Give me perfect viva questions and answers detailed for panophthalmitis case ophthalmology
Reading File
Finding Sources
Finding Sources
Searching PubMed
panophthalmitis endophthalmitis management
Reading File
Finding Sources
Finding Sources
Searching PubMed
panophthalmitis endophthalmitis intravitreal antibiotics treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
I now have comprehensive data from multiple authoritative textbooks. Let me compile the complete viva Q&A.
Panophthalmitis - Complete Viva Questions & Answers
Sources: Robbins & Cotran Pathologic Basis of Disease, Wills Eye Manual (9e), Harrison's Principles of Internal Medicine (22e), Kanski's Clinical Ophthalmology (10e), Tintinalli's Emergency Medicine, Tietz Laboratory Medicine
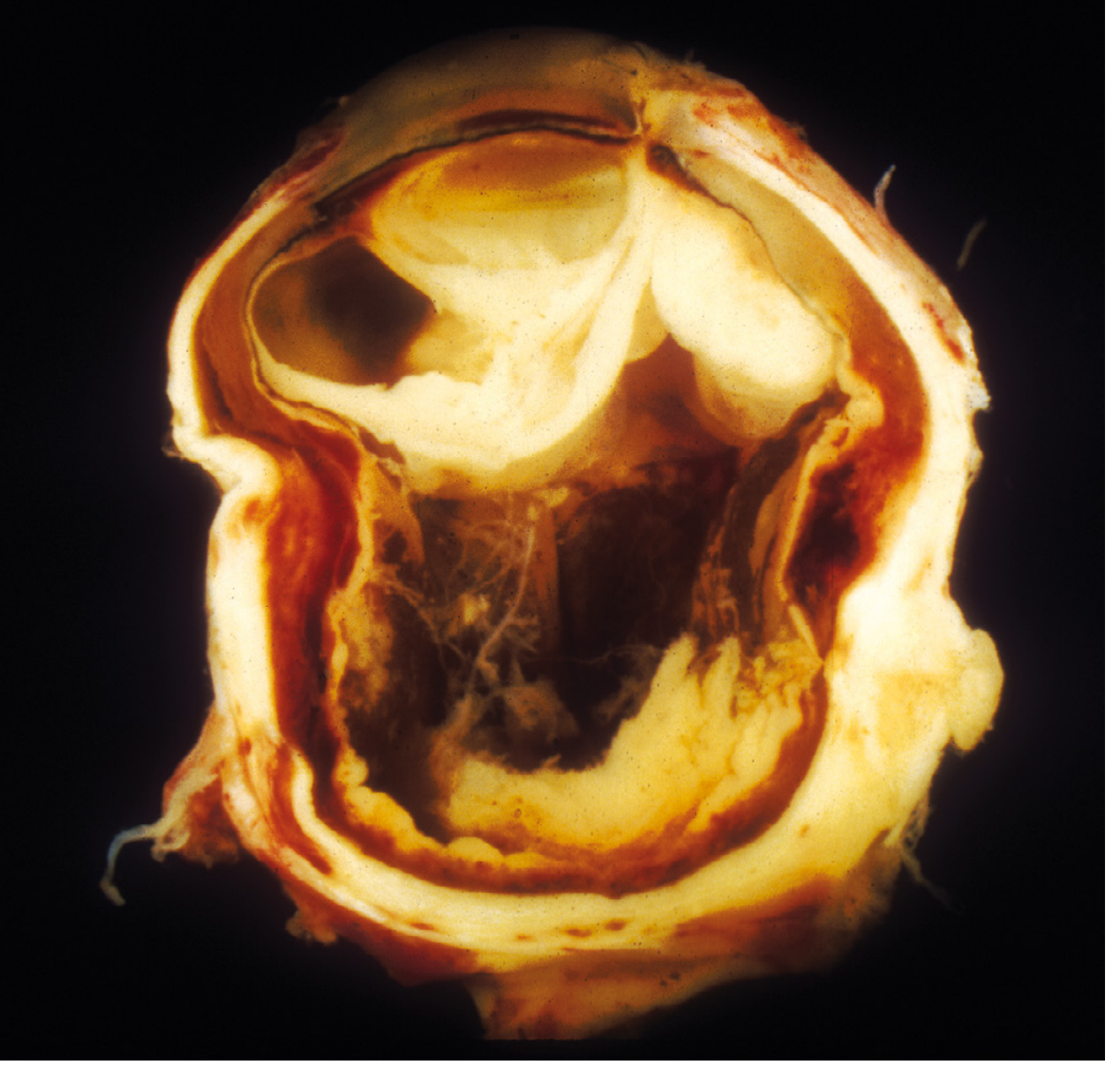
Fig: Exogenous panophthalmitis. Eye removed after foreign body injury. Suppurative inflammation of the entire orbit has distorted all internal architecture. (Robbins & Cotran, p.1216)
Q1. Define panophthalmitis and distinguish it from endophthalmitis.
Answer:
- Endophthalmitis is inflammation of the interior of the eye involving the vitreous humor. It does not extend beyond the sclera.
- Panophthalmitis is inflammation of the entire eye - the interior (vitreous, retina, choroid) plus the sclera, extending into the orbit (peri-ocular tissues).
The key distinction: panophthalmitis is endophthalmitis that has "broken out" through the scleral coat and involves periorbital structures. It is therefore the most severe and destructive form of intraocular infection.
- Robbins & Cotran Pathologic Basis of Disease, p.1216
Q2. How is panophthalmitis / endophthalmitis classified?
Answer:
By source of infection:
| Type | Definition | Common causes |
|---|---|---|
| Exogenous | Organism gains access through an external wound | Post-surgical (cataract, vitrectomy, intravitreal injection), penetrating trauma, IOFB, corneal ulcer extension |
| Endogenous | Organism delivered hematogenously from within the body | Septicemia, bacteremia, fungemia (IV drug use, immunocompromised states, hepatobiliary infections) |
Panophthalmitis typically results from untreated or rapidly progressive exogenous endophthalmitis, or from very virulent organisms in endogenous disease (e.g., Klebsiella pneumoniae, Pseudomonas aeruginosa).
- Robbins & Cotran, p.1216; Wills Eye Manual
Q3. What are the common causative organisms in panophthalmitis?
Answer:
Post-surgical (most common overall):
- Staphylococcus epidermidis - most common post-cataract
- Staphylococcus aureus
- Streptococcal species
- Gram-negative organisms: Pseudomonas, Klebsiella, Proteus, Enterobacter, E. coli, Haemophilus influenzae
- Anaerobes (less common)
Post-traumatic / penetrating injury:
- Staphylococcus, Streptococcus, Bacillus cereus (highly virulent - associated with soil/organic matter contamination)
- Fungal species (especially with organic matter - soil, vegetable matter)
- Mixed flora
Endogenous (hematogenous):
- Klebsiella pneumoniae (invasive syndrome - especially in East Asia, associated with liver abscess)
- Pseudomonas aeruginosa - causes a fulminant panophthalmitis; severe pain, chemosis, anterior uveitis, vitreous involvement
- Candida species - especially in IV drug users or systemic candidemia
- Bacillus cereus (rare, very destructive)
Bleb-associated: Streptococcus or Gram-negative organisms.
Examiner tip: Bacillus cereus is notorious for causing rapidly destructive panophthalmitis within 12-24 hours of penetrating trauma, especially from soil-contaminated injuries.
- Wills Eye Manual; Harrison's Principles of Internal Medicine 22e, p.CNS Infections chapter
Q4. Describe the clinical features (symptoms and signs) of panophthalmitis.
Answer:
Symptoms:
- Severe, deep ocular pain (cardinal feature - more severe than endophthalmitis alone)
- Drastically decreased visual acuity (may be light perception or no light perception)
- Photophobia
- Fever, malaise (especially in endogenous cases)
Signs (anterior segment):
- Eyelid edema and erythema
- Marked conjunctival chemosis and injection
- Corneal edema, corneal ring ulcer (characteristic of virulent gram-negative organisms)
- Hypopyon (pus in anterior chamber)
- Absent red reflex
- Iris microabscesses
Signs (posterior segment):
- Dense vitritis
- Retinal inflammatory infiltrates
- Flame-shaped retinal hemorrhages ± white centers (Roth spots)
- Retinal/subretinal/choroidal abscesses
Signs indicating extension beyond globe (panophthalmitis specifically):
- Proptosis
- Restricted extraocular movements
- Periorbital edema and erythema
- Leukocytosis
With Pseudomonas specifically: fulminant course with severe pain, chemosis, decreased visual acuity, anterior uveitis, vitreous involvement, and panophthalmitis - Harrison's describes this as "the most devastating of P. aeruginosa eye infections."
- Wills Eye Manual; Harrison's 22e; Robbins & Cotran, p.1216
Q5. What investigations would you order in a suspected case of panophthalmitis?
Answer:
Ocular investigations:
- B-scan ultrasonography - to assess posterior segment when view is limited; confirms vitritis, membranes, choroidal thickening, retinal detachment; establishes baseline for treatment response
- Anterior chamber paracentesis (0.2 mL) - for Gram stain, culture (blood, chocolate, Sabouraud, thioglycolate media), and sensitivities
- Vitreous tap / diagnostic vitrectomy - more sensitive than AC tap; mandatory if visual acuity is light perception or worse
- CT orbit (axial, coronal, parasagittal views with 1-mm cuts) - especially in traumatic cases to rule out intraocular foreign body (IOFB), assess orbital extension, detect gas-forming organisms
Systemic investigations (especially in endogenous panophthalmitis):
- Blood cultures (aerobic and anaerobic) × 2 sets
- Complete blood count with differential (leukocytosis expected)
- Blood glucose, HbA1c (diabetes is a major risk factor for Klebsiella endogenous panophthalmitis)
- Liver function tests + abdominal ultrasound/CT (Klebsiella liver abscess as primary source)
- Echocardiogram if endocarditis suspected
- Chest X-ray (pulmonary source for hematogenous spread)
- Infectious disease consult
Culture media for intraocular specimens:
- Blood agar (aerobic bacteria)
- Chocolate agar (fastidious organisms, Haemophilus)
- Sabouraud dextrose agar (fungi)
- Thioglycolate broth (anaerobes)
- Gram and Giemsa stains on smears
- Wills Eye Manual; Tintinalli's Emergency Medicine
Q6. What is the treatment of panophthalmitis? Give specific drug names and doses.
Answer:
Treatment is aggressive, multidisciplinary, and time-critical. Every hour of delay risks irreversible retinal damage.
Step 1: Hospitalization
- Mandatory - patient requires IV antibiotics, close monitoring q12-24h
Step 2: Cultures before antibiotics
- AC tap / vitreous tap for Gram stain, culture, sensitivity
Step 3: Intravitreal antibiotics (most important step)
Broad-spectrum coverage - given as two injections simultaneously:
| Drug | Dose | Coverage |
|---|---|---|
| Vancomycin | 1 mg in 0.1 mL | Gram-positive (MRSA, Staph) |
| Ceftazidime | 2.2 mg in 0.1 mL | Gram-negative |
| Amikacin 0.4 mg in 0.1 mL OR Clindamycin 1 mg in 0.1 mL | alternative | Gram-negative / Bacillus / anaerobes (if penicillin allergy or IOFB) |
Caution: Aminoglycosides (amikacin) carry risk of macular infarction - use cautiously. Repeat intravitreal antibiotics every 48-72 hours as needed.
For fungal panophthalmitis: intravitreal voriconazole or amphotericin B
Step 4: Systemic (IV/oral) antibiotics
- Ciprofloxacin 400 mg IV q12h OR Moxifloxacin 400 mg PO/IV daily
- Cefazolin 1 g IV q8h
- Fluoroquinolones (moxifloxacin) achieve therapeutic vitreous levels - an advantage over many other systemic antibiotics
- Adjust for renal function and pediatric dosing
Step 5: Topical therapy
- Fortified antibiotics: Vancomycin + tobramycin q1h (around the clock for 24-48 hours) - especially if bleb, wound leak, or exposed sutures
- Atropine 1% b.i.d.-t.i.d. (cycloplegia, pain relief, prevents synechiae)
- Topical steroids (prednisolone acetate 1% q1h) - for anterior segment inflammation
Step 6: Intravitreal corticosteroids
- Dexamethasone 0.4 mg/0.1 mL - considered in severe vitreous inflammation (reduces secondary inflammatory damage)
Step 7: Pars plana vitrectomy (PPV)
- Definitive indication: Visual acuity = light perception or worse (post-cataract endophthalmitis - from EVS trial data)
- PPV reduces infectious burden, obtains material for culture, removes inflammatory mediators
- In traumatic cases: removes IOFB (paramount for infection control) and inflammatory debris
- Benefit in non-surgical endophthalmitis cases is less defined but generally recommended in panophthalmitis
Step 8: Removal of IOFB (in traumatic panophthalmitis)
- Paramount - retained foreign bodies perpetuate infection
Step 9: Tetanus prophylaxis
- Tetanus toxoid 0.5 mL IM if immunization not up to date (traumatic cases)
Step 10: Evisceration / Enucleation
- When the eye is irretrievably lost, severely painful, and there is risk to the contralateral eye (sympathetic ophthalmia) or life
- Evisceration: removal of intraocular contents, scleral coat preserved - preferred for infection control, faster, lower risk of meningitis spread in some settings
- Enucleation: removal of entire globe - indicated if tumor is suspected or optic nerve involvement
- Wills Eye Manual; Harrison's 22e; Tietz Lab Medicine, p.EYE INFECTIONS; Miller's Anesthesia
Q7. What is the Endophthalmitis Vitrectomy Study (EVS) and what did it show?
Answer:
The EVS (1995) was a landmark RCT that studied management of acute post-cataract-surgery endophthalmitis. Key findings:
- Immediate PPV is beneficial when visual acuity is light perception or worse - patients with LP or worse VA who underwent PPV had a 3-fold better chance of achieving 20/40 or better vision compared to vitreous tap alone.
- Systemic antibiotics (IV amikacin + cefazolin) provided NO additional benefit over intravitreal antibiotics alone in post-cataract endophthalmitis.
- Subconjunctival antibiotics were used in the original protocol but are now rarely used.
Important limitation: The EVS specifically studied post-cataract endophthalmitis. Its results do NOT directly apply to post-traumatic, bleb-related, or endogenous panophthalmitis - systemic antibiotics may still be important in those scenarios.
- Wills Eye Manual
Q8. What is the difference between evisceration and enucleation? When is each done in panophthalmitis?
Answer:
| Feature | Evisceration | Enucleation |
|---|---|---|
| Definition | Removal of intraocular contents; scleral shell and extraocular muscles preserved | Removal of entire globe including sclera |
| Orbital contents | EOM, orbital fat, bone preserved | EOM preserved, fat preserved |
| Indications | Blind, painful eye; panophthalmitis (most preferred); phthisis bulbi | Suspected intraocular tumor; risk of sympathetic ophthalmia; optic nerve disease; when evisceration technically not possible |
| Advantages | Better cosmetic result; lower anesthesia risk; preserves natural socket anatomy | Eliminates risk of sympathetic ophthalmia completely |
| Contraindication | Suspected malignancy | - |
In panophthalmitis, evisceration is generally preferred because:
- Faster procedure
- Better cosmesis (scleral shell preserved)
- Direct access to infected contents for drainage/culture
- Reduces septic focus
Exenteration (removal of all orbital contents including globe, fat, muscles) is reserved for orbital extension or malignancy.
- Miller's Anesthesia, 10e; Tietz Lab Medicine
Q9. What organisms cause endogenous panophthalmitis, and what systemic conditions predispose to it?
Answer:
Organisms:
- Klebsiella pneumoniae - invasive syndrome: liver abscess → hematogenous spread to eye; classically in diabetic East Asian patients; [associated with 6-year Chinese study showing high mortality - PMID 34280072]
- Pseudomonas aeruginosa - fulminant; described in bacteremia; also linked to contaminated artificial tears (carbapenem-resistant strains causing outbreaks in the USA per Harrison's 22e)
- Candida albicans / tropicalis - IV drug users, systemic candidemia, TPN patients, immunocompromised
- Aspergillus - immunocompromised, post-transplant
- Bacillus cereus - post-traumatic / IV drug use
- Streptococcus pneumoniae, S. aureus - from pulmonary or skin source
Predisposing systemic conditions:
- Diabetes mellitus (most important risk factor for Klebsiella)
- Immunosuppression (HIV/AIDS, transplant, chemotherapy)
- IV drug use (fungal/bacterial)
- Infective endocarditis
- Meningitis (Neisseria meningitidis)
- Septicemia
- Pulmonary infections
- Hepatobiliary disease (Klebsiella liver abscess)
- Total parenteral nutrition (Candida)
- Robbins & Cotran, p.1216; Harrison's 22e; Wills Eye Manual
Q10. What are the differentials of panophthalmitis?
Answer:
| Condition | Distinguishing features |
|---|---|
| TASS (Toxic Anterior Segment Syndrome) | Occurs 6-24 hours post-surgery; diffuse corneal edema; NO vitritis; responds to topical steroids; sterile |
| Sterile (aseptic) endophthalmitis | Follows intravitreal triamcinolone/anti-VEGF; no pain/fever; no progressive worsening; sterile cultures |
| Phacoanaphylactic inflammation | Exposed lens protein; AC reaction, KP, elevated IOP; sterile; history of lens injury |
| Orbital cellulitis | Proptosis, restricted EOM, fever; no anterior chamber reaction; periorbital signs without hypopyon |
| Acute uveitis flare | History of uveitis/HLA-B27; no fever; responds to steroids; no hypopyon typically |
| Lens particle uveitis | Post-surgical retained lens fragment; angle/vitreous particles; no organisms |
| Sympathetic ophthalmia | Bilateral granulomatous uveitis; following perforating injury; Dalen-Fuchs nodules; latency period |
- Wills Eye Manual
Q11. What is the role of steroids in management of endophthalmitis/panophthalmitis?
Answer:
Steroids play a dual role - reducing inflammation but potentially impairing immunity:
Topical corticosteroids:
- Prednisolone acetate 1% q1h - controls anterior segment inflammation, reduces secondary scarring
Intravitreal dexamethasone:
- 0.4 mg/0.1 mL - given alongside intravitreal antibiotics in severe vitreous inflammation
- Rationale: reduces cytokine-mediated retinal damage once infection is being controlled
Systemic corticosteroids:
- Oral prednisone 60 mg/day for 5 days - was part of the original EVS protocol
- Current use depends on: causative organism (avoid in fungal), patient comorbidities (caution in diabetics), severity and duration
- Once infection is sterilized, the post-endophthalmitis inflammation can be significant and should be treated aggressively
Key principle: Steroids should only be given AFTER adequate antibiotic coverage is established. Never use steroids without concurrent antibiotics.
- Wills Eye Manual
Q12. What is the prognosis of panophthalmitis, and what factors determine outcome?
Answer:
Prognosis is generally poor for visual recovery - panophthalmitis represents the most severe end of the spectrum. Key points:
Poor prognostic factors:
- Virulent organisms (Bacillus cereus, Pseudomonas, Streptococcus) - rapid destruction within hours
- Delayed presentation / delayed treatment
- Visual acuity at presentation of light perception or worse
- Traumatic etiology with IOFB
- Immunocompromised host
- Endogenous source (mortality risk from systemic sepsis)
Better prognostic factors:
- Less virulent organisms (S. epidermidis - most favorable)
- Early presentation and treatment
- Hand motion or better visual acuity at presentation
- Post-surgical rather than traumatic etiology
The retina is exquisitely sensitive: just a few hours of suppurative inflammation in the vitreous may be sufficient to cause irreversible retinal injury. This makes panophthalmitis an ophthalmic emergency.
Systemic risk: Endogenous panophthalmitis carries mortality risk from the underlying systemic infection (septicemia, Klebsiella pneumoniae syndrome).
- Robbins & Cotran, p.1216; Wills Eye Manual; Qi M et al, Semin Ophthalmol 2022 [PMID 34280072]
Q13. What is the significance of a "corneal ring ulcer" in panophthalmitis?
Answer:
A corneal ring ulcer (ring-shaped infiltrate/ulcer at the periphery of the cornea) in the context of panophthalmitis is a characteristic sign of:
- Gram-negative infection, particularly Pseudomonas aeruginosa or Acanthamoeba
- Indicates involvement of the limbal arcade and peripheral corneal stroma
- Suggests an antigen-antibody immune complex deposition mechanism at the limbus
- In Pseudomonas endophthalmitis/panophthalmitis, the disease is described as fulminant with rapid visual deterioration, fever, leukocytosis, proptosis, corneal ring ulcer, and panophthalmitis
Its presence alongside panophthalmitis signs is a grave prognostic indicator requiring:
- Immediate intravitreal + systemic gram-negative coverage
- Surgical intervention (PPV)
- Wills Eye Manual; Harrison's 22e
Q14. What is sympathetic ophthalmia and how does it relate to panophthalmitis / penetrating trauma?
Answer:
Sympathetic ophthalmia is a bilateral granulomatous uveitis that occurs after penetrating injury (or surgery) to one eye (exciting eye), affecting the other (sympathizing eye).
Mechanism: T-cell mediated autoimmune reaction against uveal antigens (melanocytes) exposed by the trauma. The uninjured eye mounts an immune response against its own uveal tissue.
Relevance to panophthalmitis:
- Penetrating trauma causing panophthalmitis is a risk factor
- To prevent sympathetic ophthalmia in a blind, painful eye, enucleation within 2 weeks of the inciting trauma was classically recommended (before the inflammatory response becomes self-sustaining)
- Once sympathetic ophthalmia has developed, enucleation of the exciting eye may not prevent progression in the sympathizing eye
Why it matters in viva:
- This is the primary reason for considering enucleation rather than evisceration - evisceration may not remove all uveal tissue and theoretically carries a (disputed) risk of sympathetic ophthalmia
- Treatment of sympathetic ophthalmia: high-dose systemic corticosteroids, immunosuppressants (mycophenolate, azathioprine, cyclosporine)
- Kanski's Clinical Ophthalmology 10e; Wills Eye Manual
Q15. A patient presents 2 days after cataract surgery with severe eye pain, hypopyon, and absent red reflex. Visual acuity is light perception. What is your management?
Answer:
This is acute post-operative endophthalmitis with VA = LP. Manage as follows:
-
Immediate hospitalization - ophthalmic emergency
-
Cultures first: Vitreous tap (0.2 mL) + anterior chamber paracentesis (0.2 mL) - Gram stain, blood agar, chocolate agar, Sabouraud, thioglycolate
-
Intravitreal antibiotics immediately:
- Vancomycin 1 mg/0.1 mL (Gram-positive coverage)
- Ceftazidime 2.2 mg/0.1 mL (Gram-negative coverage)
- ± Dexamethasone 0.4 mg/0.1 mL intravitreally
-
Immediate pars plana vitrectomy - VA = LP is the EVS threshold; PPV gives 3× better visual outcome vs tap alone
-
Topical therapy:
- Prednisolone acetate 1% q1h
- Atropine 1% b.i.d.-t.i.d.
- Fortified vancomycin + tobramycin q1h (if wound leak/bleb)
-
Systemic antibiotics: Moxifloxacin 400 mg PO/IV daily (achieves therapeutic vitreous levels) - not proven to improve outcomes per EVS, but used in severe/bleb-related cases
-
Follow up q12-24h: Relief of pain at 48h is a good prognostic sign. If no improvement at 48h - repeat intravitreal antibiotics; reassess for drug-resistant organisms or fungal etiology
-
If cultures grow organism - narrow antibiotics accordingly
- Wills Eye Manual; EVS Study reference
Summary Table: High-Yield Viva Points
| Point | Answer |
|---|---|
| Definition | Inflammation of entire eye including sclera extending into orbit |
| Most common organism (post-cataract) | S. epidermidis |
| Most virulent organism | Bacillus cereus (destroys eye in 12-24h) |
| Corneal ring ulcer suggests | Gram-negative (Pseudomonas) |
| First-line intravitreal antibiotics | Vancomycin + Ceftazidime |
| EVS threshold for PPV | VA = light perception or worse |
| Systemic antibiotic that reaches vitreous | Moxifloxacin |
| Endogenous panophthalmitis classic cause | Klebsiella (diabetic, liver abscess) |
| Surgery to prevent sympathetic ophthalmia | Enucleation within 2 weeks |
| Preferred surgery in panophthalmitis | Evisceration (unless tumor suspected) |
| Most sensitive sample for culture | Vitreous tap (> AC tap) |
| Steroid rule | Only after antibiotic coverage established |
| Retinal tolerance of vitreous suppuration | Only a few hours before irreversible damage |
This is a shared conversation. Sign in to Orris to start your own chat.