Fever with rash? I need to know about the types and differential diagnosis
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Searching the Web
fever with rash differential diagnosis classification 2024 2025
I now have comprehensive material from Harrison's 22nd Edition (2025), Goldman-Cecil Medicine, and multiple supporting textbooks. Let me compile the full, detailed answer.
Fever with Rash - Types and Differential Diagnosis
The combination of fever and rash is a common and sometimes life-threatening clinical presentation. The key to differential diagnosis is rash morphology - identifying lesion type first, then distribution, then temporal features. Below is a systematic breakdown based on Harrison's Principles of Internal Medicine 22nd Ed. (2025) and Goldman-Cecil Medicine.
Approach to the Patient
A thorough history must cover:
-
Immune status and medications taken in the past month
-
Travel history, immunization status
-
Animal/arthropod bite exposure
-
Recent dietary exposures and sick contacts
-
Sexual history
-
Site of rash onset and direction/rate of spread
-
Harrison's Principles of Internal Medicine 22E, p. 181
Lesion Morphology - Definitions
| Term | Definition |
|---|---|
| Macule | Flat area of changed color (blanchable erythema) |
| Papule | Raised solid lesion <5 mm |
| Plaque | Raised flat-topped lesion >5 mm |
| Vesicle | Fluid-filled <5 mm |
| Bulla | Fluid-filled >5 mm |
| Pustule | Raised lesion with purulent exudate |
| Petechiae | Flat, non-blanchable purpura <3 mm (bleeding into skin) |
| Ecchymosis | Non-blanchable purpura >3 mm |
| Palpable purpura | Raised, non-blanchable - indicates vasculitis |
| Eschar (tâche noire) | Necrotic lesion covered with a black crust |
| Wheal/urticaria | Pale pink papule/plaque, transient (<24 h per area) |
Classification by Rash Type + Key Differentials
1. Centrally Distributed Maculopapular Eruptions (Most Common)
Lesions are primarily truncal.
| Disease | Key Features |
|---|---|
| Measles (Rubeola) | Rash starts at hairline D2-3, spreads downward; confluent; Koplik's spots (pathognomonic - white/blue lesions with erythematous halo on buccal mucosa) |
| Rubella (German measles) | Starts at hairline, clears from originally affected areas as it spreads; may be pruritic; Forchheimer spots (palatal petechiae); post-auricular adenopathy |
| Enteroviruses (echo/coxsackie) | Non-specific; may mimic rubella/measles |
| Infectious mononucleosis (EBV) | Maculopapular rash; classically worsened/precipitated by ampicillin/amoxicillin |
| Primary HIV infection | Maculopapular rash; concurrent pharyngitis, lymphadenopathy |
| Epidemic/Endemic typhus (Rickettsia) | Starts centrally, spreads; epidemic typhus in war/disaster settings; endemic typhus in urban rodent areas |
| Leptospirosis | Urban rodent exposure |
| Typhoid fever (rose spots) | Rose spots on trunk; travel history to endemic areas |
| Dengue fever | Mosquito-borne; tropical/subtropical travel; "islands of white in a sea of red" |
| Lyme disease (erythema migrans) | Single/multiple annular lesions - pathognomonic; may persist >1 year if untreated |
| Erythema marginatum | Acute rheumatic fever; enlarging and shifting transient annular lesions |
| SLE (malar rash) | Butterfly distribution on cheeks; sharply defined |
| Still's disease | Evanescent salmon-colored rash on trunk + proximal extremities; coincides with fever spikes |
| Zika virus | Pruritic; conjunctival injection; risk to pregnant women (microcephaly) |
| Hemophagocytic lymphohistiocytosis (HLH) | Protean - erythematous maculopapular, pyoderma gangrenosum, purpura, or panniculitis |
- Harrison's Principles of Internal Medicine 22E, pp. 181-189
2. Peripheral Eruptions
Rashes are most prominent peripherally (acral areas) and may spread centripetally. Early treatment is critical.
| Disease | Key Features |
|---|---|
| Rocky Mountain spotted fever (RMSF) - R. rickettsii | Begins on wrists and ankles, spreads centripetally including palms/soles; petechial evolution; tick bite history; can be life-threatening if untreated |
| Secondary syphilis | Copper-colored papulosquamous rash involving palms and soles; condyloma lata; lymphadenopathy |
| Hand-foot-mouth disease (Coxsackie A16, EV71) | Vesicular lesions on palms, soles, and oral mucosa; children |
| Rat bite fever (Streptobacillus) | Peripheral distribution; history of rat bite |
| Infective endocarditis | Osler nodes (tender, subcutaneous - fingertips), Janeway lesions (non-tender - palms/soles), splinter hemorrhages |
| Reactive arthritis (Reiter's) | Keratoderma blennorrhagica on palms/soles; circinate balanitis |
3. Confluent Desquamative Erythematous Eruptions ("Sunburn-like")
Diffuse erythema followed by desquamation.
| Disease | Key Features |
|---|---|
| Scarlet fever (S. pyogenes) | "Sandpaper" texture; pastia lines (linear petechiae in skin folds); circumoral pallor; strawberry tongue; streptococcal pharyngitis |
| Toxic shock syndrome (TSS) - S. aureus or S. pyogenes | Diffuse erythroderma; hypotension; multiorgan failure; tampon use / wound history |
| Kawasaki disease | Children <5y; conjunctival injection; lip cracking; strawberry tongue; cervical adenopathy; coronary artery aneurysm risk |
| Staphylococcal scalded skin syndrome (SSSS) | Neonates/young children; bullous separation at epidermis; Nikolsky sign positive |
| Drug hypersensitivity / DRESS | Drug history; eosinophilia; systemic organ involvement |
4. Vesiculobullous Eruptions
Fluid-filled lesions predominate.
| Disease | Key Features |
|---|---|
| Varicella (chickenpox) | "Dewdrop on a rose petal" lesions; all stages simultaneously; centripetal distribution |
| Herpes zoster | Dermatomal distribution; reactivation in immunocompromised/elderly |
| Herpes simplex | Grouped vesicles on erythematous base; oral or genital |
| Stevens-Johnson Syndrome / TEN | Drug reaction; targetoid lesions; mucosal involvement; Nikolsky sign; high mortality in TEN |
| Bullous pemphigoid / Pemphigus | Autoimmune; tense vs. flaccid bullae |
| Smallpox / Monkeypox | Synchronous lesion stages (vs. chickenpox); centrifugal; travel/exposure history |
| Rickettsialpox | Eschar at bite site; vesicular rash; R. akari |
| Hand-foot-mouth disease | (see peripheral above) |
5. Urticaria-like Eruptions
Wheals and hives, sometimes with angioedema.
| Disease | Key Features |
|---|---|
| Serum sickness / drug reaction | Drug or foreign protein exposure; arthralgia |
| Urticarial vasculitis | Lesions last >24 h (unlike true urticaria); burning rather than itch |
| Hereditary angioedema | C1-esterase inhibitor deficiency; swelling without rash |
| Early meningococcemia | Can initially appear urticarial before becoming petechial |
| Viral infections | EBV, hepatitis B, enteroviruses |
6. Nodular Eruptions
| Disease | Key Features |
|---|---|
| Disseminated fungal infection (Candida, Cryptococcus, Histoplasma) | Immunocompromised; umbilicated papulonodules |
| Erythema nodosum | Tender nodules on shins; associated with TB, sarcoid, strep, IBD, drugs |
| Sweet syndrome (acute febrile neutrophilic dermatosis) | Tender red plaques; neutrophilia; associated with hematologic malignancy or IBD |
| Kaposi's sarcoma | HIV/AIDS; violaceous nodules |
| Bacillary angiomatosis (Bartonella) | HIV; resembles Kaposi |
7. Purpuric Eruptions (Non-blanchable)
These can be life-threatening - always assess urgently.
| Disease | Key Features |
|---|---|
| Meningococcemia (N. meningitidis) | Rapidly progressive petechiae → purpura in children; meningismus; sepsis; medical emergency |
| Rocky Mountain spotted fever | (see peripheral; purpura in late stage) |
| Purpura fulminans | DIC; associated with meningococcemia, streptococcal/staphylococcal sepsis |
| Infective endocarditis | Petechiae, splinter hemorrhages, Osler nodes |
| Henoch-Schönlein Purpura (IgA vasculitis) | Children; palpable purpura on buttocks/legs; arthralgia, abdominal pain, nephritis |
| Thrombocytopenic purpura (ITP/TTP) | Platelet destruction; may have no fever unless secondary |
| Echovirus 9 | Viral; may mimic meningococcemia |
| Rickettsial diseases | RMSF, epidemic typhus (severe) |
| Drug-induced vasculitis | ANCA-associated; palpable purpura |
8. Eruptions with Eschars
Necrotic lesion + black crust = eschar (tâche noire) - pathognomonic for tick/mite-borne rickettsioses.
| Disease | Key Features |
|---|---|
| Scrub typhus (Orientia tsutsugamushi) | Single eschar at mite bite site; SE Asia/Pacific |
| Rickettsia africae / boutonneuse fever | Multiple eschars possible |
| Anthrax | Painless black eschar; edema; bioterrorism consideration |
| Tularemia | Ulcer + regional adenopathy (ulceroglandular form) |
| Cutaneous leishmaniasis | Ulcer with raised indurated edge |
| Ecthyma gangrenosum | P. aeruginosa sepsis; immunocompromised |
Summary Table: Quick Differential by Morphology
| Morphology | Infectious (Treatable) | Viral/Other Infectious | Non-infectious |
|---|---|---|---|
| Petechial/Purpuric | Meningococcemia, RMSF, endocarditis, epidemic typhus | Enteroviruses, EBV, CMV, dengue | HSP/IgA vasculitis, TTP, drug reaction, DRESS |
| Maculopapular | Typhoid, Lyme, HIV, syphilis, RMSF (early), ehrlichiosis | Measles, rubella, EBV, dengue, parvovirus B19, roseola (HHV-6), Zika | SLE, Still's disease, drug reaction, erythema multiforme, serum sickness |
| Vesicular/Bullous | Herpes simplex, herpes zoster, S. aureus | Varicella, monkeypox, smallpox | SJS/TEN, bullous pemphigoid, contact dermatitis |
| Confluent desquamative | Scarlet fever, TSS, SSSS | - | Kawasaki, drug hypersensitivity |
| Nodular | Disseminated fungals, bacillary angiomatosis | - | Erythema nodosum, Sweet syndrome |
| Eschar | Scrub typhus, RMSF, anthrax, tularemia | - | - |
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 21; Goldman-Cecil Medicine Table 259-2
Red Flags Requiring Immediate Action
The following presentations demand urgent workup and empiric treatment:
- Petechial/purpuric rash + fever - rule out meningococcemia; give ceftriaxone before LP if septic
- Peripheral petechiae spreading centripetally - rule out RMSF; start doxycycline empirically
- Diffuse erythroderma + hypotension - toxic shock syndrome
- Eschar + fever + travel to Asia - scrub typhus
- Bullous eruption + mucosal involvement - SJS/TEN (stop all suspect drugs immediately)
- Fever + rash + immunocompromised host - broad differential including fungi, atypical organisms
Key Diagnostic Mnemonic: "VIRUS"
A useful clinical memory aid for common exanthems in children:
- Varicella (chickenpox)
- Infectious mononucleosis (EBV)
- Rubella (German measles) / Roseola (HHV-6)
- Urticarial drug reaction
- Scarlet fever / Secondary syphilis
Primary sources: Harrison's Principles of Internal Medicine 22E (2025), Chapter 21 "Fever and Rash" (Kaye & Kaye); Goldman-Cecil Medicine, Table 259-2; Fitzpatrick's Dermatology; Tintinalli's Emergency Medicine
A 55yr old male patient presented to the opd with the history of fever since 4days and also complaints of rash since yesterday.
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
I now have everything I need to build a thorough, case-focused clinical analysis. Let me compile the full response.
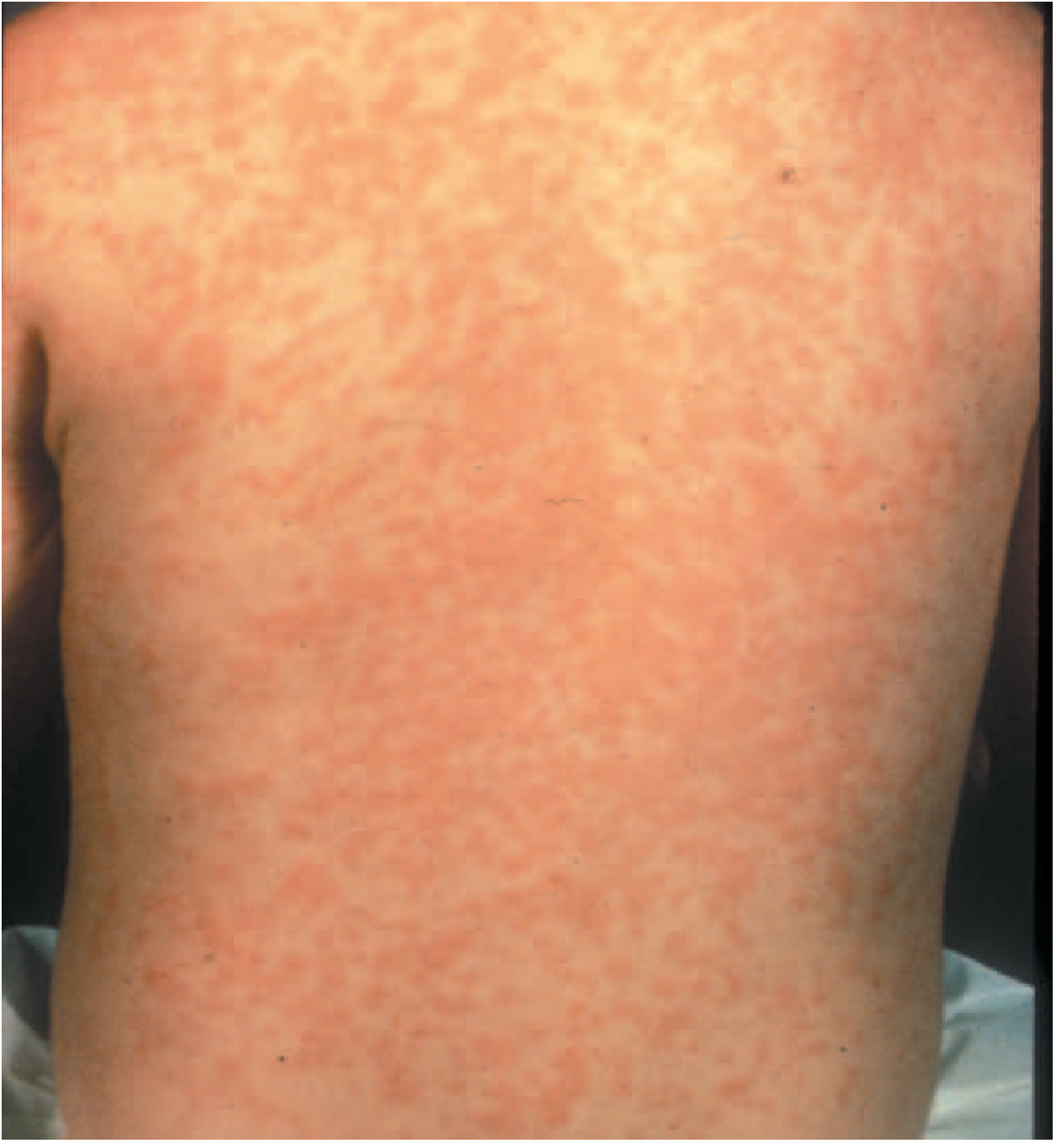
Clinical Case Analysis: 55-Year-Old Male, Fever ×4 Days + Peripheral Maculopapular Rash ×1 Day
Clinical Summary
- Age/Sex: 55-year-old male
- Fever: 4 days (rash appeared on day 4 - "fever then rash" pattern)
- Rash type: Maculopapular
- Distribution: Peripheral (wrists, ankles, hands, feet, face)
The "fever first, rash later" pattern is diagnostically important - the 4-day prodrome of fever before rash appearance is characteristic of several specific entities. The peripheral distribution narrows the differential considerably.
Priority Diagnoses (Most to Least Urgent)
🔴 1. Rocky Mountain Spotted Fever (RMSF) - R. rickettsii
Must rule out first. Potentially fatal if untreated.
- Rash begins on wrists and ankles, spreads centripetally
- Initially erythematous macules → evolves to maculopapular → petechial over days
- Palms and soles involved later in disease
- Fever precedes rash by 2-4 days (matches this case exactly)
- Tick bite history (often not recalled); outdoor exposure
- Associated: severe headache, myalgias, nausea, occasionally confusion
- Do not wait for rash to become petechial before treating - start doxycycline empirically
- Harrison's Principles of Internal Medicine 22E, Chapter 21
🔴 2. Dengue Fever
Very common in tropical/subtropical regions. Age >65 and comorbidities = higher mortality risk.
-
Fever 4-7 days, then maculopapular rash appears on days 3-5 - highly consistent with this presentation
-
"Islands of white in a sea of red" - characteristic appearance
-
Classic triad: high fever, severe headache ("break-bone fever"), retro-orbital pain + myalgia/arthralgia
-
Rash may begin peripherally and spread to trunk
-
Look for: thrombocytopenia, leukopenia, raised hematocrit, positive tourniquet test
-
Risk: dengue hemorrhagic fever in those >65, diabetics, or with cardiopulmonary disease
-
Rosen's Emergency Medicine; Goldman-Cecil Medicine
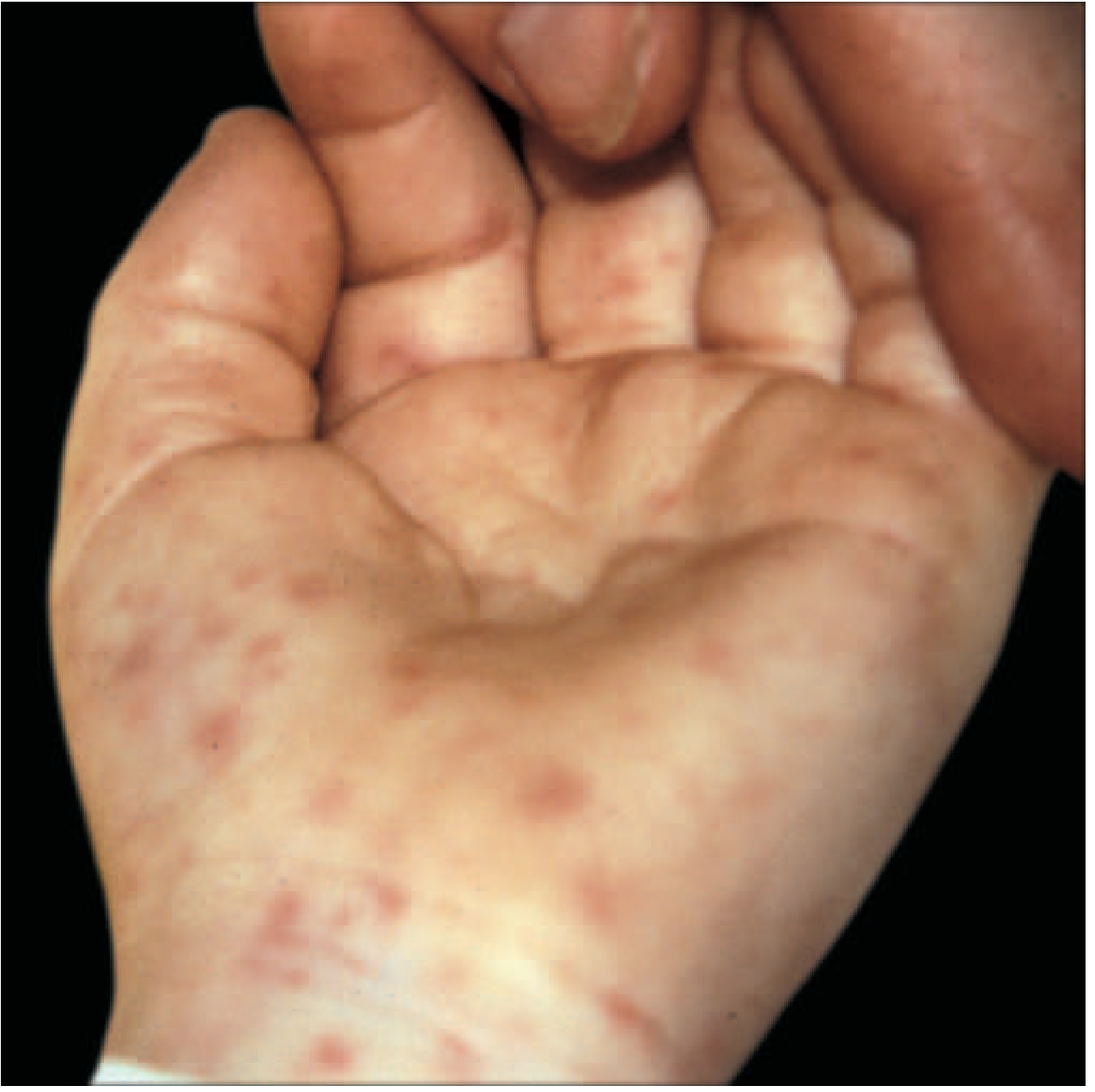
🟡 3. Secondary Syphilis
Classic peripheral maculopapular rash - always consider in adults.
-
Rash characteristically involves palms and soles - highly specific
-
Maculopapular, copper-colored
-
Fever + malaise common
-
May be pruritic or non-pruritic
-
Look for: mucous patches, condylomata lata, generalized lymphadenopathy
-
History: sexual exposure 3-5 months prior (primary chancre may have been missed/painless)
-
Diagnosis: RPR/VDRL → confirm with TPPA/FTA-ABS
-
Harrison's 22E; Tintinalli's Emergency Medicine
🟡 4. Scrub Typhus - Orientia tsutsugamushi
Extremely common in South/Southeast Asia. Often missed.
- Fever 5-14 days, then maculopapular rash appears on trunk → spreads peripherally
- Pathognomonic eschar (tâche noire) at mite bite site - check hairline, axilla, groin, behind ears
- Headache, lymphadenopathy, hepatosplenomegaly
- Age 55 in a rural/forested setting = high suspicion
- Diagnosis: Weil-Felix (OX-K positive, low sensitivity), IFA, PCR
- Treatment: doxycycline
🟡 5. Typhoid Fever (Enteric Fever) - Salmonella typhi
Rose spots: faint salmon-colored macules on trunk - may initially appear peripherally.
-
Fever builds over days 1-4 (step-ladder pattern) - matches this case
-
"Rose spots" appear in ~30% of patients - faint, blanchable, salmon-colored, 2-4mm
-
Relative bradycardia at peak fever (pulse-temperature dissociation)
-
Constipation early, diarrhea later; abdominal pain; hepatosplenomegaly
-
Travel to endemic areas (South Asia, Sub-Saharan Africa)
-
Diagnosis: blood culture (gold standard), Widal test (low specificity)
-
Harrison's 22E; Sherris & Ryan's Medical Microbiology 8E
🟡 6. Chikungunya Fever
Common in tropics; easily confused with dengue.
-
Mosquito-borne flavivirus
-
Maculopapular rash within first 5 days of fever - consistent with this case
-
Hallmark: severe debilitating polyarticular arthralgia (small joints) - persists weeks to months
-
Clinically similar to dengue but arthralgia is more prominent and hemorrhagic complications less common
-
Diagnosis: PCR (acute phase), IgM serology
-
Goldman-Cecil Medicine, Chapter on Post-Travel Care
🟢 7. Infectious Mononucleosis (EBV)
Less likely at 55, but not impossible.
- Maculopapular rash + fever + pharyngitis + lymphadenopathy (classic triad)
- Rash dramatically worsens if given ampicillin/amoxicillin
- Hepatosplenomegaly common
- Check: atypical lymphocytes on peripheral smear, heterophile antibody (Monospot), EBV serology
🟢 8. Drug Reaction / DRESS
Always consider in a 55-year-old likely on medications.
- Drug started within last 2-8 weeks (can be delayed)
- DRESS: Drug Reaction with Eosinophilia and Systemic Symptoms
- Maculopapular rash, fever, facial edema, lymphadenopathy, liver/kidney involvement
- Common culprits: allopurinol, anticonvulsants (carbamazepine, phenytoin), sulfonamides, dapsone
- Eosinophilia on CBC is a key clue
🟢 9. Lyme Disease (Erythema Migrans)
If rash is annular/target-shaped rather than discrete macules.
- Single or multiple annular "bulls-eye" lesions - pathognomonic
- Tick bite (usually Ixodes); endemic areas
- Associated: arthralgia, fatigue, cranial nerve palsy (Bell's palsy), AV block
- Note: erythema migrans is typically a single expanding lesion, not a peripheral scattered rash
🟢 10. Erythema Multiforme
If targetoid lesions are noted.
- Symmetric target/iris lesions on elbows, knees, palms, soles, face
- Triggered by HSV (most common), Mycoplasma, drugs
- Fever and malaise common
- Mucosal involvement = Stevens-Johnson spectrum (check for oral/ocular lesions)
Systematic Approach: History Questions to Ask NOW
| Question | Why It Matters |
|---|---|
| Any recent travel (especially tropical)? | Dengue, chikungunya, typhoid, scrub typhus |
| Tick/insect bite noticed? | RMSF, Lyme, scrub typhus |
| Outdoor/forest exposure? | Rickettsial diseases |
| Sexual history/new partner? | Secondary syphilis |
| Medications started in last 2 months? | DRESS, drug reaction |
| Arthralgia/joint pain? | Chikungunya, dengue, Lyme |
| Retro-orbital pain, bone pain? | Dengue |
| Eschar anywhere on body? | Scrub typhus |
| Abdominal symptoms? | Typhoid |
| Throat pain, lymph node swelling? | EBV, scarlet fever |
| Bradycardia despite fever? | Typhoid (relative bradycardia) |
Investigations to Order (First-Line)
| Investigation | Rationale |
|---|---|
| CBC with differential | Leukopenia (dengue, typhoid), thrombocytopenia (dengue, RMSF), eosinophilia (DRESS), atypical lymphocytes (EBV) |
| Blood culture (×2, aerobic) | Typhoid, bacteremia |
| Liver function tests | Dengue, EBV, typhoid, DRESS |
| Dengue NS1 antigen + IgM/IgG serology | Dengue (within first 5 days: NS1 is positive) |
| RPR/VDRL | Secondary syphilis |
| Weil-Felix (OXK) + scrub typhus IgM (ELISA/IFA) | Scrub typhus (endemic regions) |
| Rickettsial serology / PCR | RMSF if clinically suspected |
| Widal test / Typhoid IgM | Typhoid (after day 5-7) |
| Chikungunya PCR / IgM | Chikungunya |
| EBV serology (Monospot, VCA IgM) | EBV |
| Peripheral blood smear | Malaria, atypical lymphocytes |
| Coagulation profile | If hemorrhagic features develop |
| Skin biopsy (fresh lesion) | If diagnosis unclear after above |
Clinical Decision Framework
Peripheral maculopapular rash + 4 days fever
|
├── Tick bite / outdoor exposure?
│ ├── YES → RMSF (start doxycycline empirically, don't wait for labs)
│ └── Scrub typhus (check for eschar)
│
├── Tropical travel / mosquito exposure?
│ ├── Dengue (NS1, CBC, thrombocytopenia)
│ └── Chikungunya (prominent arthralgia?)
│
├── Palms/soles prominently involved?
│ └── Secondary syphilis (RPR, sexual history)
│
├── Step-ladder fever + relative bradycardia?
│ └── Typhoid (blood culture)
│
├── Recent medications?
│ └── DRESS / drug reaction (eosinophilia, liver enzymes)
│
└── Pharyngitis + lymphadenopathy?
└── EBV (Monospot, atypical lymphocytes)
Red Flags to Watch For in This Patient
- Rash becoming petechial/non-blanchable - RMSF progression or meningococcemia - treat immediately
- Thrombocytopenia + rising hematocrit - dengue hemorrhagic fever
- Hypotension - septic shock; escalate care
- Mental status change - rickettsia, typhoid, dengue encephalopathy
- Facial edema + eosinophilia - DRESS syndrome - stop all suspect drugs immediately
Sources: Harrison's Principles of Internal Medicine 22E (2025), Chapter 21 "Fever and Rash"; Rosen's Emergency Medicine; Goldman-Cecil Medicine; Sherris & Ryan's Medical Microbiology 8E; Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.