Rifampicin drug in Orthopedics mechanism usage indication dosage side effects preventions everything in detail with appropriate images and diagrams
Reading File
Finding Sources
Finding Sources
Searching the Web
rifampicin orthopedics bone joint infection mechanism dosage side effects 2024
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
rifampicin prosthetic joint infection orthopedic implant
Finding Sources
Finding Sources
Searching PubMed
rifampin bone joint infection staphylococcal
Reading Web Page
https://www.contagionlive.com/view/the-role-of-rifampin-in-b…
Finding Sources
Finding Sources
Searching the Web
rifampicin chemical structure molecular diagram image pharmacology
Loading Image
Loading Image
Searching the Web
rifampicin RNA polymerase mechanism of action diagram bacterial inhibition
Loading Image
Loading Image
Searching the Web
rifampicin biofilm penetration orthopedic implant periprosthetic joint infection diagram image
Loading Image
Loading Image
Reading Web Page
https://www.mdpi.com/2079-6382/13/12/1223
Loading Image
Loading Image
I now have sufficient information to write a comprehensive, detailed answer. Let me compile everything.
Rifampicin (Rifampin) in Orthopedics - A Complete Guide
1. Drug Overview
Rifampicin (also spelled Rifampin; trade names: Rifadin, Rimactane, Rofact) is a semi-synthetic, broad-spectrum bactericidal antibiotic belonging to the rifamycin class. It was first derived from Amycolatopsis rifamycinica (formerly Streptomyces mediterranei) in Italy in 1965. In orthopedics, it holds a unique and irreplaceable role as an adjunctive agent in bone, joint, and implant-associated infections.
Chemical formula: C₄₃H₅₈N₄O₁₂
Molecular weight: 822.94 g/mol
Nature: Lipophilic, large macrolide-type ring structure
Chemical Structure
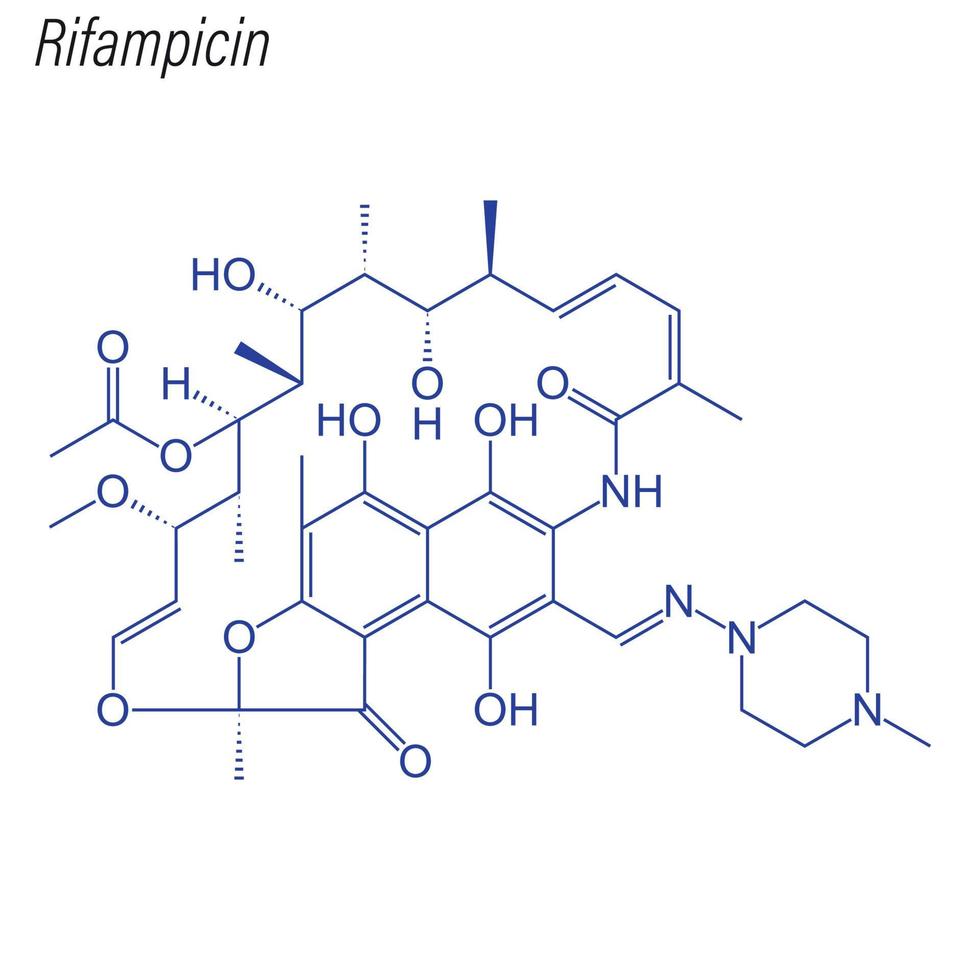
The structure features a large aliphatic ansa chain bridging positions 1 and 8 of a naphthalene core, with a piperazinyl group attached via an iminomethyl linkage - this piperazine addition distinguishes rifampicin from its parent rifamycin SV and is responsible for its superior oral bioavailability.
2. Mechanism of Action
Rifampicin exerts its bactericidal activity through a highly specific and unique mechanism.
Primary Mechanism: Inhibition of Bacterial RNA Polymerase (RNAP)
Rifampicin binds to the beta (β) subunit of bacterial DNA-dependent RNA polymerase (RNAP). This binding forms a stable drug-enzyme complex that physically blocks the elongation of RNA transcripts immediately after initiation - specifically, RNA chains longer than 2-3 nucleotides cannot form. The result: complete shutdown of mRNA synthesis, followed by failure of protein synthesis and bacterial death.
Target gene: rpoB (encodes the β subunit of RNAP)
Binding site: The rifampicin binding pocket (Rif pocket) is within the RNA polymerase cleft, adjacent to the active site.
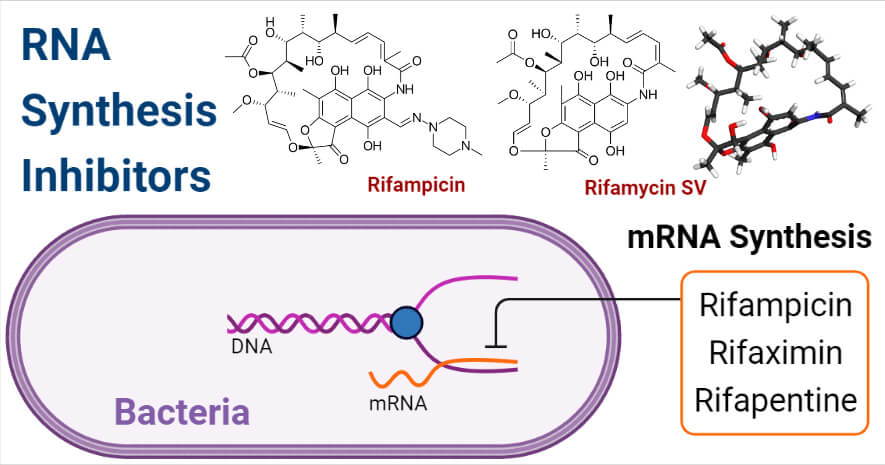
The diagram above shows how rifampicin blocks mRNA synthesis at the RNA polymerase level in bacteria, halting the transcription process entirely.
Key Properties Explaining Its Orthopedic Value
| Property | Clinical Relevance |
|---|---|
| Lipophilicity | Penetrates cell membranes, bone cortex, and biofilm matrix |
| Bactericidal vs. staphylococci | MIC ~0.06 µg/mL, kills even in biofilm context |
| Biofilm penetration | Diffuses into the extracellular polymeric substance (EPS) matrix of staphylococcal biofilms |
| Intracellular activity | Kills bacteria inside osteoblasts, macrophages, and leukocytes - bacteria hiding intracellularly evade most other antibiotics |
| Activity against dormant bacteria | Effective against slow-dividing or non-dividing bacteria (persisters), because it targets transcription, not cell wall synthesis |
| Concentration-dependent kill | Bactericidal activity is concentration dependent |
Why Biofilm is So Important in Orthopedics
Biofilm-forming organisms (primarily Staphylococcus aureus and S. epidermidis) attach to implant surfaces and secrete a polysaccharide-rich matrix. This matrix:
- Reduces antibiotic penetration by 10-1000x for most drugs
- Promotes bacterial quiescence (slow/no growth), reducing efficacy of cell-wall-active agents (beta-lactams, vancomycin)
- Triggers immune evasion
Rifampicin is one of the very few antibiotics that retains bactericidal activity within established biofilms, making it indispensable in implant-associated infections.
3. Pharmacokinetics
| Parameter | Value |
|---|---|
| Bioavailability (oral) | 90-95% fasting; reduced to ~50% with food |
| Peak plasma level | 7-10 µg/mL (600 mg dose) at ~2-4 hours |
| Volume of distribution | High - penetrates all tissues including bone, CSF, pleural fluid |
| Bone:plasma ratio | ~0.14 (AUC ratio) - recent PET/CT imaging in humans confirmed this |
| Protein binding | ~80% (albumin) |
| Metabolism | Hepatic; auto-induces CYP450 enzymes (CYP3A4, CYP2C9, P-glycoprotein) |
| Active metabolite | 25-desacetylrifampicin (retains antibacterial activity) |
| Half-life | 2-5 hours (can shorten to 1-2 hours with continued dosing due to auto-induction) |
| Elimination | Bile (primary, ~60-65%), urine (~30%) |
Important: High-dose rifampicin (e.g. 20-25 mg/kg/day) achieves significantly greater bone concentrations than standard dosing (10-15 mg/kg/day), with bone levels of 2 mg/L vs <0.2 mg/L respectively - a recent translational PET/CT imaging study demonstrated this directly in humans with confirmed S. aureus bone infections.
4. Orthopedic Indications
4.1 Periprosthetic Joint Infection (PJI) - PRIMARY INDICATION
This is the most important orthopedic use of rifampicin. PJI (infection around a total hip replacement, total knee replacement, shoulder replacement, etc.) involving staphylococci is treated with rifampicin-based combination therapy.
Clinical scenarios:
- Acute postoperative PJI (within 3 months of surgery) with stable implant - treated with DAIR (Debridement, Antibiotics, Implant Retention) + rifampicin combination
- Acute hematogenous PJI (sudden bacteremic seeding of a well-fixed implant) - DAIR + rifampicin
- Chronic PJI - exchange arthroplasty (one or two-stage) followed by rifampicin-based oral suppression therapy
Evidence: The landmark Zimmerli et al. RCT (NEJM 1998) showed ciprofloxacin + rifampicin vs ciprofloxacin + placebo for stable staphylococcal orthopedic device infections: 100% cure rate in ciprofloxacin-rifampicin arm vs 58% in placebo arm. This established the standard of care.
IDSA & EBJIS guidelines: Rifampicin is recommended in combination with fluoroquinolones or other agents for staphylococcal PJI managed with implant retention.
4.2 Fracture-Related Infection (FRI)
Infections following internal fixation of fractures (intramedullary nails, plates, screws). When hardware is retained for fracture healing, rifampicin is added to the antibiotic regimen for staphylococcal organisms, given the same biofilm concerns as PJI.
4.3 Osteomyelitis
- Acute hematogenous osteomyelitis with staphylococci - rifampicin added to beta-lactam or fluoroquinolone backbone, particularly in MRSA or in cases with hardware involvement
- Chronic osteomyelitis - especially useful in the oral phase after IV antibiotics, in combination with another active agent
- Diabetic foot osteomyelitis (DFO) - recent large VA observational study (n=6174) found adjunctive rifampicin significantly reduced mortality and amputation rates (OR 0.65, p=0.04) compared to antibiotics alone. The randomized VA INTREPID trial is currently ongoing.
- Vertebral osteomyelitis / Spondylodiscitis - rifampicin combination therapy in staphylococcal cases
4.4 Septic Arthritis with Hardware / Adjacent Implant
When septic arthritis occurs near a prosthetic joint or hardware, rifampicin is used adjunctively.
4.5 Osteoarticular Tuberculosis (Pott's Disease / TB Spine / TB Joints)
Rifampicin is a cornerstone first-line anti-TB drug in the standard HRZE regimen used for:
- Spinal tuberculosis (Pott's disease) - TB of the thoracic/lumbar vertebrae causing kyphotic deformity (gibbus)
- Tuberculous arthritis (hip, knee, elbow joints)
- Tuberculous osteomyelitis
Standard TB regimen used in skeletal TB:
- 2 months: Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E)
- 4-10 months continuation: Isoniazid (H) + Rifampicin (R)
- Total duration: 6-12 months (spinal TB may need 12 months)
4.6 Hemophilic Arthropathy - Synoviorthesis
An unusual niche use: intra-articular rifampicin injection has been used as a chemical synoviorthesis (synovial ablation) in hemophilic arthropathy, particularly when radioactive synoviorthesis is unavailable. Published series of 24 treated joints demonstrated good efficacy (noted in Campbell's Operative Orthopaedics 15th Ed).
5. Dosage and Administration
Oral (most common in orthopedic practice)
| Indication | Dose | Frequency | Duration |
|---|---|---|---|
| PJI (DAIR - staphylococci) | 450-600 mg (or 7.5-10 mg/kg) | Twice daily (BID) | 3-6 months (hip/knee); may extend |
| PJI - oral suppression phase | 300-450 mg | BID | Until combination completed |
| Osteomyelitis | 450-600 mg | BID | 6-12 weeks minimum |
| Spinal TB (adult) | 10 mg/kg/day (max 600 mg) | Once daily | 6-12 months |
| Diabetic Foot Osteomyelitis | 300-600 mg | BID | As per backbone antibiotic duration |
| Pediatric (TB / bone) | 10-20 mg/kg/day | Once daily | Per indication |
Golden rule: Rifampicin must NEVER be given as monotherapy in any indication. Resistance develops within 1-7 days of monotherapy due to single-step point mutations in rpoB. ALWAYS combine with at least one other active agent.
Preferred Combination Partners in Orthopedics
| Organism | Preferred Partner | Rationale |
|---|---|---|
| MSSA (methicillin-sensitive S. aureus) | Fluoroquinolone (ciprofloxacin/levofloxacin) or clindamycin | High oral bioavailability, good bone penetration |
| MRSA | Vancomycin + rifampicin (acute phase), then TMP-SMX or doxycycline + rifampicin (oral) | Vancomycin for IV phase; rifampicin carries oral phase |
| CoNS (coagulase-negative staph) | Fluoroquinolone or TMP-SMX | Per sensitivity |
| M. tuberculosis | INH + Rifampicin + PZA + Ethambutol | Standard HRZE backbone |
IV Formulation
Available as IV (rifampicin for infusion 600 mg); used when oral route unavailable. Must be given as slow infusion over 30-180 minutes. IV formulation now also used in some centers for severe osteoarticular infections during the initial phase.
6. Side Effects and Adverse Reactions
6.1 Characteristic / Unique Side Effects
Orange-red discoloration of body fluids (VERY COMMON)
- Urine, tears, saliva, sweat, sputum, CSF - all turn orange-red
- Harmless but alarming to patients if not warned
- Permanently stains soft contact lenses - patients must wear glasses during treatment
6.2 Gastrointestinal (Common, 3-10%)
- Nausea, vomiting, anorexia, abdominal cramps
- Diarrhea (occasionally severe)
- Usually dose-related and improves with time
6.3 Hepatotoxicity (Most Clinically Significant)
- Elevated transaminases: Occurs in up to 20% of patients; usually asymptomatic and transient
- Clinical hepatitis: 0.6-3% - more common when combined with isoniazid
- Fulminant hepatic failure: Rare (<0.1%) but fatal if unrecognized
- Risk factors: Pre-existing liver disease, alcoholism, elderly, concurrent hepatotoxic drugs
Monitoring: LFTs (ALT, AST, bilirubin) at baseline, 2 weeks, 4 weeks, then monthly. Stop if ALT >3x ULN with symptoms or >5x ULN asymptomatic.
6.4 Drug Interactions - Potent CYP Inducer (Most Important in Practice)
Rifampicin is one of the most potent inducers of hepatic cytochrome P450 enzymes (CYP3A4, CYP2C9, CYP2C8, CYP2C19) and P-glycoprotein. This dramatically reduces serum levels of co-administered drugs:
| Drug Class | Specific Drugs Affected | Clinical Consequence |
|---|---|---|
| Antiretrovirals (HIV) | Protease inhibitors, NNRTIs | Sub-therapeutic HIV levels - use rifabutin instead |
| Anticoagulants | Warfarin | Dramatically reduces INR - requires dose doubling+ with close monitoring |
| Oral contraceptives | Estrogen + progestins | Contraceptive failure - use barrier method |
| Antifungals | Fluconazole, voriconazole | Drastically reduced antifungal levels |
| Immunosuppressants | Cyclosporine, tacrolimus, sirolimus | Transplant rejection risk - critical interaction |
| Statins | Most statins | Reduced statin levels |
| Quinolones | Ciprofloxacin, moxifloxacin | Moderate reduction in ciprofloxacin AUC |
| Antidiabetics | Sulfonylureas, glipizide | Reduced efficacy |
| Beta-blockers | Metoprolol, propranolol | Reduced efficacy |
| Antiepileptics | Phenytoin (complex interaction) | Altered drug levels |
| Corticosteroids | Prednisolone | Reduced steroid effect |
| Clindamycin | Clindamycin | Rifampicin significantly reduces clindamycin levels (pharmacokinetic study, PMID 37302771) |
The interaction with clindamycin is particularly relevant in orthopedics - rifampicin markedly decreases clindamycin plasma concentrations through induction of CYP3A4, requiring dose adjustment or alternative partner selection.
6.5 Hypersensitivity Reactions (Less Common)
- Flu-like syndrome: Fever, chills, headache, myalgia (more common with intermittent dosing - reason why daily dosing is preferred)
- Cutaneous reactions: Pruritus, rash, urticaria
- Anaphylaxis: Rare
6.6 Hematological
- Thrombocytopenia (immune-mediated, rare with daily dosing, more common with intermittent)
- Hemolytic anemia
- Leukopenia
6.7 Renal
- Acute tubular necrosis, interstitial nephritis (rare, mostly with intermittent high doses)
- Orange-colored urine (not harmful - discoloration only)
6.8 Other
- Headache, dizziness, visual disturbances (rare)
- Elevated serum uric acid (mild)
7. Resistance Mechanisms
Rifampicin resistance arises rapidly and almost exclusively through single-step point mutations in rpoB (gene encoding the β subunit of RNAP). These mutations alter the rifampicin binding pocket so that the drug can no longer bind effectively.
| Resistance Mechanism | Details |
|---|---|
| rpoB mutation | Most common; cluster of mutations at codons 516, 526, 531 (Mycobacteria) or equivalent positions in staphylococci |
| Biofilm-mediated | Slow-growing sessile bacteria in biofilm display phenotypic tolerance (not true resistance) |
| Efflux pumps | Less significant but described |
| ADP-ribosyltransferases | Inactivate rifampicin (uncommon) |
Clinical implication: Because a single point mutation produces high-level resistance, the frequency of spontaneous resistant mutants is ~1 in 10^7-10^8 bacteria. Even large bacterial burdens (as in osteomyelitis or PJI) contain resistant mutants. Using rifampicin with a second active antibiotic kills these mutants before they expand - this is the entire rationale for mandatory combination therapy.
8. Contraindications
| Contraindication | Reason |
|---|---|
| Severe hepatic dysfunction (Child-Pugh C) | Major risk of fulminant hepatic failure |
| Hypersensitivity to rifamycins | Cross-reactivity within class |
| Rifampicin monotherapy | Rapid resistance emergence - never use alone in bacterial infections |
| HIV patients on protease inhibitors | Profound drug interaction - use rifabutin instead |
| Organ transplant patients on calcineurin inhibitors without close monitoring | Risk of rejection |
Relative contraindications (use with caution):
- Alcoholic liver disease
- Concurrent hepatotoxic medications
- Concurrent anticoagulation with warfarin
- Pregnancy (Category C - risk-benefit assessment required; used in TB)
9. Monitoring and Precautions
Before Starting
- Baseline LFTs (ALT, AST, bilirubin, ALP) and serum creatinine
- Full blood count (FBC/CBC)
- Drug interaction review - check ALL current medications
- Bilirubin/jaundice history - baseline assessment
- Inform patient about orange discoloration of body fluids
- Soft contact lens warning - advise glasses
- Contraception counseling - advise additional barrier method
During Treatment
- LFTs: At 2 weeks, 4 weeks, then monthly (or at any symptom of hepatitis)
- FBC: Baseline, then monthly
- Symptoms: Enquire about jaundice, nausea, RUQ pain at every visit
- Drug levels of co-medications: Especially anticoagulants (INR weekly initially), immunosuppressants, antiretrovirals
Stopping Rules
- Stop immediately if: jaundice, ALT >5x ULN (asymptomatic), or ALT >3x ULN with symptoms
- Renal monitoring if pre-existing kidney disease
10. Special Situations in Orthopedics
Optimal Timing of Rifampicin Initiation in PJI
- Controversial but critical: Evidence suggests rifampicin should be delayed until the acute bacteremia/bacteriuria is controlled and surgical debridement has removed the bulk of the biofilm
- Starting rifampicin with a high bacterial burden (before debridement) risks rapid emergence of resistance
- Recommended practice: Start rifampicin 3-7 days after surgery and after initial bacteremia has cleared (usually confirmed by 2 negative blood cultures)
Duration of Rifampicin in PJI
- Hip PJI with DAIR: 3 months (IDSA/EBJIS recommendation)
- Knee PJI with DAIR: 3-6 months
- Chronic PJI after 2-stage exchange: Rifampicin during the oral phase (typically 3 months after reimplantation)
- Two-stage with spacer: Rifampicin included in antibiotic regimen during the inter-stage interval
High-Dose Rifampicin - Emerging Evidence
Recent translational research using PET/CT to measure rifampicin bone concentrations found that standard doses (10-15 mg/kg/day) achieve very low bone levels (AUC bone:plasma ratio ~0.14). High-dose rifampicin (25-35 mg/kg/day) significantly improved bone concentrations and bacterial killing in animal models, and a 4-week high-dose course was noninferior to a 6-week standard-dose course. Clinical studies are ongoing.
Rifampicin in MRSA Osteomyelitis
Per IDSA guidelines: Vancomycin (first-line) with the addition of rifampicin recommended for MRSA bacteremia complicated by osteomyelitis. Vancomycin trough targets: 15-20 µg/mL.
11. Practical Summary Table
| Feature | Detail |
|---|---|
| Class | Rifamycin antibiotic |
| Target | β subunit of bacterial RNAP |
| Activity | Bactericidal; active against biofilm, intracellular, and dormant bacteria |
| Main organisms targeted | Staphylococci (MSSA, MRSA, CoNS), Mycobacterium tuberculosis |
| Route | Oral (preferred), IV available |
| Standard dose | 300-600 mg twice daily (adult) |
| KEY RULE | NEVER use as monotherapy |
| Primary orthopedic indications | PJI, osteomyelitis, FRI, TB bone/joint |
| Main side effect | Hepatotoxicity; drug interactions via CYP induction |
| Monitoring | LFTs, FBC, drug interaction check |
| Contraindications | Severe liver disease, rifamycin allergy, concurrent PIs (HIV) |
12. Recent Evidence (PubMed, 2023-2025)
- PMID 37302771 (2023, Int J Antimicrob Agents): Rifampicin significantly reduces clindamycin plasma concentrations in staphylococcal osteoarticular infections through pharmacokinetic interaction - dose adjustment of clindamycin needed when used with rifampicin.
- PMID 38517016 (2024, Bone Joint Res): Implant retention in fracture-related infection model - rifampicin-containing regimens showed superior outcomes.
- RICOTTA Trial (2024, Bone & Joint): Ongoing RCT comparing rifampicin combination therapy vs antimicrobial monotherapy in the oral phase of staphylococcal PJI - results eagerly awaited.
- High-dose rifampicin study (Science Translational Medicine): PET/CT demonstrated bone:plasma AUC ratio of 0.14 in human S. aureus bone infections; high-dose (35 mg/kg) achieved superior bone levels and bacterial killing in animal models with fewer adverse effects vs longer standard-dose courses.
Key Takeaway Points for Orthopedic Practice
- Rifampicin's unique value in orthopedics is its ability to penetrate biofilm, kill intracellular bacteria, and act against slow-growing/dormant organisms - properties no other common antibiotic combines.
- Mandatory combination - always pair with an active partner drug (ciprofloxacin for MSSA/CoNS; TMP-SMX or doxycycline for MRSA oral phase).
- Delay initiation until debridement is done and bacteremia cleared (typically day 3-7 post-surgery) to prevent resistance selection.
- Hepatotoxicity and CYP interactions are the most clinically impactful adverse effects - perform baseline LFTs and comprehensive drug interaction check before prescribing.
- Warn patients proactively about orange body fluid discoloration and contact lens staining.
- TB spine and joints represent the other major orthopedic niche where rifampicin is the backbone of a multi-drug regimen for 6-12 months.
This is a shared conversation. Sign in to Orris to start your own chat.