Explain the emergency drug that is adrenals its pathway mechanism its physiology in detail and protocols and criteria before giving in emergency condition
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive data from multiple authoritative textbooks. Let me compile the complete, detailed response.
Adrenaline (Epinephrine) — The Primary Emergency Drug
Origin: The Adrenal Medulla
Epinephrine (adrenaline) is the principal hormone of the adrenal medulla, secreted by chromaffin cells — which are specialized modified postganglionic sympathetic neurons. The adrenal medulla is innervated by preganglionic cholinergic sympathetic fibers from the hypothalamus. Under stress (pain, hemorrhage, exercise, hypoglycemia, hypoxia), the hypothalamus fires impulses down to preganglionic neurons → acetylcholine is released → chromaffin cell membranes depolarize → Ca²⁺ rapidly enters → exocytosis of epinephrine-containing chromaffin granules into the bloodstream.
The adrenal medulla secretes roughly 80% epinephrine and 20% norepinephrine.
Biosynthetic Pathway (Catecholamine Synthesis)
The pathway proceeds from dietary amino acids entirely within chromaffin cells and adrenergic neurons:
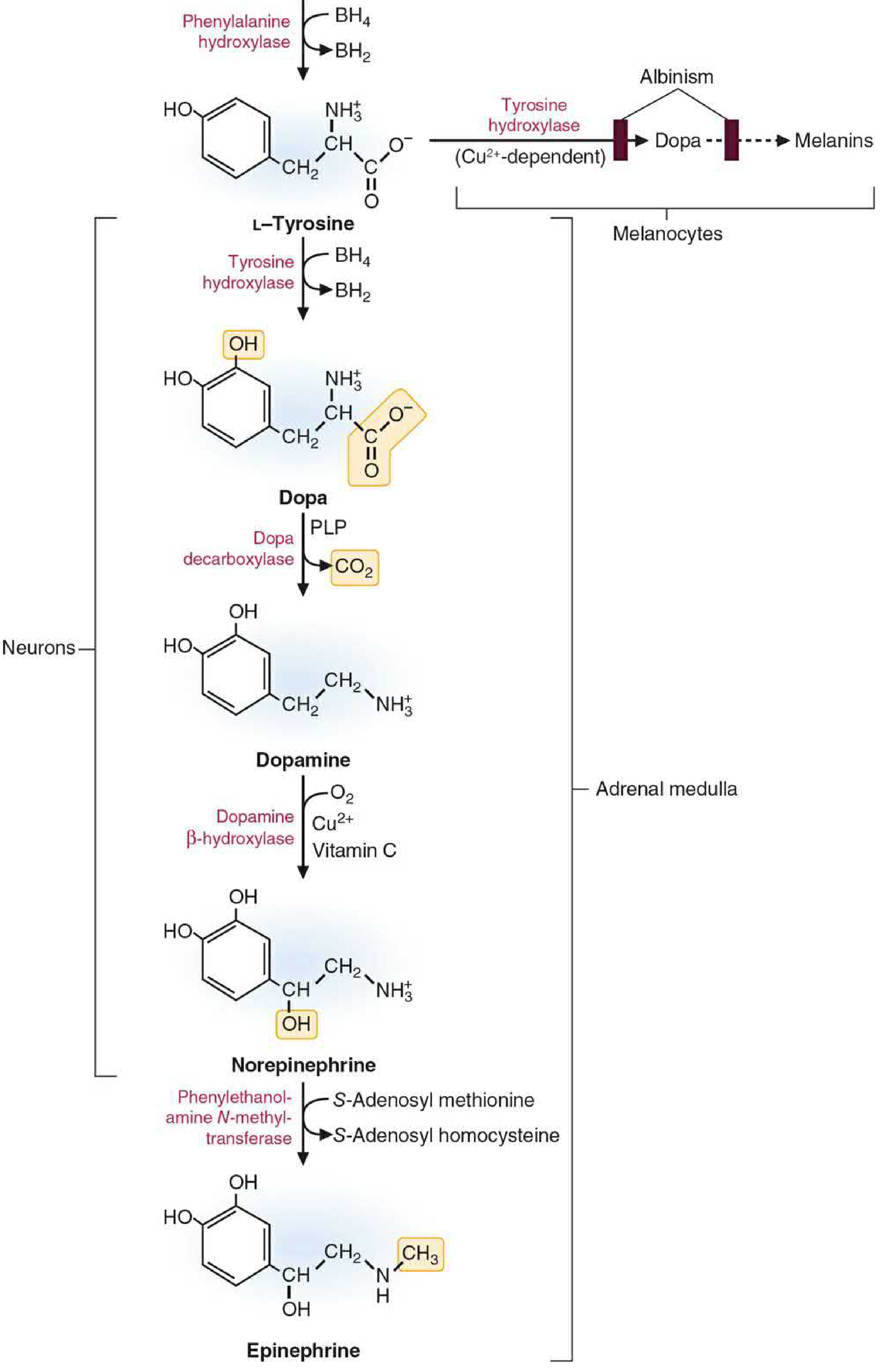
Catecholamine and melanin biosynthesis — Basic Medical Biochemistry: A Clinical Approach, 6e
Step-by-Step:
| Step | Substrate → Product | Enzyme | Cofactors | Location |
|---|---|---|---|---|
| 1 (rate-limiting) | L-Tyrosine → L-DOPA | Tyrosine hydroxylase (TH) | Tetrahydrobiopterin (BH₄) | Cytosol |
| 2 | L-DOPA → Dopamine | DOPA decarboxylase (AADC) | Pyridoxal phosphate (Vit B₆) | Cytosol |
| 3 | Dopamine → Norepinephrine | Dopamine β-hydroxylase (DBH) | Vitamin C (ascorbic acid), Cu²⁺, O₂ | Storage vesicles |
| 4 | Norepinephrine → Epinephrine | PNMT (phenylethanolamine-N-methyltransferase) | S-Adenosyl methionine (SAM), Vit B₁₂, folate | Cytoplasm (NE exits vesicle, is methylated, re-enters) |
Key points:
- Step 1 (TH) is the rate-limiting step — most regulated pharmacologically
- Step 4 (PNMT) is unique to the adrenal medulla and epinephrine-containing neurons; requires cortisol from the adrenal cortex (portal blood) to upregulate PNMT — creating a functional synergy between the cortisol axis and the catecholamine axis under stress
- Epinephrine is stored in chromaffin granules complexed with ATP and chromogranins; VMAT2 (vesicle monoamine transporter 2) mediates H⁺-gradient-driven uptake into granules
Receptor Mechanism of Action
Epinephrine is a mixed α- and β-adrenergic receptor agonist — the most potent endogenous catecholamine. All adrenergic receptors are G-protein coupled receptors (GPCRs).
Receptor Subtypes and Downstream Signaling:
| Receptor | G-Protein | Second Messenger | Effect |
|---|---|---|---|
| α₁ | Gq | ↑ IP₃/DAG → ↑ Ca²⁺ | Vasoconstriction, ↑ SVR, reduces mucosal edema |
| α₂ | Gi | ↓ cAMP | Presynaptic inhibition, platelet aggregation |
| β₁ | Gs | ↑ cAMP → PKA | ↑ heart rate (chronotropy), ↑ contractility (inotropy) |
| β₂ | Gs | ↑ cAMP → PKA | Bronchodilation, vasodilation, stabilizes mast cells/basophils |
Physiological Effects of Epinephrine by System:
Cardiovascular:
- α₁: vasoconstriction → ↑ systemic vascular resistance (SVR) → ↑ blood pressure (critical in shock)
- β₁: ↑ heart rate, ↑ myocardial contractility, ↑ cardiac output
- Coronary blood flow: primarily increases via metabolic autoregulation (not direct receptor activation); but can directly constrict epicardial coronaries via α₁ at high doses
Respiratory:
- β₂: bronchodilation of airway smooth muscle → treats bronchospasm of anaphylaxis/asthma
- Reduces mucosal edema via α₁ vasoconstriction → reduces laryngeal edema
Metabolic (counterregulatory hormone — "fight or flight"):
- ↑ Glycogenolysis in liver and muscle (β₂/β₃) → ↑ blood glucose
- ↑ Gluconeogenesis in liver
- ↑ Lipolysis in adipose tissue → ↑ free fatty acids
- Inhibits insulin secretion, stimulates glucagon secretion from pancreas
- Net effect: mobilizes fuel substrates for energy under acute stress
Immunological/Allergic:
- Mast cell and basophil stabilization via β₂ → inhibits further mediator (histamine, leukotriene) release
- This is why it is uniquely effective in anaphylaxis — it addresses all pathophysiological arms simultaneously
Half-life: Epinephrine has a very short half-life in blood (~2 minutes); inactivated by:
- Reuptake into presynaptic terminals
- MAO (monoamine oxidase) — mitochondrial
- COMT (catechol-O-methyltransferase) — extraneuronal Final metabolites: vanillylmandelic acid (VMA), metanephrines → excreted in urine
Emergency Indications & Protocols
1. ANAPHYLAXIS — First-Line Drug
Criteria for epinephrine in anaphylaxis (treat immediately when 2+ of the following occur rapidly after allergen exposure, OR hypotension alone after known allergen):
- Urticaria/angioedema + respiratory difficulty (stridor, wheeze, dyspnea)
- Urticaria/angioedema + hypotension or syncope
- Skin involvement + GI symptoms (vomiting, cramping)
- Isolated severe hypotension after known allergen
"There are NO absolute contraindications to epinephrine in anaphylaxis." — Rosen's Emergency Medicine & Tintinalli's Emergency Medicine
Anaphylaxis Treatment Algorithm:
Step 1 — Immediate: Airway, Breathing, Circulation
- Assess airway (look for uvular edema, stridor, angioedema — intubate early if threatening)
- Oxygen to maintain SpO₂ >90%
- IV access + cardiac monitoring
- Supine position (or recovery position if vomiting)
- Remove causative agent if identifiable
Step 2 — Epinephrine (First-Line)
| Route | Adult Dose | Pediatric Dose |
|---|---|---|
| IM (preferred) — anterolateral thigh | 0.3–0.5 mg (0.3–0.5 mL of 1:1000) | 0.01 mg/kg (0.01 mL/kg of 1:1000); max 0.5 mg |
| Auto-injector (EpiPen®) | 0.3 mg IM | 0.15 mg (<30 kg) — EpiPen Jr® |
| Repeat | Every 5–10 minutes if no response | Same interval |
| IV bolus (if cardiovascular collapse) | 100 mcg over 5–10 min (0.1 mg in 10 mL NS) | — |
| IV infusion (refractory shock) | Start 1 mcg/min (1 mg in 1000 mL NS at 1 mL/min); titrate to 10 mcg/min max | 0.1 mcg/kg/min → max 1.5 mcg/kg/min |
IM injection into the anterolateral thigh achieves higher, faster, more consistent peak plasma levels than deltoid or SC injection. Central venous access preferred for IV infusion — tissue necrosis risk from extravasation.
Step 3 — Fluid Resuscitation
- Adults: 1–2 L NS or LR rapid bolus (up to 7 L may be required)
- Pediatrics: 20 mL/kg bolus, repeat as needed
- Intraosseous access if IV not achievable
Step 4 — Second-Line Agents (adjuncts — do NOT precede or replace epinephrine):
| Drug | Adult Dose | Role |
|---|---|---|
| Diphenhydramine (H₁ blocker) | 25–50 mg IV/IM | Cutaneous symptoms |
| Ranitidine (H₂ blocker) | 50 mg IV over 5 min | Added antihistamine effect |
| Hydrocortisone | 250–500 mg IV | Prevents biphasic reaction |
| Methylprednisolone | 80–125 mg IV | Prevents biphasic reaction |
| Albuterol (salbutamol) | 2.5–5 mg nebulized | Persistent bronchospasm |
| Glucagon | 1–5 mg IV over 5 min, then 5–15 mcg/min infusion | Patients on β-blockers (epinephrine's β-effects blocked → glucagon bypasses β-receptor) |
Special situation — Beta-Blocker Patients:
If patient is on beta-blockers, epinephrine's β₂ effects are blocked → paradoxical hypertension from unopposed α₁ stimulation can occur → use glucagon + higher IV epinephrine doses + IV fluids.
Observation criteria after anaphylaxis treatment:
- Observe for biphasic anaphylaxis (recurrence 1–72 hrs later; risk higher with severe initial episode, multiple epinephrine doses)
- Admit or observe ≥4–6 hours if: protracted reaction, IV epinephrine required, >1 dose IM epinephrine, airway involvement, unknown trigger, poor social support
- Discharge requires: EpiPen® prescription + instruction, allergen avoidance plan, allergist referral
2. CARDIAC ARREST — ACLS Protocol
Criteria: Pulseless cardiac arrest confirmed — VF, pulseless VT, asystole, or PEA
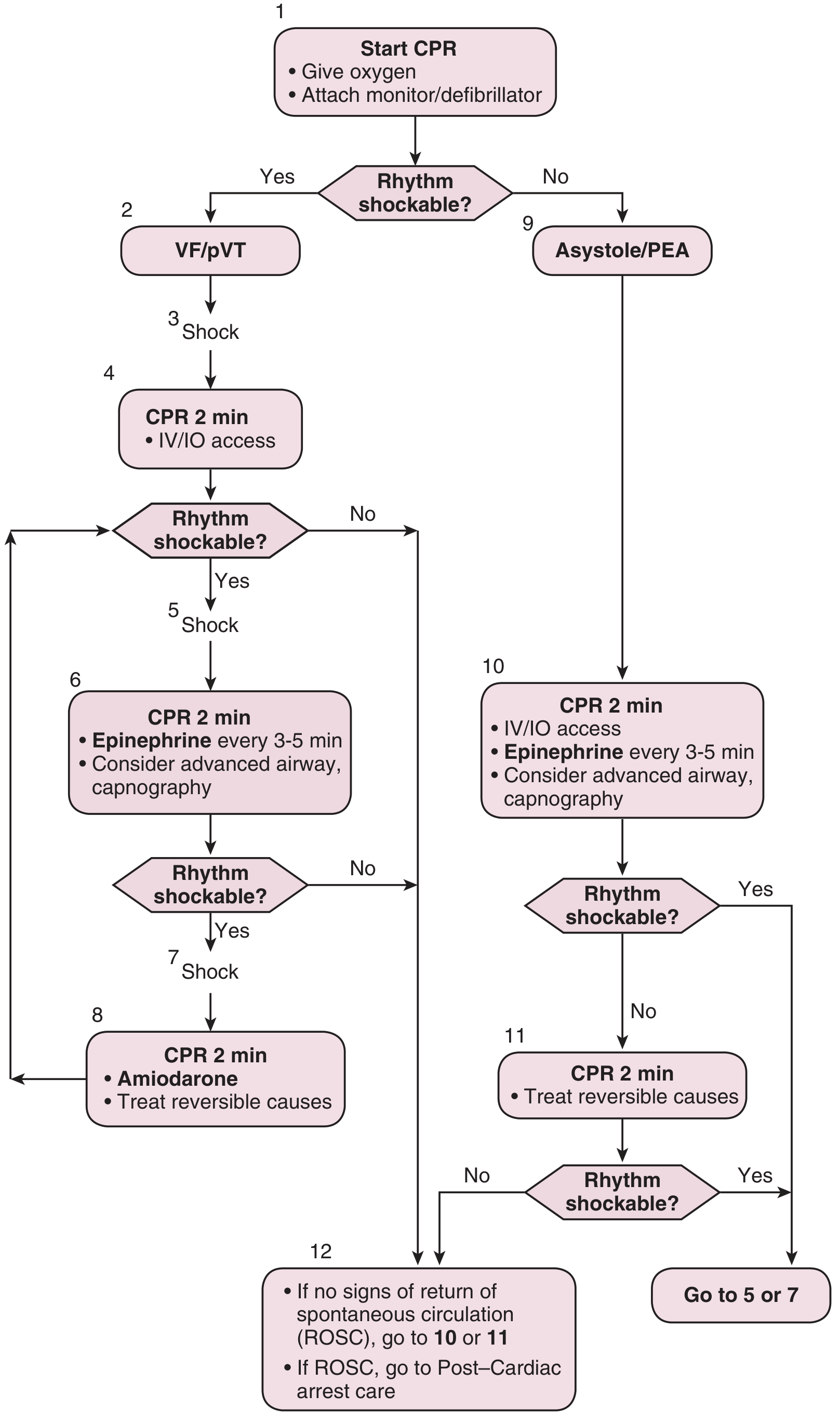
Adult Cardiac Arrest Algorithm — Roberts and Hedges' Clinical Procedures in Emergency Medicine
Protocol:
| Rhythm | Epinephrine Timing | Dose |
|---|---|---|
| VF/pVT (shockable) | After 2nd shock + CPR cycle | 1 mg IV/IO every 3–5 minutes |
| Asystole/PEA (non-shockable) | Immediately with CPR | 1 mg IV/IO every 3–5 minutes |
CPR Quality Standards:
- Push hard ≥2 inches (5 cm), fast 100–120/min, full chest recoil
- Minimize interruptions; rotate compressor every 2 minutes
- 30:2 compressions:ventilations (no advanced airway); 1 breath every 6 sec with advanced airway
Drug Therapy in Arrest:
- Epinephrine: 1 mg IV/IO every 3–5 min (only drug for asystole/PEA; for VF/pVT after shocks)
- Amiodarone: 300 mg IV/IO (1st dose), 150 mg (2nd dose) — for refractory VF/pVT
- Vasopressin: removed from 2015 ACLS guidelines (equivalent to epinephrine, simplified algorithm)
Mechanism in arrest: Epinephrine's α₁ vasoconstriction → ↑ aortic diastolic pressure → ↑ coronary perfusion pressure during CPR → improves chances of ROSC (return of spontaneous circulation)
Note: No ACLS drug, including epinephrine, has been proven to improve long-term neurological survival. A worsened neurological outcome has been associated with epinephrine use (possibly from prolonged cerebral vasoconstriction). It improves ROSC rates but long-term benefit remains debated.
Reversible causes to treat (4 H's and 4 T's):
- Hypovolemia, Hypoxia, Hydrogen ion (acidosis), Hypo/hyperkalemia, Hypothermia
- Tension pneumothorax, Tamponade, Toxins, Thrombosis (pulmonary/coronary)
3. OTHER EMERGENCY USES
| Indication | Route/Dose | Mechanism Used |
|---|---|---|
| Severe croup (laryngotracheobronchitis) | Nebulized racemic epinephrine 0.5 mL of 2.25% in 3 mL NS | α₁ mucosal vasoconstriction → reduces subglottic edema |
| Acute severe asthma (refractory to bronchodilators) | 0.3 mg SC/IM 1:1000 | β₂ bronchodilation |
| Upper GI bleeding (injection) | Local 1:10,000 | α₁ vasoconstriction |
| Local anesthetic adjunct | 1:100,000–1:200,000 dilution | α₁ vasoconstriction → prolongs nerve block, ↓ bleeding |
| Hypoglycemia refractory to glucose | 0.5–1 mg SC/IM | Stimulates hepatic glycogenolysis |
Contraindications and Cautions
In anaphylaxis and cardiac arrest: NO absolute contraindications exist.
Relative cautions (not contraindications) in non-arrest settings:
- Cardiac arrhythmias: monitor closely; epinephrine can trigger dysrhythmias
- Hypertension: α₁-mediated surge — use lower doses and careful titration
- Beta-blocker use: risk of paradoxical hypertension from unopposed α₁ effects
- Ischemic heart disease: may ↑ myocardial oxygen demand; still use in true emergency
- Hyperthyroidism: increased sensitivity to catecholamines
- Pregnancy: use in true emergency; monitor fetal heart rate
Side effects:
- Palpitations, anxiety, tremor, pallor, dizziness, headache
- Hypertensive crisis (especially with β-blockers)
- Cardiac arrhythmias (especially IV bolus without dilution)
- Tissue necrosis if IV extravasates → requires central line for infusions
- Pulmonary edema (high doses, pre-existing cardiac/pulmonary disease)
Summary Table
| Feature | Detail |
|---|---|
| Class | Endogenous catecholamine; sympathomimetic |
| Source | Adrenal medulla chromaffin cells (80% of medullary output) |
| Synthesis | Tyrosine → DOPA → Dopamine → NE → Epinephrine (via PNMT + SAM) |
| Rate-limiting step | Tyrosine hydroxylase (step 1) |
| Receptors | α₁, α₂, β₁, β₂ (mixed agonist) |
| Primary emergency uses | Anaphylaxis (1st line), Cardiac arrest, Severe croup |
| Anaphylaxis dose | IM 0.3–0.5 mg (adult), 0.01 mg/kg (child) — anterolateral thigh |
| Cardiac arrest dose | IV/IO 1 mg every 3–5 minutes |
| Half-life | ~2 minutes (inactivated by MAO + COMT) |
| Contraindications | None absolute in emergencies |
Sources: Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Basic Medical Biochemistry (Lieberman & Peet, 6e); Kaplan & Sadock's Comprehensive Textbook of Psychiatry; Barash, Cullen & Stoelting's Clinical Anesthesia, 9e; Roberts and Hedges' Clinical Procedures in Emergency Medicine; The Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.