Iron deficiency anemia
"iron deficiency anemia" AND treatment
Iron Deficiency Anemia
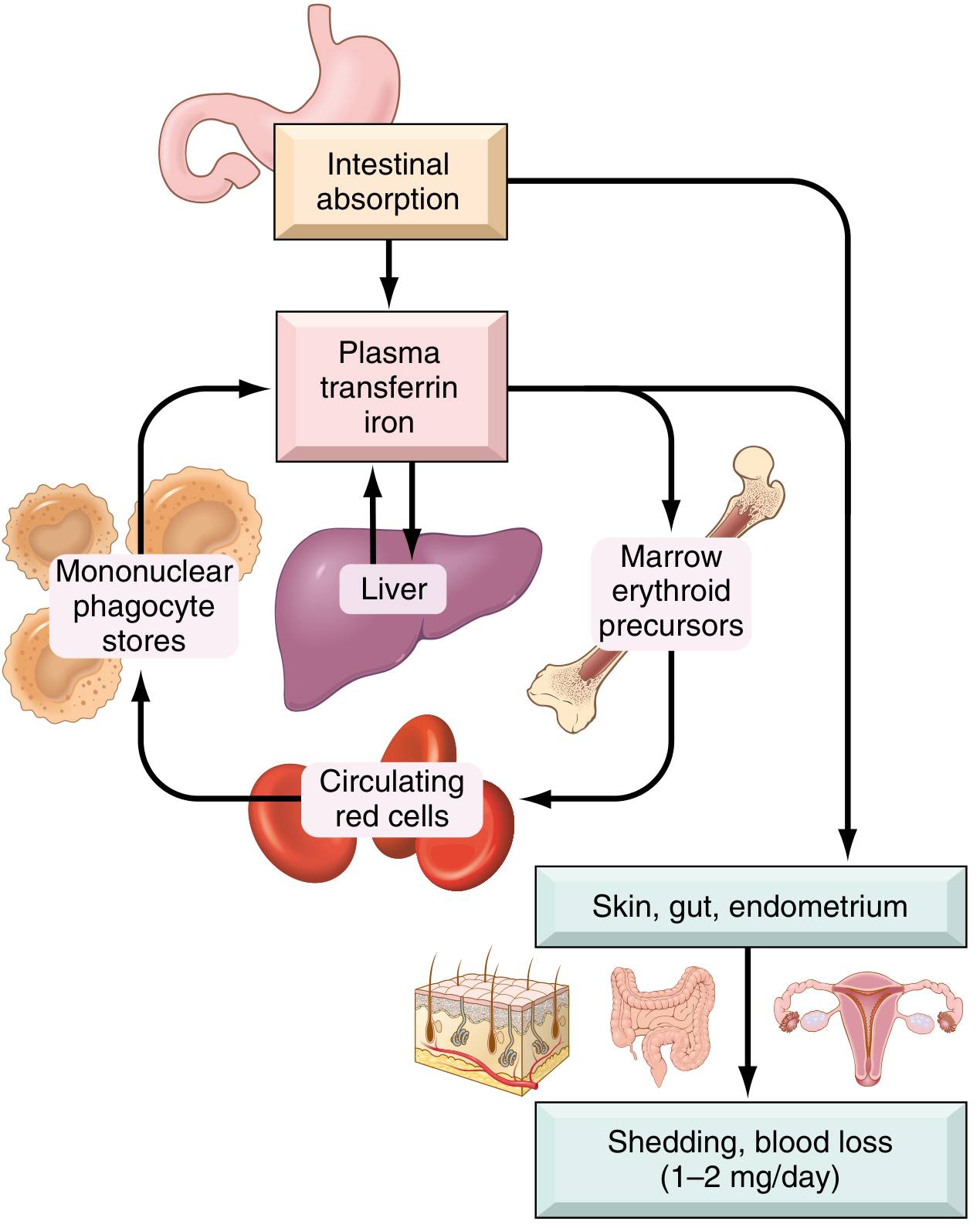
Iron Metabolism - Normal Physiology
| Pool | Males (mg) | Females (mg) |
|---|---|---|
| Hemoglobin | 2100 | 1750 |
| Myoglobin | 300 | 250 |
| Enzymes | 50 | 50 |
| Ferritin/hemosiderin (storage) | 1000 | 400 |
| Total | 3450 | 2450 |
- Daily dietary iron in the US: 10-20 mg; daily losses: 1-2 mg (shed epithelial/mucosal cells)
- Heme iron (animal products): ~20% absorbed. Non-heme iron (vegetables): only 1-2% absorbed
- Average daily requirement: 7-10 mg (males), 7-20 mg (females)
- Absorption is enhanced by ascorbic acid, citric acid, amino acids; inhibited by tannins (tea), carbonates, oxalates, phosphates
Hepcidin - The Master Regulator
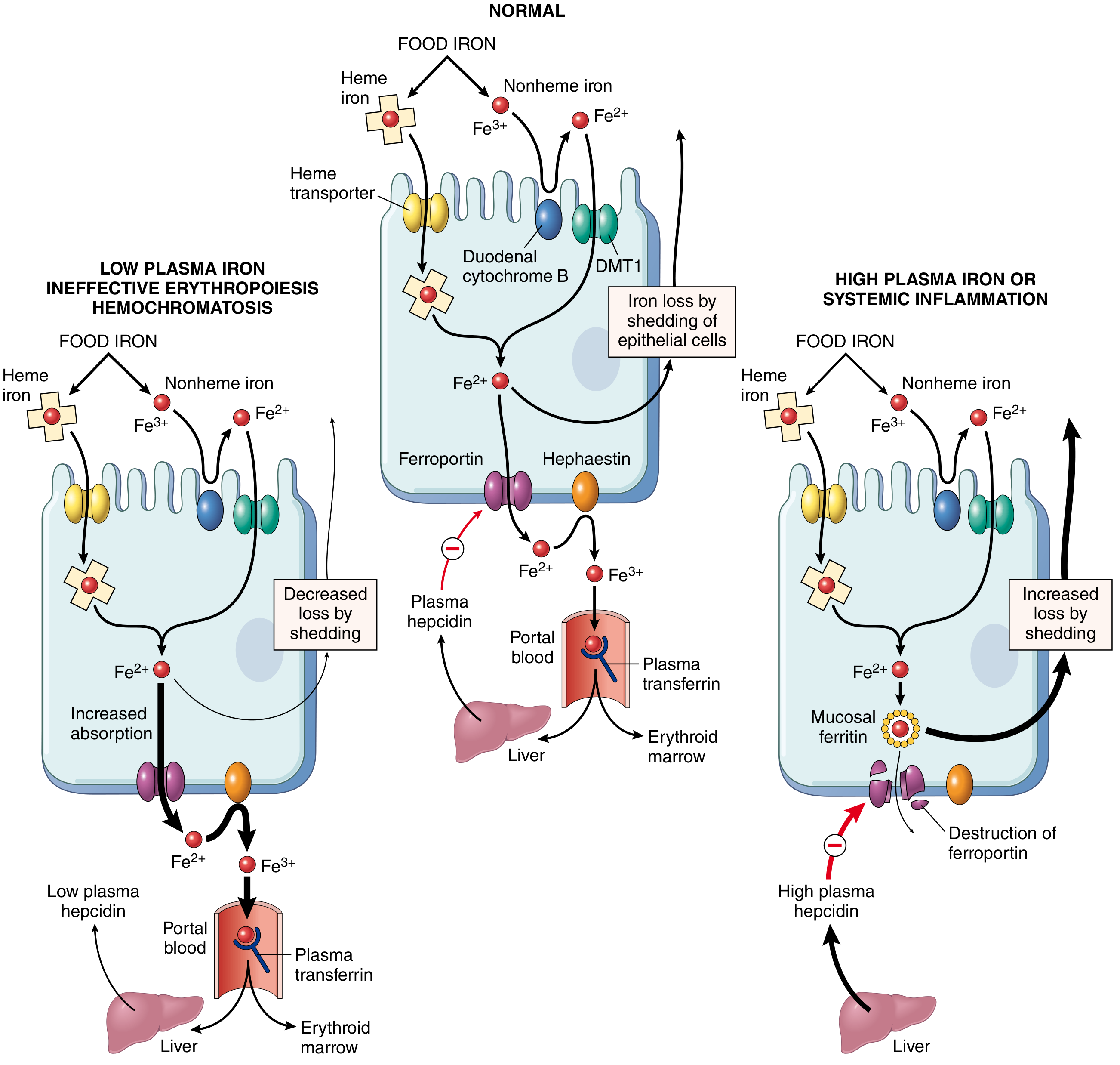
- Non-heme iron is reduced from Fe³⁺ to Fe²⁺ by ferrireductases (duodenal cytochrome B), then transported into enterocytes by DMT1
- Fe²⁺ exits the enterocyte via ferroportin, is oxidized by hephaestin/ceruloplasmin to Fe³⁺, and binds transferrin
- Hepcidin (hepatic peptide) binds ferroportin → endocytosis and degradation → traps iron in enterocytes → iron lost as cells slough
- In iron deficiency: hepcidin falls → increased absorption
- In chronic inflammation: hepcidin rises → iron sequestration in macrophages → anemia of chronic disease
Etiology
| Cause | Examples |
|---|---|
| Dietary lack | Low-resource countries; infant/toddler diets poor in meat; vegetarian diets |
| Impaired absorption | Celiac disease, gastrectomy, achlorhydria, H. pylori infection (decreases absorption + microerosions), Crohn's disease |
| Increased requirement | Pregnancy, lactation, rapid growth in infancy/adolescence |
| Chronic blood loss | GI bleeding (peptic ulcer, colorectal cancer, hookworm), menorrhagia, hematuria |
Chronic blood loss is the most common cause in adult males and postmenopausal women in high-resource countries - GI malignancy must be excluded.
Stages of Iron Deficiency
- Storage depletion - serum ferritin falls, bone marrow iron disappears (Prussian blue stain negative)
- Transport depletion - serum iron falls, TIBC rises, transferrin saturation falls (<15%)
- Functional deficiency - hemoglobin synthesis impaired → microcytic, hypochromic anemia
Morphology

- Small cells (microcytic)
- Pale/central pallor enlarged (normally 1/3 diameter; in IDA, hemoglobin seen only at rim)
- "Pencil cells" (elongated red cells) - characteristic
- Poikilocytosis
Clinical Features
- Fatigue, pallor, weakness, dyspnea on exertion, palpitations
| Sign | Description |
|---|---|
| Koilonychia | Spoon-shaped nails |
| Alopecia | Hair loss |
| Pica | Craving for non-food items (clay); or specific foods like ice (pagophagia) |
| Atrophic glossitis | Tongue becomes smooth and pale |
| Esophageal webs | Can cause dysphagia |
| Plummer-Vinson syndrome | Triad: microcytic anemia + atrophic glossitis + esophageal webs |
Laboratory Diagnosis
| Test | Finding in IDA |
|---|---|
| Hemoglobin/Hematocrit | Low (moderate reduction) |
| MCV | Low (<80 fL) - microcytic |
| MCH/MCHC | Low - hypochromic |
| Serum iron | Low |
| TIBC (transferrin) | High (increased transferrin synthesis) |
| Transferrin saturation | <15% |
| Serum ferritin | Low (<12 µg/L) - most sensitive early marker |
| Serum hepcidin | Low |
| Reticulocyte count | Low (then rises with treatment) |
| Peripheral smear | Microcytic, hypochromic, pencil cells |
| Bone marrow (Prussian blue) | Absent stainable iron |
Ferritin is the most sensitive and specific early marker. In pregnancy, a ferritin cutoff of 30 ng/mL gives 92% sensitivity and 98% specificity.
Treatment
- Ferrous sulfate 325 mg (65 mg elemental iron) 1-3×/day
- Non-enteric-coated preparations preferred for absorption
- Take on empty stomach or with vitamin C to enhance absorption; avoid with tea/dairy/antacids
- Single daily dosing is as effective as multiple doses and has fewer GI side effects (important in pregnancy)
- Reticulocytosis appears in 5-7 days; hemoglobin rises over 6-8 weeks; continue therapy for 3-6 months after normalization to replenish stores
- Oral intolerance or malabsorption
- Severe anemia (Hgb <9 g/dL)
- Ongoing rapid blood loss
- Pregnancy: IV iron is the treatment of choice in the third trimester and for severe IDA (Hgb <9 g/dL) in the second trimester
- Formulations: ferric carboxymaltose, iron sucrose, low-molecular-weight iron dextran
- Note: A 2025 systematic review (PMID 39935027) identified hypophosphatemia as a significant adverse effect of ferric carboxymaltose (FCM)
GI Work-up
- All adult males (any age)
- All postmenopausal women
- Colonoscopy first
- Upper endoscopy + push enteroscopy if colonoscopy negative
- Duodenal biopsy for celiac disease
- Test and treat H. pylori if found
- Capsule endoscopy if all above are negative
- Pursue non-GI causes if capsule study is also negative
Special Populations
- Iron deficiency occurs in ~18% of US pregnancies; IDA in ~5%
- Severe anemia (<6-7 g/dL) associated with preterm birth, fetal mortality, PROM, gestational hypertension
- ACOG/WHO recommend at least 30 mg elemental iron daily; intermittent dosing (2-3×/week) reduces GI side effects while maintaining efficacy
- A 2024 USPSTF systematic review (PMID 39163033) examined screening and supplementation in pregnancy - supports universal supplementation recommendations
Key Differentials (Microcytic Anemia)
| Feature | IDA | Thalassemia | Anemia of Chronic Disease |
|---|---|---|---|
| Serum iron | Low | Normal/high | Low |
| TIBC | High | Normal | Low/normal |
| Ferritin | Low | Normal/high | Normal/high |
| Hepcidin | Low | Low (thal major) | High |
| RBC count | Low | Often normal/high | Low |
AML
"acute myeloid leukemia" AND treatment
HTTP 502 for https://eutils.ncbi.nlm.nih.gov/entrez/eutils/esearch.fcgi?tool=orrisai&email=dev%40orris.ai&api_key=***&db=pubmed&term=%28%22acute+myeloid+leukemia%22+AND+treatment%29+AND+%28%22Meta-Analysis%22%5Bpt%5D+OR+%22Systematic+Review%22%5Bpt%5D+OR+%22Practice+Guideline%22%5Bpt%5D%29+NOT+%22Retracted+Publication%22%5Bpt%5D&retmode=json&retmax=3&sort=relevance&datetype=pdat&reldate=730
We encountered an error while processing your request. Please try again or reach out to us for help.
Chronic myeloid leukemia
An error occurred (ValidationException) when calling the ConverseStream operation: Expected toolResult blocks at messages.18.content for the following Ids: tooluse_9LC6wryZVruEQcKy6dnOBD
We encountered an error while processing your request. Please try again or reach out to us for help.