Elbow arthroscopy for orthopaedics 10 marks pg answer with flow chart and images
Reading File
Finding Sources
Searching the Web
elbow arthroscopy orthopaedics indications portals technique complications
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from Campbell's Operative Orthopaedics (2026) and Miller's Review of Orthopaedics. Let me compile the full 10-mark answer with all images and a flowchart.
ELBOW ARTHROSCOPY
10-Mark Structured Answer - Orthopaedics
DEFINITION
Elbow arthroscopy is a minimally invasive surgical procedure in which a small-diameter arthroscope is introduced into the elbow joint through small skin portals to visualize, diagnose, and treat intra-articular pathology.
HISTORICAL NOTE
Elbow arthroscopy has advanced considerably in popularity and sophistication. New portals and more advanced surgical techniques have been described, and a better understanding of the pathological findings has been obtained. However, it remains technically demanding due to the proximity of major neurovascular structures.
INDICATIONS
(Campbell's Operative Orthopaedics, 15th Ed., 2026)
| Category | Specific Indication |
|---|---|
| Loose bodies | Evaluation and removal |
| OCD | Evaluation and treatment of osteochondritis dissecans of the capitellum |
| Chondral lesions | Radial head osteochondral lesions |
| Osteophytes | Excision from humerus and olecranon |
| Synovitis | Partial synovectomy, especially in rheumatoid disease |
| Stiffness | Debridement and lysis of adhesions in post-traumatic/degenerative disease |
| Tennis elbow | Arthroscopic tennis elbow release |
| Diagnostic | Painful elbow when other diagnostic tests are inconclusive |
| Bursitis | Debridement of inflamed olecranon bursae |
| Instability | Stabilization procedures |
| Fractures | Treatment of select intra-articular fractures |
CONTRAINDICATIONS
- Bony ankylosis or severe fibrous ankylosis preventing safe arthroscope introduction
- Previous anterior transposition of ulnar nerve - eliminates certain portals (relative contraindication)
- Periarticular infection
PATIENT POSITIONING
Three positions are acceptable:
1. Supine Position (most common)
- Hand/forearm in sterile waterproof stockinette suspension with 5-6 lb weight
- Shoulder: neutral rotation + 90° abduction
- Elbow: 90° flexion
- Allows access to both sides; neurovascular structures in antecubital fossa are relaxed
- Surgeon sits on rolling stool at chest level
2. Prone Position
- Patient prone on chest rolls with tourniquet proximally
- Shoulder in 90° abduction, elbow in 90° flexion, hand pointing toward floor
- Advantages: improved arthroscopic mobility, easier joint manipulation, better access to the posterior compartment
3. Lateral Decubitus Position
- Can be performed on standard operating table
Anesthesia: General anesthesia preferred - complete muscle relaxation and eliminates intraoperative discomfort.
Equipment: 4-mm, 30° arthroscope (standard) and 2.7-mm, 70° wide-angle arthroscope. Inflow by gravity or pump at 40-50 mmHg.
PORTALS
The elbow's proximity to the brachial artery, median nerve, ulnar nerve, and radial nerve makes portal placement the most critical and hazardous step.
FLOWCHART: Portal Establishment Sequence
START
│
▼
Joint Distension
(Direct Lateral Portal / Soft Spot)
│
├── 18-gauge needle → 20-30 mL saline
├── Triangular soft spot: lateral epicondyle + radial head + olecranon tip
└── Capsule distension pushes NV structures away from joint
│
▼
Anterolateral Portal (Diagnostic Portal - First)
│
├── Proximal anterolateral: 2 cm proximal + 1 cm anterior to lateral epicondyle [PREFERRED]
├── Mid-anterolateral: just proximal + ~1 cm anterior to radiocapitellar joint
└── Distal anterolateral (traditional): 2-3 cm distal + 1 cm anterior to lateral epicondyle
At risk: Radial nerve, lateral antebrachial cutaneous nerve
│
▼
Anteromedial / Proximal Medial Portal (Working Portal)
│
├── Proximal medial (preferred): 2 cm proximal to medial epicondyle, anterior to septum
├── Anteromedial (traditional): 2 cm distal + 2 cm anterior to medial epicondyle
└── At risk: Ulnar nerve, medial antebrachial cutaneous nerve, brachial artery, median nerve
│
▼
Posterior Portals (for posterior compartment)
│
├── Direct posterior (transtriceps): 3 cm proximal to olecranon tip, through olecranon fossa
├── Posterolateral: just lateral to triceps tendon, 1-4 cm proximal to olecranon
├── Proximal posterolateral: 2.5-3 cm proximal to olecranon, elbow in 30° flexion
└── At risk: Posterior antebrachial cutaneous nerve, ulnar nerve
│
▼
Direct Lateral Portal (if needed)
│
└── Center of triangle: lateral epicondyle + radial head + olecranon tip
Traverses: skin → subcutaneous tissue → anconeus → capsule
│
▼
PROCEDURE COMPLETE
Portal Anatomy - Images
Medial and Lateral portal views (Miller's Review of Orthopaedics, 9th Ed.):
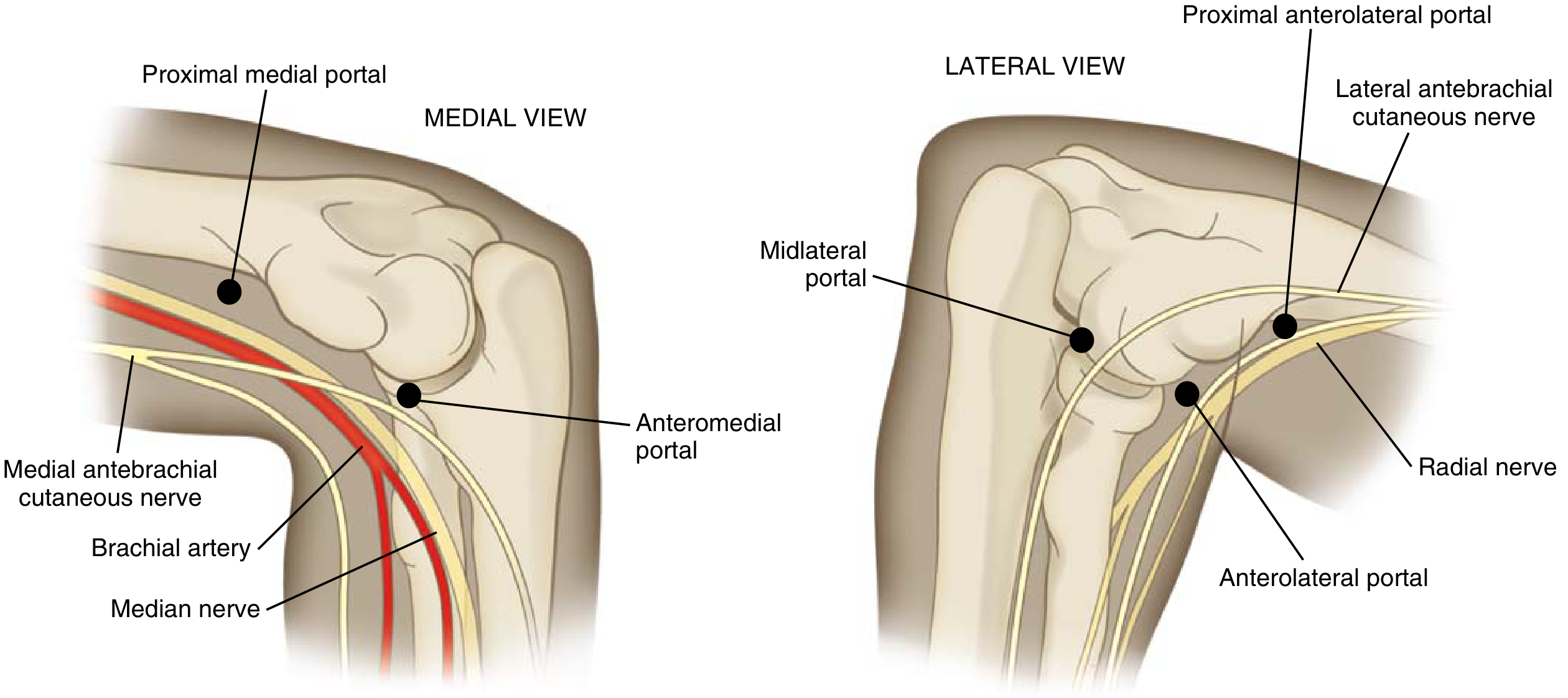
Fig. 1 - Medial view: Proximal medial portal (2 cm proximal to medial epicondyle, anterior to intermuscular septum) and anteromedial portal. At risk: brachial artery, median nerve, medial antebrachial cutaneous nerve. Lateral view: Proximal anterolateral portal and anterolateral portal, with radial nerve nearby.
Posterior portals (Miller's Review of Orthopaedics, 9th Ed.):
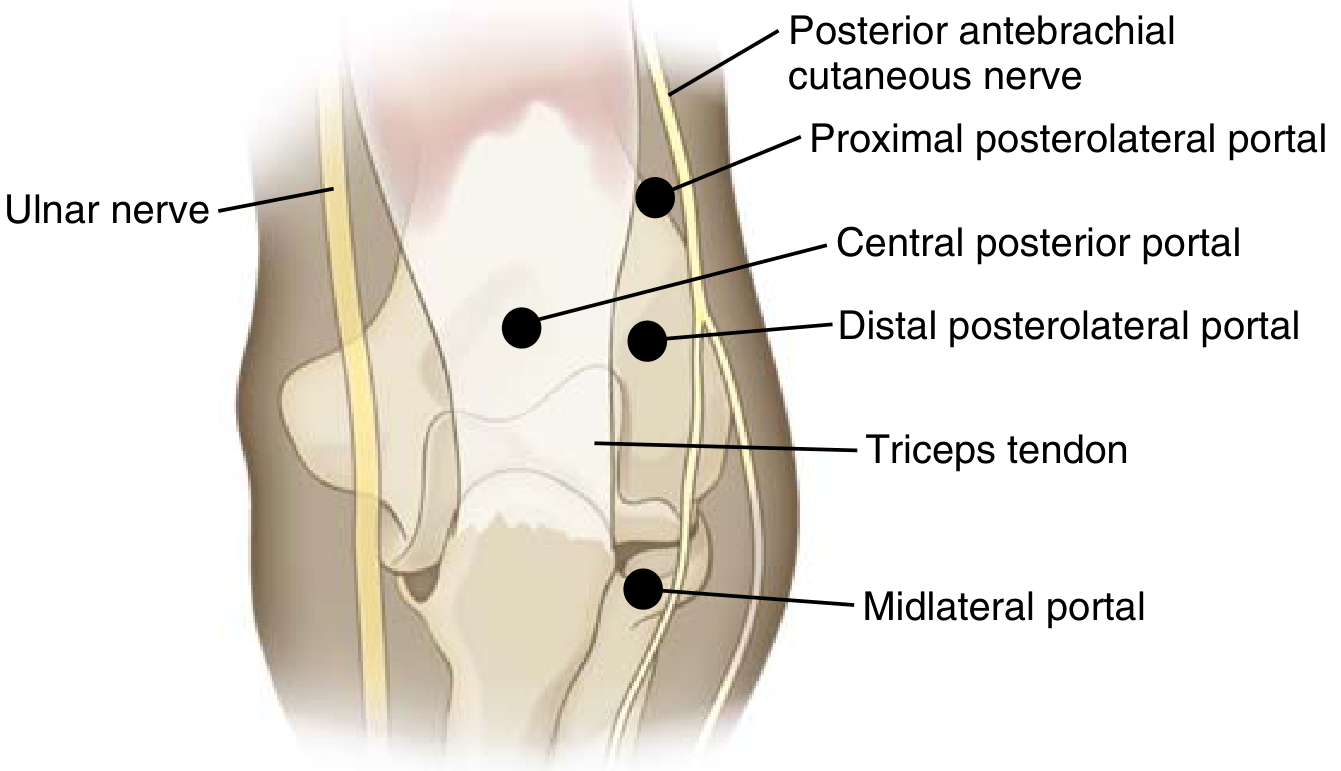
Fig. 2 - Posterior view: Proximal posterolateral portal, central posterior portal, distal posterolateral portal, and midlateral portal. Ulnar nerve and posterior antebrachial cutaneous nerve are at risk.
Medial portal - landmark (2 cm from medial epicondyle, anterior to septum):
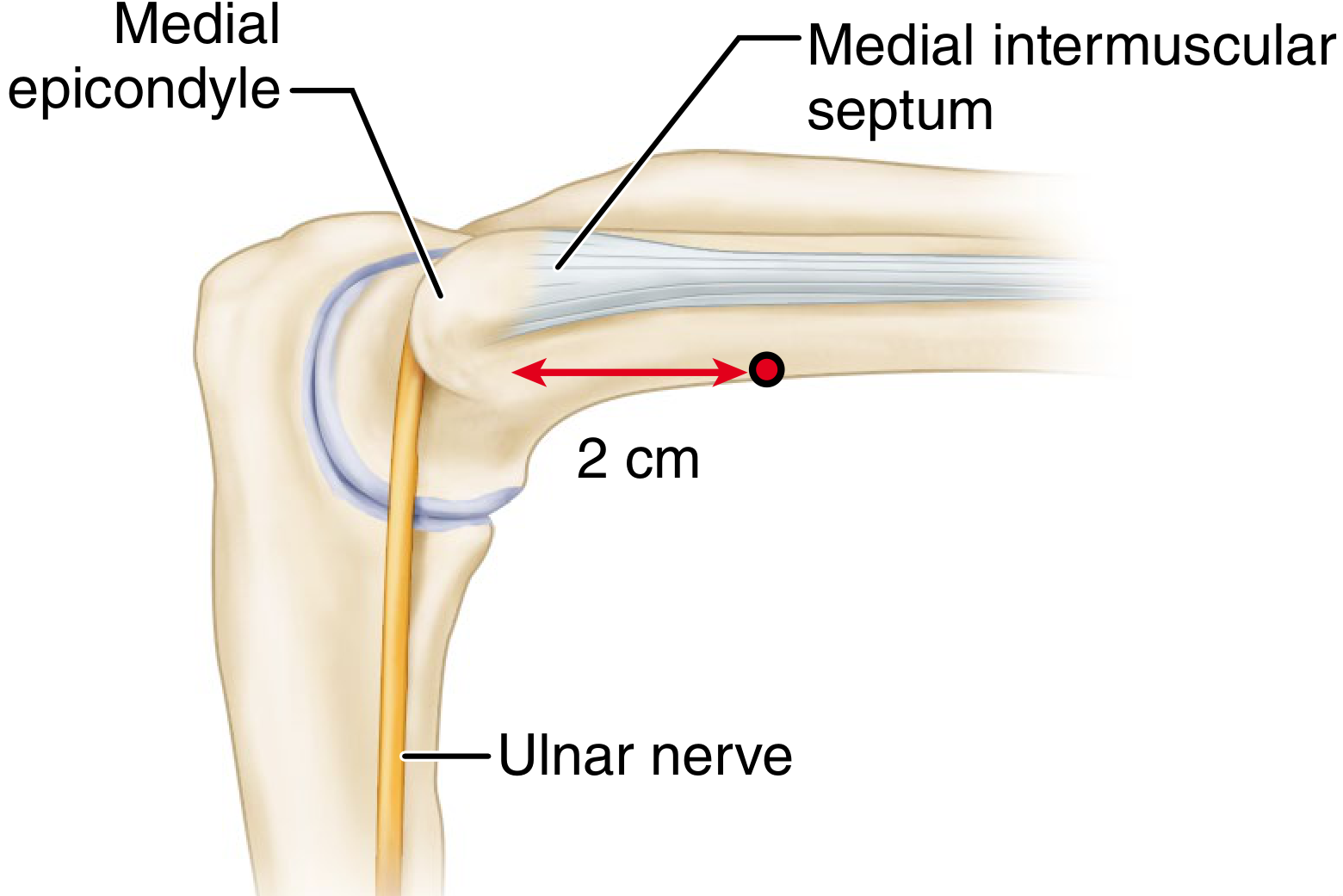
Fig. 3 - Proximal medial portal: placed 2 cm proximal to medial epicondyle and anterior to medial intermuscular septum, away from ulnar nerve.
Medial neurovascular anatomy at the elbow (Orthobullets):

Fig. 4 - Superomedial portal with neurovascular relations. The ulnar nerve lies posterior to medial epicondyle; median nerve and brachial artery lie anteromedially.
Lateral view - direct lateral portal and radial nerve anatomy:

Fig. 5 - Lateral portal: direct lateral portal in the soft spot triangle. Radial nerve and lateral antebrachial cutaneous nerve branches are at risk.
TECHNIQUE: ELBOW ARTHROSCOPY (Technique 57.32, Campbell's 2026)
Step-by-Step Technique
1. Joint Distension (via direct lateral soft spot)
- Inject 20-30 mL of normal saline using an 18-gauge needle
- Distension pushes neurovascular structures anteriorly and away
2. Anterolateral Portal (First Working Portal)
- Mark the proximal anterolateral portal: 2 cm proximal + 1 cm anterior to lateral epicondyle
- Nick skin with No. 11 blade; bluntly dissect down to fascia with mosquito hemostat
- Pass arthroscopy cannula + blunt trocar at ~70° to horizontal, capturing joint capsule laterally
- Examine: coronoid process, trochlear ridge, anterior capsule, medial collateral ligament, radiocapitellar joint, annular ligament, capitellum
3. Anteromedial Portal (Second Working Portal)
- Established via Wissinger rod technique or under direct arthroscopic vision
- Used for instrumentation and assessment of medial structures
4. Direct Lateral Portal
- Posterior to the radiocapitellar joint
- Traverses anconeus muscle
- Views: radiocapitellar articulation, radial head (pronation/supination), capitellum
5. Posterior Portals
- For posterior compartment: olecranon tip/fossa, posteromedial and posterolateral gutters, triceps, posterior medial collateral ligament
SYSTEMATIC ARTHROSCOPIC EXAMINATION
| Portal | Structures Visualized |
|---|---|
| Anterolateral | Coronoid process, trochlea, anterior capsule, MCL (anterior 10-15%), synovium |
| Anteromedial | Radial head, capitellum, annular ligament, radiocapitellar + radioulnar joints |
| Direct lateral | Three-bone articulation (radius, ulna, humerus), radial head bare area |
| Posterolateral | Posterior compartment, olecranon fossa, olecranon tip, medial gutter, posterior UCL |
| Direct posterior | Olecranon fossa, trochlea, posterior compartment |
COMPLICATIONS
Elbow arthroscopy has a higher complication rate than other joints (6% minor, 1% major).
FLOWCHART: Complications
COMPLICATIONS OF ELBOW ARTHROSCOPY
│
┌───────┴────────┐
MAJOR MINOR
│ │
Nerve injury Fluid extravasation
(most common & Superficial infection
devastating) Temporary neurapraxia
│ Hematoma
┌─┴────────────┐ Stiffness
Anterior Posterior
portals portals
│ │
Radial nerve Posterior antebrachial
Median nerve cutaneous nerve
Brachial artery Ulnar nerve
│
Permanent motor/
sensory deficit
Nerve-Portal Risk Map
| Portal | At-Risk Structure |
|---|---|
| Proximal anterolateral | Radial nerve (closest - 3.4 mm avg) |
| Anterolateral (distal) | Posterior interosseous nerve |
| Anteromedial (distal) | Median nerve, medial antebrachial cutaneous |
| Proximal medial | Medial antebrachial cutaneous nerve |
| Direct posterior | Ulnar nerve |
| Posterolateral | Posterior antebrachial cutaneous nerve |
Prevention:
- Always use nick-and-spread technique (never stab blindly)
- Identify ulnar nerve and medial epicondyle before medial portals
- Distend joint fully before any portal creation
- Use blunt trocars, not sharp
- Monitor fluid extravasation; abort if antecubital fossa becomes tense
SPECIFIC PROCEDURES PERFORMED ARTHROSCOPICALLY
- Loose body removal - most common indication; confirms diagnosis and removes fragments
- OCD capitellum - debridement/fixation/microfracture for unstable lesions
- Elbow contracture release - anterior and posterior capsulotomy; lysis of adhesions
- Tennis elbow (lateral epicondylitis) release - ECRB debridement
- Partial synovectomy - rheumatoid/inflammatory arthritis
- Olecranon/coronoid osteophyte excision - valgus extension overload (throwing athletes)
- Septic arthritis washout - effective as open drainage in acute cases
- Radial head excision - select cases
- Fracture-assisted reduction - radial head, coronoid fractures
POSTOPERATIVE CARE
- Portal wounds: steri-strips or single suture
- Bulky compressive dressing for 24-48 hours
- Early range-of-motion exercises started within 24-72 hours
- Neurovascular assessment on recovery
SUMMARY TABLE
| Feature | Details |
|---|---|
| Scope size | 4 mm, 30° (standard); 2.7 mm, 70° (supplemental) |
| Pump pressure | 40-50 mmHg (low pressure) |
| Tourniquet | High on arm (proximal) |
| First portal | Distension via lateral soft spot |
| Standard diagnostic | Proximal anterolateral |
| Most dangerous step | Anteromedial portal (median nerve, brachial artery nearby) |
| Most common complication | Nerve injury (6% minor, 1% major) |
| Key rule | Nick-and-spread technique always; never stab |
Sources:
- Campbell's Operative Orthopaedics, 15th Ed. (2026) - Chapter 57, p. 3223-3232
- Miller's Review of Orthopaedics, 9th Ed. - Elbow Arthroscopy portals, p. 731
This is a shared conversation. Sign in to Orris to start your own chat.