Tell me 10 common heart diseases with ecg graph and changes occur in ecg
ECG changes heart diseases electrocardiogram
atrial fibrillation ECG rhythm strip
ST elevation myocardial infarction STEMI ECG
ventricular tachycardia ECG wide QRS
left ventricular hypertrophy ECG voltage criteria
heart block AV block first degree second degree third degree ECG PR interval
pericarditis ECG saddle shape ST elevation diffuse
pulmonary embolism ECG S1Q3T3 right heart strain
Wolff-Parkinson-White WPW syndrome ECG delta wave short PR
hypertrophic cardiomyopathy ECG deep Q waves septal hypertrophy
10 Common Heart Diseases with ECG Changes
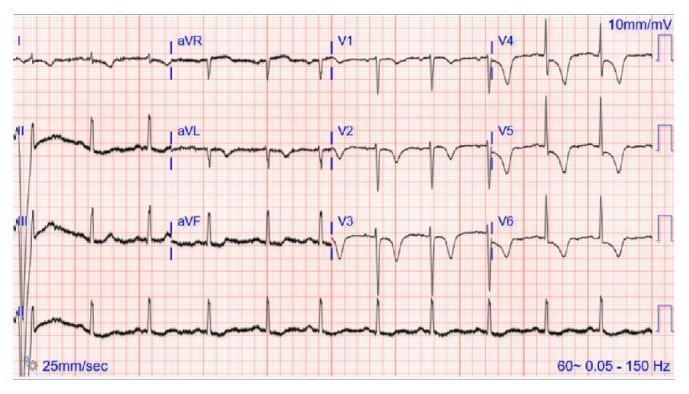
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
- ST-segment elevation ≥1 mm in ≥2 contiguous leads (convex/tombstone morphology)
- Reciprocal ST depression in opposite leads
- Hyperacute T waves (tall, broad, peaked) — earliest sign
- Pathological Q waves develop within hours (>40 ms wide, >25% R-wave height) — marker of necrosis
- T-wave inversion in evolutionary phase
| Territory | Elevated Leads | Reciprocal Depression |
|---|---|---|
| Anterior (LAD) | V1–V4 | II, III, aVF |
| Inferior (RCA) | II, III, aVF | aVL, I |
| Lateral (LCx) | I, aVL, V5–V6 | II, III, aVF |

2. 🫀 Non-ST-Elevation ACS (NSTEMI / Unstable Angina)
- ST depression (horizontal or downsloping) ≥0.5–1 mm in ≥2 contiguous leads
- T-wave inversion — deep, symmetric (Wellens syndrome pattern: biphasic or deeply inverted T waves in V2–V3 = critical LAD stenosis)
- No ST elevation, no Q waves
- May have transient ST elevation during ischemic episode
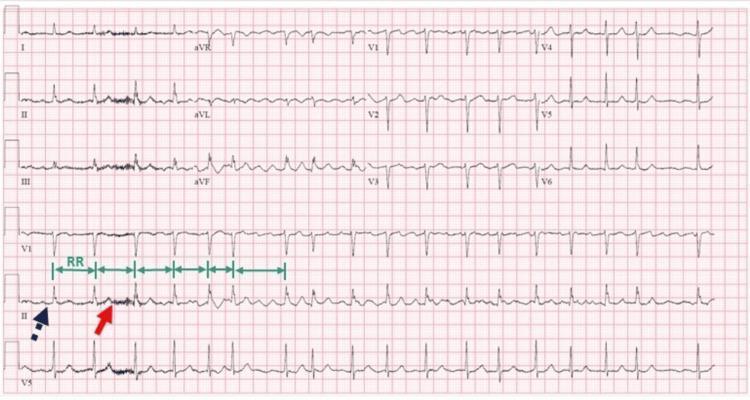
3. 🫀 Atrial Fibrillation (AF)
- Absent P waves — replaced by irregular fibrillatory (f) waves (best seen in V1 and lead II), rate 350–600/min
- Irregularly irregular RR intervals — the hallmark
- Narrow QRS complexes (unless aberrant conduction or pre-excitation)
- Ventricular rate typically 100–180/min in uncontrolled AF
- If AF + regular slow ventricular rate → suspect complete heart block
4. 🫀 Ventricular Tachycardia (VT)
- Wide QRS complexes ≥120 ms (often ≥160 ms)
- Regular rapid rhythm — rate 100–250 bpm
- AV dissociation — P waves independent of QRS (hallmark of VT vs SVT)
- Fusion beats and capture beats (Dressler beats) — pathognomonic
- Concordance — all QRS complexes in V1–V6 pointing same direction
- No RBBB/LBBB typical morphology (Brugada criteria help distinguish from SVT with aberrancy)

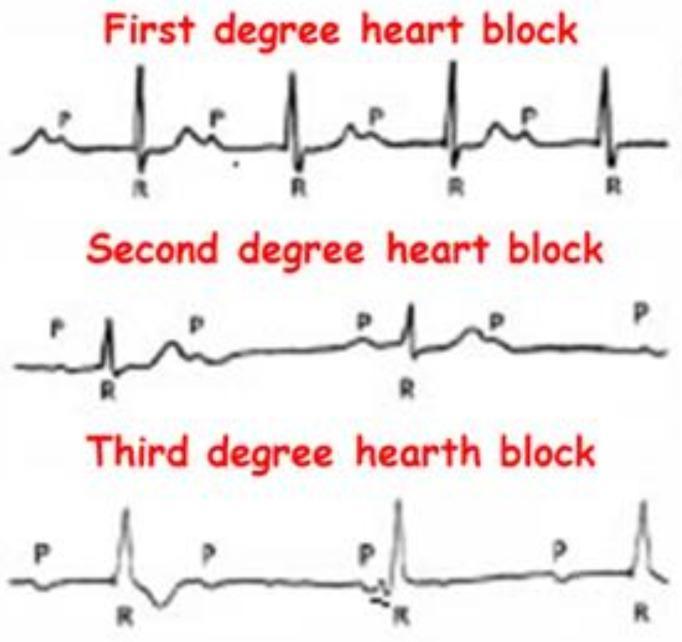
5. 🫀 AV Heart Block (1°, 2°, 3°)
| Type | ECG Finding |
|---|---|
| 1° AV Block | PR interval >200 ms (1 large box); every P conducts |
| 2° Mobitz I (Wenckebach) | Progressive PR lengthening until a QRS is dropped; RR shortens before dropped beat |
| 2° Mobitz II | Fixed PR interval, then sudden non-conducted P wave — higher risk |
| 3° (Complete) Block | Complete AV dissociation — atrial rate > ventricular rate; wide or junctional escape rhythm |
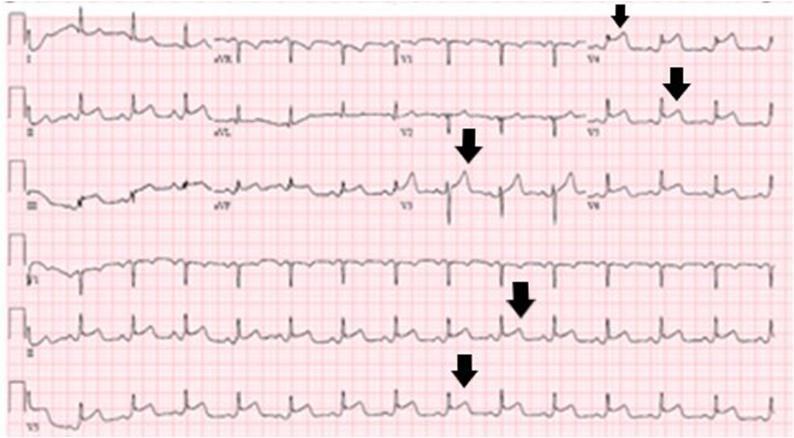
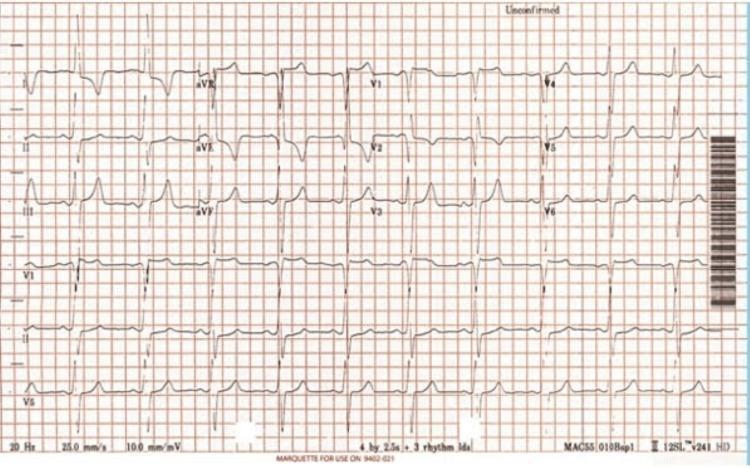
6. 🫀 Left Ventricular Hypertrophy (LVH)
- High voltage criteria (Sokolow-Lyon): S in V1 + R in V5 or V6 ≥35 mm
- Cornell criteria: R in aVL + S in V3 >28 mm (men) / >20 mm (women)
- LV strain pattern: ST depression + T-wave inversion in lateral leads (I, aVL, V5–V6)
- Left axis deviation
- Prolonged QRS duration (can reach 110 ms)
- Left atrial enlargement: bifid P wave (P mitrale) in II, negative terminal component in V1
7. 🫀 Acute Pericarditis
- Stage 1 (acute): Diffuse concave/saddle-shaped ST elevation in almost all leads (except aVR and V1 which show ST depression); PR depression (most sensitive early sign, best in lead II); Spodick's sign — downsloping TP segment
- Stage 2: ST normalizes, T waves flatten
- Stage 3: Diffuse T-wave inversions
- Stage 4: ECG returns to normal

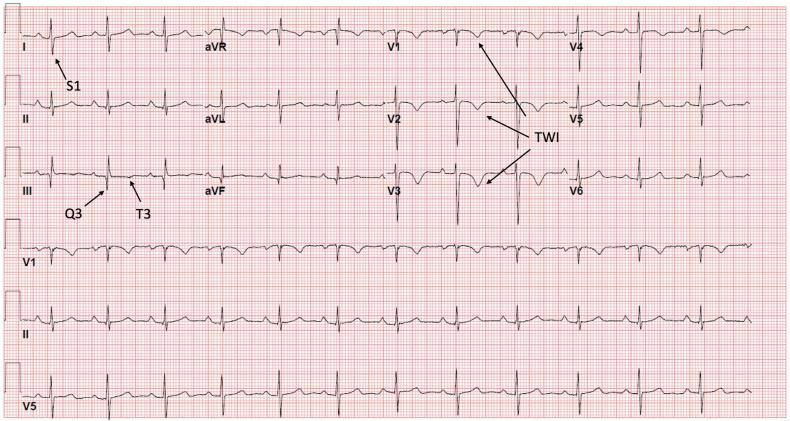
8. 🫀 Pulmonary Embolism (PE)
- Sinus tachycardia — most common finding
- S1Q3T3 pattern: Deep S wave in lead I + Q wave in lead III + T-wave inversion in lead III (McGinn-White sign)
- Right bundle branch block (complete or incomplete) — right ventricular strain
- T-wave inversions in V1–V4 — right heart strain
- Right axis deviation
- P pulmonale (tall peaked P in II >2.5 mm) in massive PE
- Atrial fibrillation may be precipitated

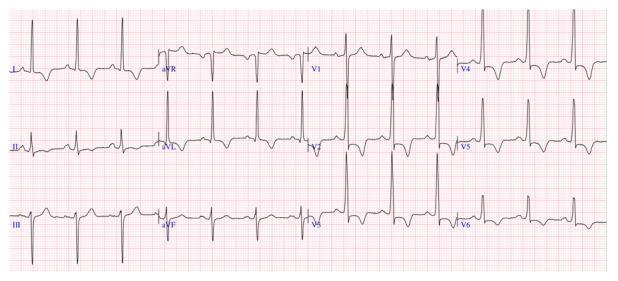
9. 🫀 Wolff-Parkinson-White (WPW) Syndrome
- Short PR interval <120 ms (bypasses AV node via accessory pathway)
- Delta wave — slurred, slow upstroke at the start of the QRS (signature finding)
- Wide QRS >120 ms (due to pre-excitation + delta wave)
- Secondary ST-T wave changes (discordant to QRS)
- "Pseudo-infarction" pattern — negative delta waves mimic pathological Q waves in inferior leads
- Accessory pathway location can be estimated from delta wave polarity:
- Positive delta in V1 → left-sided pathway
- Negative delta in inferior leads → posteroseptal pathway

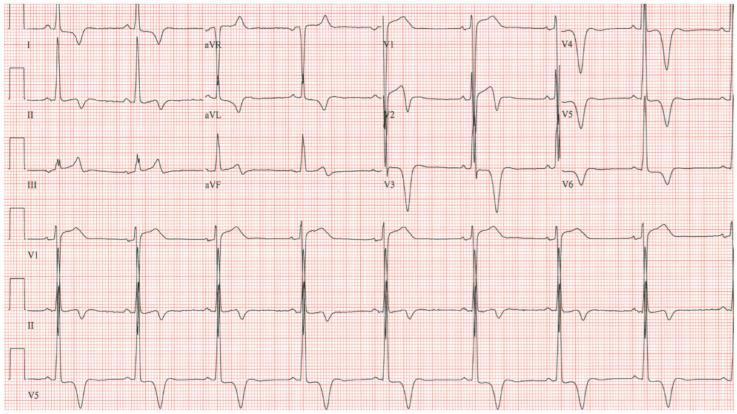
10. 🫀 Hypertrophic Cardiomyopathy (HCM)
- High-voltage LVH pattern — Sokolow-Lyon ≥35 mm
- Deep, narrow "dagger-like" Q waves in lateral (I, aVL, V5–V6) and inferior (II, III, aVF) leads — due to septal hypertrophy
- Giant T-wave inversions in V3–V5 — especially in apical HCM (Yamaguchi syndrome, inversions >10 mm)
- ST-segment depression (strain pattern) in lateral leads
- Atrial fibrillation — common complication
- Left axis deviation and prolonged QRS in advanced cases
- Absence of septal Q waves can occur in severe septal HCM
Quick Reference Summary Table
| # | Disease | Key ECG Finding | Rate/Rhythm |
|---|---|---|---|
| 1 | STEMI | ST elevation (convex) + Q waves | Sinus, varies |
| 2 | NSTEMI/UA | ST depression + T inversion | Sinus |
| 3 | Atrial Fibrillation | No P waves, irregular RR | Irregular 100–180 |
| 4 | Ventricular Tachycardia | Wide QRS + AV dissociation | Regular 100–250 |
| 5 | AV Heart Block | PR prolonged / dropped QRS / AV dissociation | Slow |
| 6 | LVH | High voltage + strain pattern | Sinus |
| 7 | Pericarditis | Diffuse concave ST elevation + PR depression | Sinus, ±tachycardia |
| 8 | Pulmonary Embolism | S1Q3T3 + RBBB + sinus tachycardia | Sinus tachycardia |
| 9 | WPW Syndrome | Short PR + delta wave + wide QRS | Sinus ±tachycardia |
| 10 | HCM | Deep Q waves + giant T inversions + LVH | Sinus, ±AF |
Source: Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine; ROSEN's Emergency Medicine: Concepts and Clinical Practice
Make a Powerpoint presentation on CVA with appropriate images
ischemic stroke brain CT scan infarction
hemorrhagic stroke intracerebral hemorrhage CT brain
stroke FAST symptoms face arm speech time
stroke risk factors hypertension atherosclerosis
thrombolysis tPA stroke treatment management
cerebral artery anatomy MCA ACA PCA brain blood supply
stroke rehabilitation physiotherapy neurological recovery
stroke complications dysphagia hemiplegia aphasia
node /home/daytona/skills/shared/scripts/fetch_images.js \ "https://cdn.orris.…