Dysarthragia and difficulty waking disease
Reading File
Finding Sources
Finding Sources
Searching PubMed
dysarthria hypersomnia neurological disease
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching PubMed
"Kleine-Levin syndrome" treatment
Reading File
Finding Sources
Loading Image
Searching the Web
dysarthria difficulty waking hypersomnia neurological diagnosis differential
I now have comprehensive material to provide a thorough answer. Here is the full response:
Dysarthria + Difficulty Waking: Clinical Overview
The combination of dysarthria (impaired speech motor execution) and difficulty waking / excessive sleepiness (hypersomnia) is a classic pairing in several neurological and neuromuscular diseases. Here is the structured differential:
1. Myotonic Dystrophy (Type 1 and Type 2) - The Key Neuromuscular Cause
This is one of the most important diagnoses where both features are intrinsic to the disease, not coincidental.
Dysarthria arises from palatal, pharyngeal, and tongue muscle weakness. The "hatchet face" appearance (temporalis and masseter atrophy), nasal or slurred speech, and dysphagia are hallmarks.
Hypersomnia is a recognized systemic manifestation - listed explicitly alongside cataracts, gonadal atrophy, insulin resistance, and cardiac conduction disease.
"Palatal, pharyngeal, and tongue involvement can lead to dysarthria and dysphagia... Other associated features include intellectual impairment, hypersomnia, posterior subcapsular cataracts, gonadal atrophy, insulin resistance..."
- Harrison's Principles of Internal Medicine 22E, p. 2232
Both DM1 (classic form) and DM2/PROMM share these features. The hypersomnia in myotonic dystrophy is thought to have a central origin (CNS involvement), not purely explained by respiratory muscle weakness alone, though sleep-disordered breathing contributes.
Key exam findings: Grip myotonia (delayed relaxation after handshake), percussion myotonia of thenar eminence, frontal baldness, cataracts.
2. Kleine-Levin Syndrome (KLS) - The Episodic Hypersomnia Syndrome
KLS is the prototypical recurrent hypersomnia, primarily affecting adolescent males. Dysarthria is not a core feature of KLS itself, but the "difficulty waking" component is extreme and pathognomonic.
Clinical features:
- Episodic hypersomnia: patients sleep 16-18+ hours per day for days to weeks, waking only to eat and toilet
- Megaphagia / hyperphagia - compulsive overeating during brief awakenings
- Behavioral changes: social withdrawal, confusion, memory disturbance, hypersexuality, hallucinations
- Between episodes: completely normal cognition and behavior
- Predominantly adolescent males; onset late teens to mid-20s
- ICSD-III requires at least 2 episodes lasting 2 days to 5 weeks, occurring >once/year
"For days or weeks, the patients, mostly adolescent boys, sleep 18 h or more a day, awakening only long enough to eat and attend to toilet needs. They appeared dull, often confused, and restless..."
- Adams and Victor's Principles of Neurology, 12th Ed.
Pathophysiology: Limbic-hypothalamic dysfunction. SPECT imaging during episodes shows hypoperfusion of bilateral thalami, hypothalamus, frontal and temporal lobes (see image below).
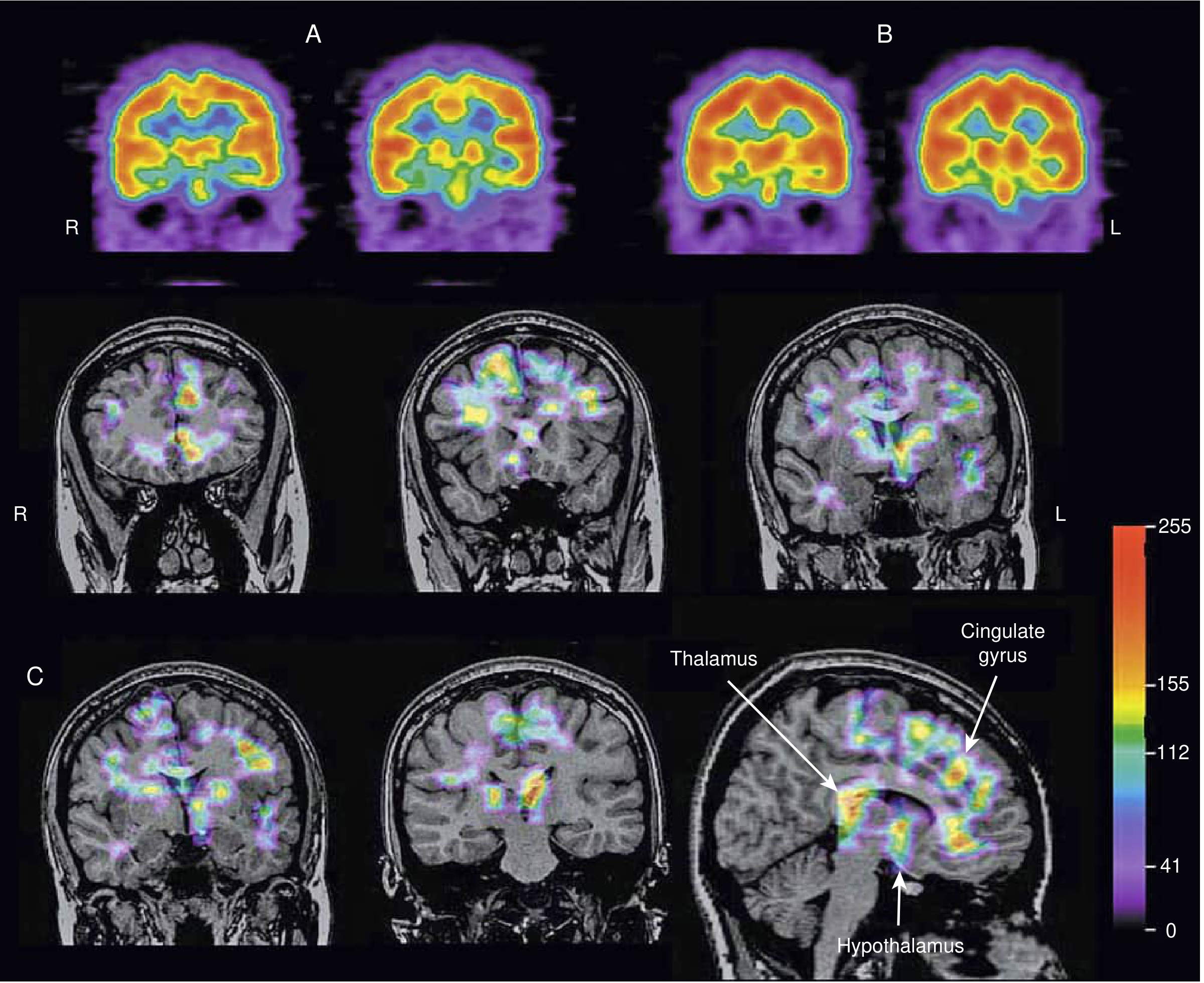
SPECT images in KLS: (A) Active episode - hypoperfusion in bilateral frontal, temporal, and diencephalic structures. (B) Convalescent phase - recovery of perfusion. (C) Subtraction image showing bilateral thalami, hypothalamus, and frontal regions most affected. - Bradley and Daroff's Neurology in Clinical Practice
Treatment: No consistently proven therapy. Lithium has tentative evidence from an open-label trial to reduce relapse rate and episode duration. Stimulants (modafinil, amphetamines) used for the sleepiness. Clarithromycin and flumazenil have been reported in case series.
3. Brainstem Lesions (Stroke, Tumor, Demyelination)
Lesions of the brainstem (pons, medulla, midbrain) can simultaneously impair:
- Dysarthria - through disruption of corticobulbar tracts or cerebellar-brainstem connections
- Consciousness/arousal - through disruption of the ascending reticular activating system (ARAS)
Causes: Pontine infarcts, posterior fossa tumors (astrocytomas, lymphomas, hamartomas of the posterior hypothalamus), multiple sclerosis plaques, central pontine myelinolysis.
A classic syndrome is the "locked-in syndrome" (basilar artery occlusion) - though that is an extreme. More subtle brainstem strokes cause dysarthria + lethargy/hypersomnia.
"Focal neurological lesions may also cause excessive sleepiness. For example, lesions of the brainstem, thalamus, hypothalamus, and periaqueductal region..."
- Bradley and Daroff's Neurology in Clinical Practice
4. Idiopathic Hypersomnia (IH) - "Sleep Drunkenness"
IH features profound "sleep inertia" (prolonged difficulty waking, also called sleep drunkenness) as its most characteristic symptom. Dysarthria is not a primary feature but can manifest during the severe sleep inertia phase as slurred, confused speech.
Key features:
- Chronic excessive daytime sleepiness despite adequate or prolonged nighttime sleep
- Unrefreshing naps (unlike narcolepsy, where naps ARE refreshing)
- Severe difficulty waking from both nighttime sleep and naps
- Cognitive dysfunction ("brain fog")
- Possible GABAergic mechanism (some patients respond to clarithromycin or flumazenil)
5. Secondary / Symptomatic Narcolepsy
Hypothalamic lesions (tumors, sarcoidosis, neuromyelitis optica) can destroy hypocretin (orexin)-producing cells, causing narcolepsy with cataplexy. These lesions can also cause dysarthria if they extend or compress adjacent structures.
6. Wilson's Disease
Though not prominently linked above from this search, Wilson's disease (hepatolenticular degeneration - copper accumulation) is a classic cause of:
- Dysarthria - scanning/slurred speech from basal ganglia and cerebellar involvement
- Neuropsychiatric features including hypersomnia and personality change
Age of onset: typically 5-35 years. Look for Kayser-Fleischer rings, liver disease, psychiatric symptoms.
Differential Summary Table
| Condition | Dysarthria Type | Sleep/Waking Problem | Key Distinguishing Feature |
|---|---|---|---|
| Myotonic Dystrophy (DM1/DM2) | Bulbar/nasal | Hypersomnia (central) | Myotonia, hatchet face, cataracts, ECG changes |
| Kleine-Levin Syndrome | Not typical (confusion/slurring during episodes) | Episodic hypersomnolence 16-18h/day | Episodes with megaphagia, hypersexuality; normalcy between |
| Idiopathic Hypersomnia | Not primary; slurred during sleep inertia | Severe sleep inertia, difficulty waking | Chronic, no episodes, unrefreshing naps |
| Brainstem Stroke/Lesion | Dysarthria prominent | Arousal deficit / lethargy | Focal signs, acute onset, imaging |
| Wilson's Disease | Dysarthria from basal ganglia | Hypersomnia, behavioral change | KF rings, liver disease, copper studies |
| Obstructive Sleep Apnea | Dysarthria rare | Hypersomnia, difficult morning waking | Snoring, obesity, witnessed apneas |
Approach to Investigation
- History: Age, episodic vs. chronic, associated megaphagia/hypersexuality (KLS), family history of myotonia (DM1/DM2), psychiatric change (Wilson's), snoring (OSA)
- Examination: Myotonia testing (grip release, percussion), Kayser-Fleischer rings on slit lamp, bulbar signs, cerebellar signs
- Investigations:
- EMG/NCS + muscle biopsy - myotonic dystrophy
- Brain MRI (especially brainstem and diencephalon)
- Polysomnography + MSLT - narcolepsy, IH, KLS
- Serum ceruloplasmin, 24-h urine copper - Wilson's disease
- Genetic testing (DMPK gene repeat expansion) - DM1
- SPECT during symptomatic phase - KLS
Recent evidence note: A 2023 review by Arnulf et al. on KLS (PMID 37684104) and a 2025 update on central disorders of hypersomnolence PMID 40533080 continue to show no definitive pathophysiological mechanism for KLS and no high-evidence pharmacotherapy established beyond lithium's role in relapse reduction.
This is a shared conversation. Sign in to Orris to start your own chat.