: 8.95,
sections: [
{
heading: "Primary Indication",
body: "Patients at risk for EARLY / predictable lymph node metastases based on primary tumor site",
},
{
heading: "Level Selection by Site",
bullets: [
"Oral cavity → I, II, III (Supraomohyoid)",
"Oropharynx / Larynx / Hypopharynx → II, III, IV (Lateral)",
"Thyroid / Trachea / Larynx (midline) → VI (Anterior/Central)",
"Posterior scalp / Cutaneous → IIA, IIB, III, IV, V (Posterolateral)",
],
},
{
heading: "Basis (Shah's Study)",
body: "Oral cavity mets → Levels I-III. Pharynx/larynx → Levels II-IV. When positive nodes found outside these — disease also present in the at-risk zone.",
},
{
heading: "Equivalent Efficacy",
body: "Studies show SND has same therapeutic value as RND/MRND for selected patients. Combined with adjuvant RT for N+ disease.",
},
],
},
];
cards.forEach(card => {
const cw = 4.2;
// Card background
s.addShape(pres.shapes.RECTANGLE, {
x: card.x, y: 0.75, w: cw, h: 6.55,
fill: { color: card.darkBg }, line: { color: card.color, pt: 1.5 },
});
// Header band
s.addShape(pres.shapes.RECTANGLE, {
x: card.x, y: 0.75, w: cw, h: 0.45,
fill: { color: card.color }, line: { color: card.color },
});
s.addText(card.title, {
x: card.x, y: 0.75, w: cw, h: 0.45,
fontSize: 11, bold: true, color: C.white, fontFace: "Arial",
align: "center", valign: "middle", margin: 0,
});
let yPos = 1.28;
card.sections.forEach(sec => {
// Section heading
s.addText(sec.heading, {
x: card.x + 0.1, y: yPos, w: cw - 0.2, h: 0.25,
fontSize: 9.5, bold: true, color: card.color, fontFace: "Arial",
valign: "middle", margin: 0,
});
yPos += 0.25;
if (sec.body) {
s.addText(sec.body, {
x: card.x + 0.12, y: yPos, w: cw - 0.24, h: 0.52,
fontSize: 8.5, color: C.offWhite, fontFace: "Arial",
valign: "top", wrap: true, margin: 0,
});
yPos += 0.57;
}
if (sec.bullets) {
const bulletItems = sec.bullets.map((b, i) => ({
text: b,
options: {
bullet: { indent: 12 },
breakLine: i < sec.bullets.length - 1,
fontSize: 8.5,
color: C.offWhite,
fontFace: "Arial",
},
}));
s.addText(bulletItems, {
x: card.x + 0.12, y: yPos, w: cw - 0.24, h: sec.bullets.length * 0.28,
valign: "top", margin: 0, wrap: true,
});
yPos += sec.bullets.length * 0.285 + 0.05;
}
yPos += 0.08; // spacing between sections
});
});
s.addText("Cummings Otolaryngology | Scott-Brown's | Sabiston Surgery", {
x: 0.2, y: 7.35, w: 12.9, h: 0.15,
fontSize: 7.5, color: C.muted, fontFace: "Arial", italic: true, margin: 0,
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 4 - COMPLICATIONS + QUICK MEMORY AIDS
// ═══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.background = { color: C.bg };
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 13.3, h: 0.07, fill: { color: C.gold }, line: { color: C.gold } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.07, w: 13.3, h: 0.58, fill: { color: C.panel }, line: { color: C.panel } });
s.addText("COMPLICATIONS & NEET PG MEMORY AIDS", {
x: 0.2, y: 0.07, w: 13, h: 0.58,
fontSize: 16, bold: true, color: C.gold, fontFace: "Arial", valign: "middle", charSpacing: 2, margin: 0,
});
// ── COMPLICATIONS TABLE (left 60%) ──
s.addText("KEY COMPLICATIONS OF NECK DISSECTION", {
x: 0.15, y: 0.73, w: 7.8, h: 0.3,
fontSize: 10.5, bold: true, color: C.gold, fontFace: "Arial", margin: 0,
});
const compRows = [
[
{ text: "Complication", options: { fill: { color: "1A3050" }, color: C.white, bold: true, fontSize: 9, fontFace: "Arial", align: "center", valign: "middle" } },
{ text: "Details / Key Fact", options: { fill: { color: "1A3050" }, color: C.white, bold: true, fontSize: 9, fontFace: "Arial", align: "center", valign: "middle" } },
{ text: "Rx", options: { fill: { color: "1A3050" }, color: C.white, bold: true, fontSize: 9, fontFace: "Arial", align: "center", valign: "middle" } },
],
[
{ text: "⚠ Shoulder Drop\n(Trapezius palsy)", options: { fill: { color: "200808" }, color: C.rnd, bold: true, fontSize: 8.5, fontFace: "Arial", valign: "middle" } },
{ text: "SAN (CN XI) sacrifice in RND. #1 morbidity. Cannot abduct arm >90°", options: { fill: { color: "1A1010" }, color: C.offWhite, fontSize: 8.5, fontFace: "Arial", valign: "middle" } },
{ text: "Physiotherapy", options: { fill: { color: "141010" }, color: C.muted, fontSize: 8.5, fontFace: "Arial", valign: "middle", align: "center" } },
],
[
{ text: "Chylous Fistula", options: { fill: { color: "141A10" }, color: C.snd, bold: true, fontSize: 8.5, fontFace: "Arial", valign: "middle" } },
{ text: "Level IV dissection. Left side >> Right. ~1.9–3% incidence. Thoracic duct injury", options: { fill: { color: "0F1A0F" }, color: C.offWhite, fontSize: 8.5, fontFace: "Arial", valign: "middle" } },
{ text: "MCT diet, octreotide; surgery if >300 mL/day", options: { fill: { color: "0C1510" }, color: C.muted, fontSize: 8.5, fontFace: "Arial", valign: "middle" } },
],
[
{ text: "Marginal Mandibular\nNerve Injury", options: { fill: { color: "12180A" }, color: C.mrnd, bold: true, fontSize: 8.5, fontFace: "Arial", valign: "middle" } },
{ text: "Most common nerve injured. Facial droop at corner of mouth. Level I-II dissection", options: { fill: { color: "141808" }, color: C.offWhite, fontSize: 8.5, fontFace: "Arial", valign: "middle" } },
{ text: "Observation; often temporary", options: { fill: { color: "101408" }, color: C.muted, fontSize: 8.5, fontFace: "Arial", valign: "middle" } },
],
[
{ text: "Greater Auricular\nNerve Injury", options: { fill: { color: "141418" }, color: "A0A0D0", bold: true, fontSize: 8.5, fontFace: "Arial", valign: "middle" } },
{ text: "C2-C3 origin; exits at Erb's point. Sensory loss over parotid/ear. Up to 36% temp injury rate", options: { fill: { color: "0F1018" }, color: C.offWhite, fontSize: 8.5, fontFace: "Arial", valign: "middle" } },
{ text: "Usually temporary", options: { fill: { color: "0C0E15" }, color: C.muted, fontSize: 8.5, fontFace: "Arial", valign: "middle" } },
],
[
{ text: "Carotid Artery\nBlowout (CBS)", options: { fill: { color: "200808" }, color: C.rnd, bold: true, fontSize: 8.5, fontFace: "Arial", valign: "middle" } },
{ text: "RARE but FATAL. Risk: prior RT, fistula, advanced disease. 50% mortality. Proximal to bifurcation", options: { fill: { color: "1A0808" }, color: C.offWhite, fontSize: 8.5, fontFace: "Arial", valign: "middle" } },
{ text: "Endovascular embolization/stenting; emergency surgery", options: { fill: { color: "150808" }, color: C.muted, fontSize: 8.5, fontFace: "Arial", valign: "middle" } },
],
[
{ text: "Bilateral IJV Sacrifice", options: { fill: { color: "200808" }, color: C.rnd, bold: true, fontSize: 8.5, fontFace: "Arial", valign: "middle" } },
{ text: "Massive facial edema + raised ICP. AVOID simultaneous bilateral IJV ligation", options: { fill: { color: "1A0808" }, color: C.offWhite, fontSize: 8.5, fontFace: "Arial", valign: "middle" } },
{ text: "Stage procedures; consider MRND to preserve 1 IJV", options: { fill: { color: "150808" }, color: C.muted, fontSize: 8.5, fontFace: "Arial", valign: "middle" } },
],
];
s.addTable(compRows, {
x: 0.15, y: 1.08,
w: 7.85,
colW: [2.1, 3.6, 2.15],
rowH: [0.3, 0.45, 0.48, 0.45, 0.48, 0.48, 0.45],
border: { type: "solid", pt: 0.5, color: C.border },
});
// ── RIGHT COLUMN: MEMORY AIDS ──
const rx = 8.3;
s.addText("NEET PG ONE-LINERS", {
x: rx, y: 0.73, w: 4.85, h: 0.3,
fontSize: 10.5, bold: true, color: C.gold, fontFace: "Arial", margin: 0,
});
const oneLinersBg = "0F1E30";
s.addShape(pres.shapes.RECTANGLE, {
x: rx, y: 1.08, w: 4.85, h: 2.88,
fill: { color: oneLinersBg }, line: { color: C.border, pt: 1 },
});
const oneLiners = [
["RND =", "Levels I-V + SAN + IJV + SCM ALL removed"],
["#1 morbidity of RND =", "Shoulder drop (SAN sacrifice)"],
["Most common nerve injured =", "Marginal mandibular branch (CN VII)"],
["Functional ND =", "MRND Type III (all 3 structures preserved)"],
["Bilateral IJV sacrifice →", "Raised ICP + massive facial edema"],
["Chyle leak side =", "Left >> Right (thoracic duct)"],
["Chyle leak Rx >300 mL/day =", "Surgical ligation"],
["Jugulo-digastric node =", "Tonsillar node (Level II)"],
["Oral cavity SND =", "Supraomohyoid (I-III)"],
["Larynx/Oropharynx SND =", "Lateral (II-IV)"],
];
oneLiners.forEach((line, i) => {
const yy = 1.13 + i * 0.272;
s.addText([
{ text: line[0] + " ", options: { bold: true, color: C.gold, fontSize: 8.5 } },
{ text: line[1], options: { bold: false, color: C.offWhite, fontSize: 8.5 } },
], {
x: rx + 0.12, y: yy, w: 4.6, h: 0.26,
fontFace: "Arial", valign: "middle", margin: 0, wrap: true,
});
});
// ERB'S POINT BOX
s.addShape(pres.shapes.RECTANGLE, {
x: rx, y: 4.03, w: 4.85, h: 1.55,
fill: { color: "0A1A28" }, line: { color: C.gold, pt: 1.2 },
});
s.addText("ERB'S POINT — Key Anatomy", {
x: rx + 0.08, y: 4.08, w: 4.7, h: 0.28,
fontSize: 9.5, bold: true, color: C.gold, fontFace: "Arial", margin: 0,
});
s.addText([
{ text: "Location: ", options: { bold: true, color: C.mrnd } },
{ text: "Junction of upper 1/3 & lower 2/3 of posterior SCM border\n", options: { color: C.offWhite } },
{ text: "Nerves emerging at Erb's Point:\n", options: { bold: true, color: C.mrnd } },
{ text: "• Spinal Accessory Nerve (SAN / CN XI)\n• Greater Auricular Nerve (C2-C3)\n• Lesser Occipital Nerve\n• Transverse Cervical Nerve\n• Supraclavicular Nerve", options: { color: C.offWhite } },
], {
x: rx + 0.1, y: 4.38, w: 4.68, h: 1.15,
fontSize: 8.5, fontFace: "Arial", valign: "top", wrap: true, margin: 0,
});
// THORACIC DUCT BOX
s.addShape(pres.shapes.RECTANGLE, {
x: rx, y: 5.65, w: 4.85, h: 0.9,
fill: { color: "0A1A10" }, line: { color: C.snd, pt: 1.2 },
});
s.addText("THORACIC DUCT — Key Point", {
x: rx + 0.08, y: 5.68, w: 4.7, h: 0.25,
fontSize: 9.5, bold: true, color: C.snd, fontFace: "Arial", margin: 0,
});
s.addText("Opens at junction of LEFT internal jugular vein + LEFT subclavian vein.\nMust be protected during LEFT Level IV neck dissection.\nRight-sided equivalent (right lymphatic duct) is smaller but also at risk.", {
x: rx + 0.1, y: 5.95, w: 4.68, h: 0.58,
fontSize: 8.5, color: C.offWhite, fontFace: "Arial", valign: "top", wrap: true, margin: 0,
});
s.addText("Cummings Otolaryngology | Scott-Brown's | Sabiston Surgery", {
x: 0.2, y: 7.35, w: 12.9, h: 0.15,
fontSize: 7.5, color: C.muted, fontFace: "Arial", italic: true, margin: 0,
});
}
// ═══════════════════════════════════════════════════════════════════
// WRITE FILE
// ═══════════════════════════════════════════════════════════════════
pres.writeFile({ fileName: "/home/daytona/workspace/neck-dissection/RND_vs_MRND_vs_SND.pptx" })
.then(() => console.log("✅ PPTX written successfully"))
.catch(e => console.error("❌ Error:", e));
Running Command
cd /home/daytona/workspace/neck-dissection && node chart.js 2>&1
Your comparison chart is ready!
RND vs MRND vs SND
Presentation · PPTX
The file is a 4-slide NEET PG reference deck in a dark navy/clinical color scheme:
| Slide | Content |
|---|---|
| Slide 1 | Title slide with color-coded pills for RND (red), MRND (orange), SND (green) |
| Slide 2 | Main comparison table - Levels, structures, indications, SND subtypes by primary site, morbidity, contraindications, and recurrence rates side by side |
| Slide 3 | Indications deep dive - 3 detailed column cards, one per dissection type, with specific criteria, types, key points, and Shah's level-mapping study |
| Slide 4 | Complications table + NEET PG one-liners + Erb's Point anatomy box + Thoracic duct key point |
This is a shared conversation. Sign in to Orris to start your own chat.