Hysteroscopy — Complete Practical Overview
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hysteroscopy"[MeSH Terms] AND ("technique" OR "complications" OR "outcomes")
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
hysteroscopy uterine cavity endoscope view
Reading File
Reading File
Searching Images
hysteroscopy submucous fibroid polyp resection
Reading File
Reading File
Searching Images
hysteroscopy distension media intrauterine adhesions Asherman syndrome
Reading File
Reading File
Reading File
Reading File
Hysteroscopy — Complete Practical Overview
1. Definition and Historical Context
A hysteroscope is an endoluminal endoscope adapted from the urologic cystoscope that enables direct visualization of the cervical canal and endometrial cavity for both diagnosis and intrauterine procedures. The first published hysteroscopic procedure (a polypectomy) dates to 1869, but routine clinical use did not emerge until the latter half of the 20th century. Key milestones include:
- 1973 — first hysteroscopic lysis of intrauterine adhesions (IUAs)
- Electrosurgical resection adapted from urology for submucous leiomyoma removal
- Mechanical septum division using purpose-built scissors
- Nd:YAG laser endometrial ablation → later superseded by RF resectoscope and, from 2002, hysteroscopically guided thermal ablation ("nonresectoscopic EA")
- Modern miniaturized instruments now allow the vast majority of procedures to be performed in an office or procedure room under local or no anesthesia
— Berek & Novak's Gynecology; Pfenninger and Fowler's Procedures for Primary Care, 3rd ed.
2. Indications
Diagnostic
| Category | Specific Indication |
|---|---|
| Bleeding | Unexplained abnormal uterine bleeding (pre- and postmenopausal) |
| Lesions | Endometrial polyps, submucous leiomyoma, hyperplasia/malignancy |
| Structural anomaly | Uterine septum, arcuate uterus, Müllerian anomaly |
| Adhesions | Asherman's syndrome (intrauterine adhesions) |
| Fertility/RPL | Infertility workup, recurrent pregnancy loss, abnormal HSG |
| Foreign body | Lost/embedded IUD, retained products of conception |
| Pre-procedural | Evaluation before endometrial ablation (any method) |
| Other | Occluded tubal ostia, endometriosis, suspected malignancy |
Therapeutic / Operative
- Adhesiolysis (IUA lysis)
- Endometrial polypectomy
- Submucous myomectomy
- Uterine septum resection (metroplasty)
- Endometrial ablation (resectoscopic or nonresectoscopic)
- Foreign body / IUD removal
- Retained products of conception removal
- Hysteroscopic sterilization (Essure microinsert)
- Directed endometrial biopsy
Hysteroscopy is considered the gold standard for uterine cavity evaluation because it permits direct visualization and, unlike blind sampling, can detect focal lesions such as polyps and submucous fibroids that curettage misses.
— Berek & Novak's Gynecology, p. 1356; Pfenninger and Fowler's, p. 976
3. Contraindications
| Type | Examples |
|---|---|
| Absolute | Cardiac or pulmonary instability; acute pelvic infection |
| Relative | Pregnancy; coagulopathy (ITP, von Willebrand disease); known cervical/uterine carcinoma; acute heavy uterine bleeding; previous uterine perforation or recent surgery; morbid obesity |
— Pfenninger and Fowler's, p. 976
4. Equipment
4a. The Hysteroscope
Rigid hysteroscope — solid rod lens; preferred diameter ≤5–5.5 mm (including introducing sheath) to minimize required cervical dilation and patient discomfort. Viewing angles:
- 0° — panoramic view, ideal all-purpose scope
- 12° and 30° — more restricted, downward-looking views (require orientation adjustment to navigate the cervical canal)
Flexible hysteroscope — 3.5–5 mm diameter; distal tip deflects 90–120°; no outer sheath needed; built-in operating channel; latest models use digital chip-on-tip sensors rather than fiberoptic bundles. Advantages: greater maneuverability, better patient tolerance. Disadvantage: higher cost; operating channel may be smaller.

4b. Light Source
A 100–300 W xenon light source is preferred (emulates daylight, superior illumination). Halogen is acceptable.
4c. Sheaths and Operating Channels
Rigid hysteroscopes are fitted with an outer sheath before passage through the cervix. Continuous-flow sheaths (with fenestrations at the distal tip) allow simultaneous inflow and outflow of distension media, maintaining a clear view. Operating sheaths contain a 1–2.3 mm channel for passage of:
- Biopsy forceps
- Grasping forceps
- Scissors
- Electrosurgical electrodes (monopolar or bipolar RF needles, loops, rollerball)
- Nd:YAG laser fibers
4d. Energy Sources for Operative Hysteroscopy
| Modality | Use |
|---|---|
| Monopolar RF (loop/rollerball/vaporize) | Leiomyoma resection, endometrial ablation, septum division — requires electrolyte-free distension media |
| Bipolar RF | Safer in saline; reduces TUR syndrome risk |
| Nd:YAG laser | Vaporization/ablation; largely superseded by RF |
| Mechanical scissors | Adhesiolysis, septum transection ("cold" technique — minimizes thermal endometrial damage) |
4e. Resectoscope
The resectoscope (adapted from urology) is the standard instrument for larger operative procedures (myomectomy, ablation). It consists of a 26–28 Fr outer sheath with a high-flow irrigation system and an electrode operating element. It requires general or spinal anesthesia and operating room setup.
— Berek & Novak's Gynecology, p. 1372–1386
5. Patient Preparation
Timing
For premenopausal women, scheduling in the early proliferative phase (days 7–10) allows optimal visualization of a thin endometrium.
Cervical Preparation
- Misoprostol 400 μg orally or 200–400 μg vaginally, approximately 3–24 hours before the procedure, facilitates cervical dilation — particularly useful in postmenopausal women (higher-quality evidence)
- Postmenopausal women may benefit from vaginal estrogen daily for 2 weeks pre-procedure
- Intracervical vasopressin (0.05 U/mL, 4 cc at 4 and 8 o'clock) intraoperatively significantly reduces force needed for dilation
Anesthesia Options
- No anesthesia — small-diameter diagnostic hysteroscopy is often well tolerated
- Topical/local — topical bupivacaine + intrastromal cervical block (2% lidocaine ± epinephrine, 4-quadrant injection)
- Paracervical block
- Conscious sedation / general/spinal anesthesia — for complex operative procedures or anxious patients
— Berek & Novak's Gynecology, p. 1376; Pfenninger and Fowler's, p. 978
6. Distension Media
Distension of the endometrial cavity is essential to create a viewing space. A minimum pressure of ~45 mmHg is needed; the lowest effective pressure should be used (should not exceed mean arterial pressure) to minimize extravasation.
| Medium | Type | Energy Compatibility | Notes |
|---|---|---|---|
| Normal saline (0.9%) | Isotonic electrolyte | Bipolar RF / diagnostic | Safest; preferred for office hysteroscopy and bipolar systems |
| CO₂ gas | Gas | Diagnostic only | Clear view initially; risk of severe cramping and shoulder pain if gas passes through tubes into peritoneum; no liquid pooling |
| 1.5% Glycine | Hypotonic, electrolyte-free | Monopolar RF | Risk of dilutional hyponatremia (TUR syndrome) if absorbed |
| 3% Sorbitol | Hypotonic, electrolyte-free | Monopolar RF | Similar risks to glycine |
| 5% Mannitol | Slightly hypotonic | Monopolar RF | Osmotic diuresis reduces fluid overload risk |
| Dextrose in water | Hypotonic | Diagnostic | Rarely used |
| 32% Dextran 70 | High-viscosity | Diagnostic | Can crystallize in instruments; risk of anaphylaxis; largely abandoned |
Fluid deficit monitoring is mandatory during operative hysteroscopy. Absorption of >1,000–1,500 mL of electrolyte-free media requires immediate termination of the procedure to prevent dilutional hyponatremia and pulmonary edema (TUR-like syndrome).
— Berek & Novak's Gynecology, p. 1378
7. Technique — Step-by-Step
Positioning
Modified dorsal lithotomy with legs in knee-calf-ankle stirrups. "Candy cane" stirrups are avoided, particularly for conscious patients.
Examination
Bimanual pelvic examination before instrumentation to determine uterine size, position (version and flexion), and adnexal findings.
Vaginoscopic ("No-Touch") Approach
For many patients, the hysteroscope can be passed directly into the vagina under vision, the external os identified endoscopically, and advanced into the cavity without a tenaculum or dilation — significantly reducing pain. Tenaculum and dilation are reserved for stenotic or narrow cervices.
Cervical Dilation
When required, progressive dilation is performed with graduated dilators, respecting the version and flexion of the uterus. Simultaneous transabdominal ultrasound guidance helps in difficult cases. Avoid using a uterine sound (traumatizes canal, can cause bleeding or perforation).
Entry and Systematic Survey
- Insert hysteroscope under direct vision through endocervical canal
- Identify internal os
- Advance into endometrial cavity
- Systematically inspect: fundus → right cornua/tubal ostium → left cornua/tubal ostium → anterior wall → posterior wall → lateral walls → isthmus → endocervical canal (on withdrawal)
- Note negative and positive findings at each anatomical level
- Perform biopsy, polypectomy, or other procedure as indicated
Reporting
Hysteroscopic findings should document both positive and negative findings at each level: cornua and tubal ostia, fundus, anterior/posterior/lateral walls, isthmus, internal os, and endocervical canal. Also document: endometrial appearance, distension medium used and recovered, estimated blood loss, complications.
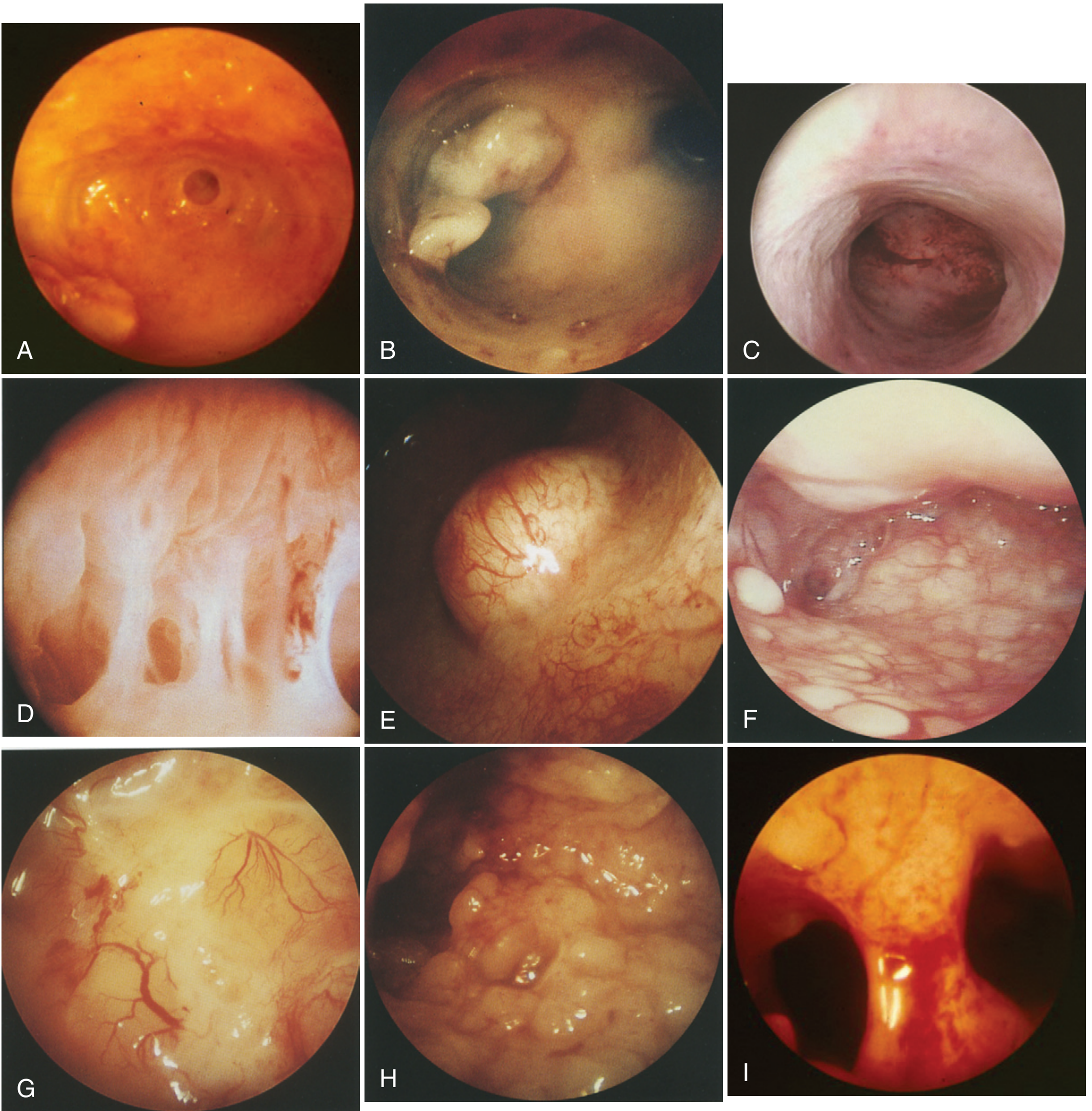
8. Hysteroscopic Findings — Interpretation
Normal
Endometrial cavity is smooth, pale pink; gland ostia visible as tiny openings; bilateral tubal ostia appear as dark circular depressions at cornua.

Endometrial Polyps
Exophytic, usually sessile lesions; soft on contact with forceps; surface resembles surrounding endometrium; pedunculated forms have a vascular pedicle. Can be associated with glandular hyperplasia.
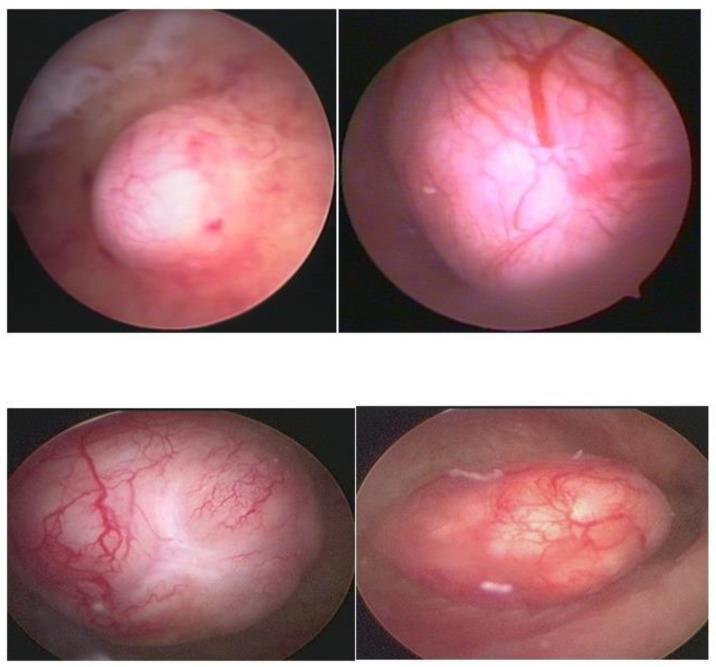
Submucous Leiomyoma (Fibroid)
Round/ovoid, smooth to lobulated, pearly white, with prominent surface vessels. Compressed endometrium may show ulceration at apex. FIGO classification (Type 0–2) based on intramural extension:
- Type 0 — entirely intracavitary, no intramural component
- Type 1 — ≥50% intracavitary
- Type 2 — <50% intracavitary
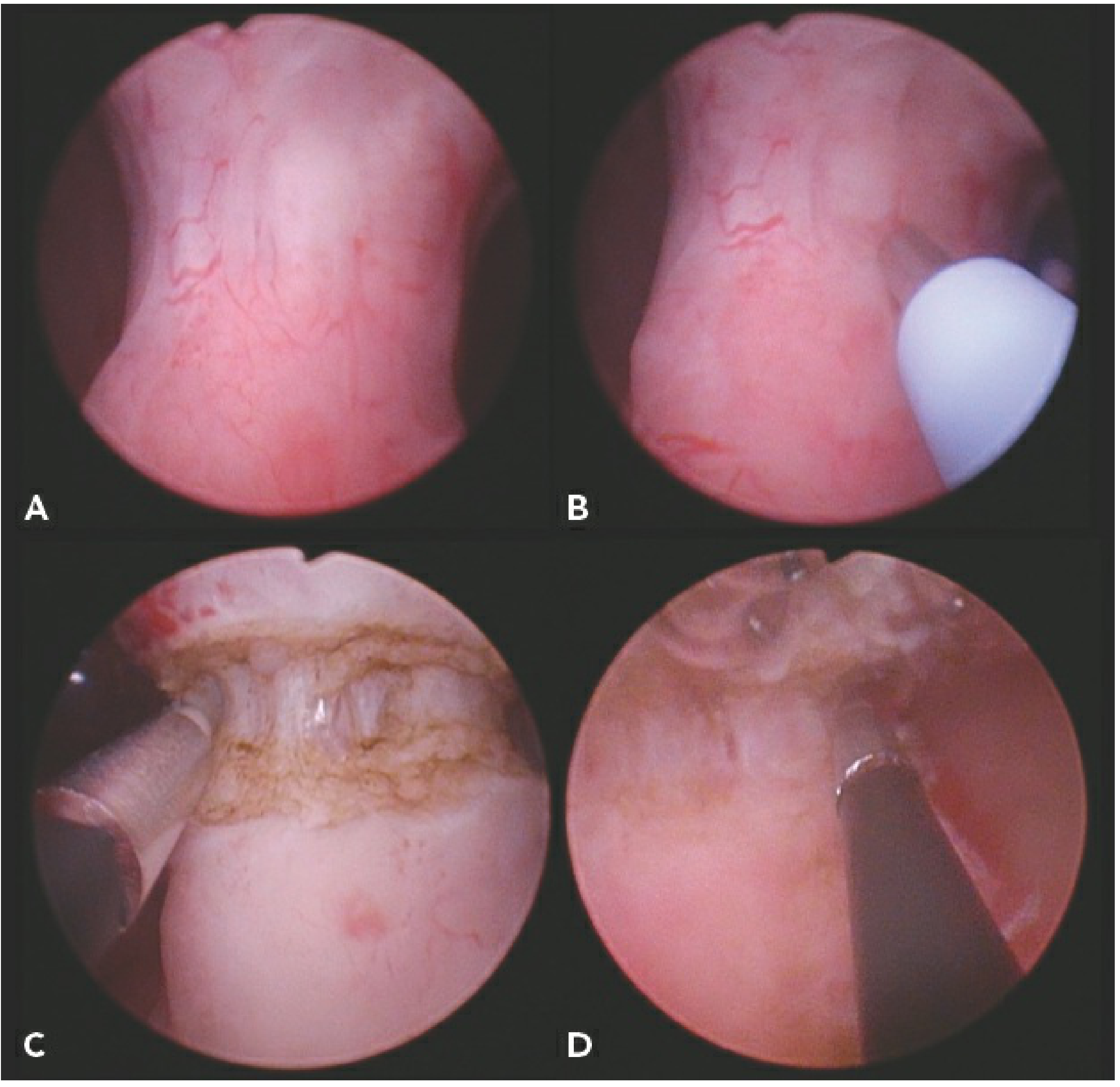
Intrauterine Adhesions (Synechiae / Asherman's Syndrome)
Pale, fibrous bands bridging uterine walls; may be filmy (endometrial — from abortive tissue, easy to lyse) or dense "buttress"-like myometrial adhesions or connective fiber adhesions that distort cavity morphology. Classified by the American Fertility Society (AFS) scoring system.

Uterine Septum
- Arcuate — fundal bulge protruding downward; may appear atrophic relative to surrounding endometrium
- Incomplete/complete septum — classic "double-barrel shotgun" appearance on entry past internal os; septum has same endometrial covering as surrounding tissue
Endometrial Atrophy (Postmenopausal)
Thin, pale/nearly white mucosa; transparent, revealing underlying vasculature; hemorrhagic petechiae typical.
Endometrial Hyperplasia
- Low-risk (EH/EIN grade 1): widened glandular ostia with cystic formations ~1 mm; increased thickness; non-homogeneous regeneration
- High-risk (EIN): polypoid appearance; arborescent "corkscrew" vascularization; "cerebroid" mucosal surface due to abnormal glandular growth
Endometrial Carcinoma
Irregular, polylobular excrescences; bleeding or necrotic areas; irregular/anarchic vascularization. May appear as focal lesions at cornua or diffuse implants. Hysteroscopy is highly reliable for diagnosis; a directed biopsy confirms histology.
— Pfenninger and Fowler's, p. 982–984
9. Operative Procedures in Detail
Polypectomy
Small polyps removed with grasping forceps or scissors through operating channel. Larger polyps require resectoscope loop resection or morcellation. "See and treat" concept: diagnosis and excision in single outpatient visit.
Myomectomy (Submucous)
- Type 0 and 1 fibroids: resectoscope loop under electrolyte-free media (monopolar) or saline (bipolar)
- Shave resection technique until fibroid is flush with the endometrial surface
- Type 2 fibroids: challenging; may require two-stage procedure; risk of incomplete resection and fluid absorption
- GnRH agonist pretreatment (3 months) may reduce fibroid size and vascularity
Adhesiolysis
Mechanical scissors preferred (minimizes thermal injury to residual endometrium). Severe adhesions may require simultaneous laparoscopy and/or ultrasound guidance to prevent perforation. Post-procedure: IUD or Foley balloon catheter placed to stent cavity; estrogen supplementation promotes re-epithelialization.

Septum Resection
Used for recurrent pregnancy loss (RPL) associated with uterine septum (rAFS/CONUTA Class U2). Hysteroscopic metroplasty achieves reproductive outcomes comparable to abdominal metroplasty with substantially reduced morbidity. Technique:
- Confirm external uterine contour by MRI or 3D ultrasound (distinguish septum from bicornuate uterus) before proceeding
- Dissect from anterior to posterior until two of three end-point criteria met: patient pain, bleeding, visualization of myometrial fibers
- Performed with scissors (mechanical) or RF/bipolar needle; can be done under local anesthesia in office
- Simultaneous laparoscopy or transabdominal ultrasound guidance reduces perforation risk
Endometrial Ablation (EA)
Destruction of the endometrium to treat heavy menstrual bleeding (HMB) in women who do not desire future fertility.
First-generation (resectoscopic):
- Rollerball/roller-barrel desiccation
- Loop resection (TCRE)
- Nd:YAG laser vaporization
- Require surgeon skill and carry higher complication risk
Second-generation (nonresectoscopic — NREA):
- Thermal balloon (ThermaChoice, Cavaterm) — heated fluid
- NovaSure (bipolar mesh — impedance-controlled)
- Microwave endometrial ablation (MEA)
- Cryoablation
- Require pre-procedural hysteroscopy to exclude contraindications (submucous fibroids, malignancy, uterine anomalies)
Foreign Body Removal (Embedded IUD)
If IUD strings are absent and ultrasound confirms intracavitary position, operating hysteroscope with grasping forceps allows removal. Partially myometrium-embedded devices require additional imaging; individualized management.
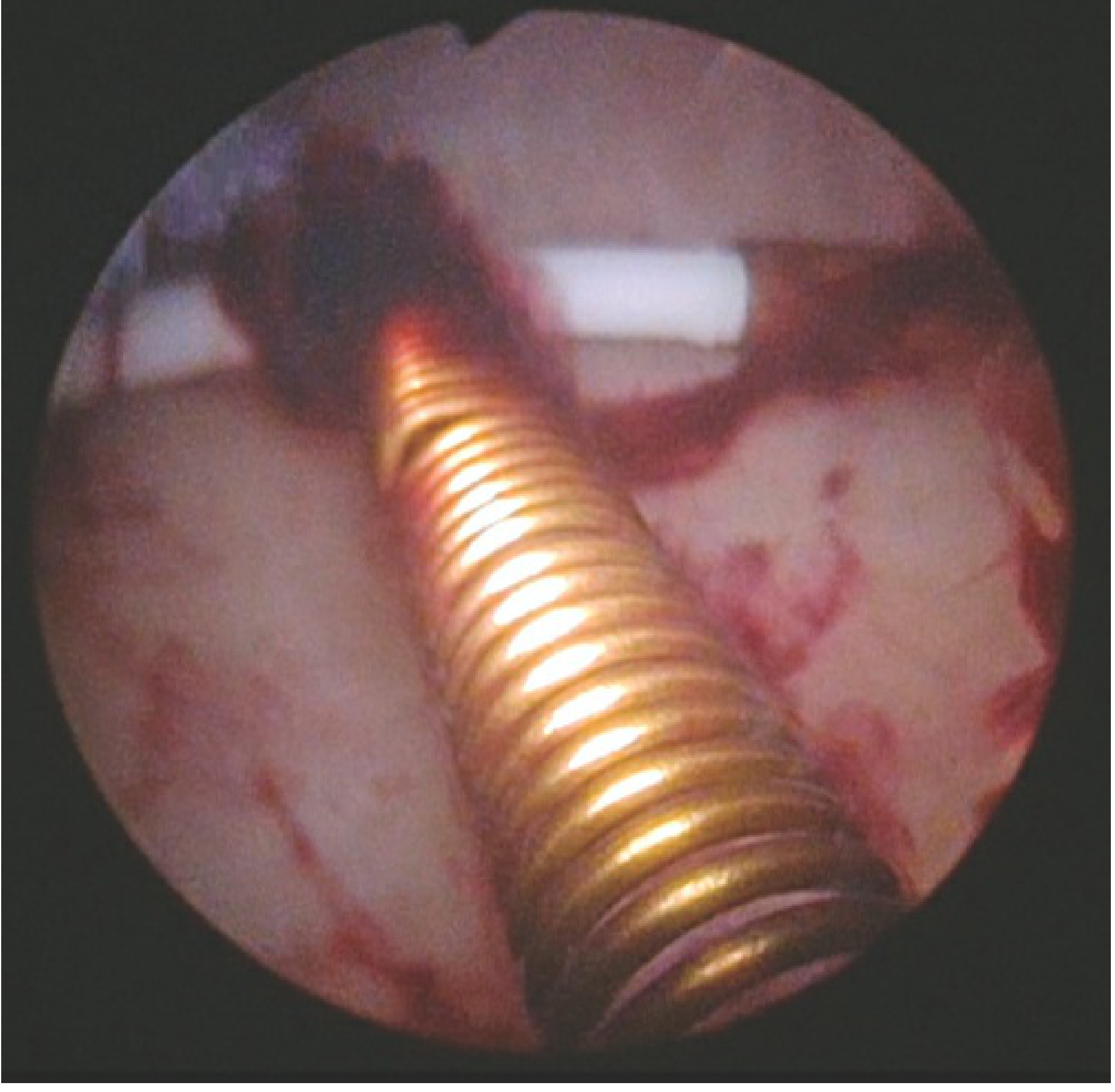
Hysteroscopic Sterilization (Essure)
- Microinsert (stainless steel inner coil + nitinol outer coil + polyethylene terephthalate fibers) deployed into fallopian tube via operating channel
- 3–8 coils remain visible in uterine cavity; remainder are intratubular
- Fibrous tissue ingrowth over ~3 months achieves permanent occlusion
- Confirmation required: modified HSG (no peritoneal spillage) or TVUS (if strict criteria met)
- Failure rate to prevent pregnancy reported up to 2.5%; ~4–8% develop new pelvic pain
— Berek & Novak's Gynecology; Tintinalli's EM, p. 3271
10. Complications
Diagnostic Hysteroscopy — Low Risk
Complications are rare and rarely severe. Expected post-procedure effects: slight vaginal bleeding, mild lower abdominal cramping. Patients should have an escort home.
| Complication | Notes |
|---|---|
| Vasovagal reaction | Most common adverse event |
| Uterine perforation | Usually fundal; most are benign; may require laparoscopy |
| Bleeding | Usually minor |
| Infection | Rare; prophylactic antibiotics not routinely indicated |
| CO₂-related pain | Severe cramping, right shoulder pain if gas passes into peritoneal cavity via tubes |
Operative Hysteroscopy — Higher Risk
| Complication | Mechanism / Notes |
|---|---|
| Uterine perforation | Risk 0–1.8%; risk ↑ with adhesiolysis, deep myometrial dissection; may require laparotomy if adjacent organ injured |
| Fluid overload / TUR syndrome | Absorption of electrolyte-free distension media → dilutional hyponatremia, cerebral edema, pulmonary edema; requires stopping procedure, diuresis, correction of electrolytes |
| Hemorrhage | Especially during myomectomy; vasopressin injection into myoma reduces risk |
| Air/gas embolism | Risk with any hysteroscopic procedure; avoid elevating insufflation pressure |
| Infection | Pelvic infection uncommon |
| Cervical laceration | From tenaculum or dilation |
| Failure to complete procedure | Cervical stenosis, poor distension, technical difficulty |
| Bowel/urinary tract injury | If perforation with energy device |
| Intrauterine adhesion formation | Post-operative complication of resection procedures |
Complications are more frequent with operative than diagnostic hysteroscopy. The highest-risk procedures are adhesiolysis of severe synechiae and resection of large or deeply intramural leiomyomas.
— Berek & Novak's Gynecology, p. 1371; Tintinalli's Emergency Medicine, Table 105-4
11. Special Situations
Office vs. Operating Room Hysteroscopy
- Most diagnostic hysteroscopies and many operative procedures (polypectomy, small myomectomy Type 0–1, adhesiolysis, septum division, IUD removal) can be performed in the office under local anesthesia with small-diameter scopes
- Operating room under regional or general anesthesia required for: complex adhesiolysis, large or Type 2 myomas, resectoscopic ablation, procedures anticipated to require significant fluid management
Postmenopausal Women
- Higher likelihood of cervical stenosis — pre-treat with vaginal estrogen
- Misoprostol may be less effective for dilation; combine with topical estrogen
- Atrophic endometrium: thin, pale, transparent — recognize as normal in this group
Comparison with Alternative Diagnostic Modalities
| Modality | Advantages | Limitations |
|---|---|---|
| Hysteroscopy (gold standard) | Direct visualization; directed biopsy; simultaneous treatment | Invasive; discomfort; cost |
| SIS (saline infusion sonography) | Non-invasive; evaluates myometrium; comparable accuracy for polyps | Cannot perform biopsy/treatment; no endocervical evaluation |
| HSG | Evaluates tubal patency | Indirect; misses flat lesions; radiation |
| MRI | Best myometrial detail; delineates septum vs. bicornuate | Cost; no tissue sampling |
| Blind endometrial biopsy | Adequate for global hyperplasia/cancer detection | Misses focal lesions (polyps, fibroids) |
12. CPT Procedure Codes (Reference)
| Code | Procedure |
|---|---|
| 58555 | Hysteroscopy, diagnostic |
| 58558 | Hysteroscopy + biopsy/polypectomy ± D&C |
| 58559 | Hysteroscopy + lysis of intrauterine adhesions |
| 58560 | Hysteroscopy + division/resection of intrauterine septum |
| 58561 | Hysteroscopy + removal of leiomyomas |
| 58562 | Hysteroscopy + removal of impacted foreign body |
| 58563 | Hysteroscopy + endometrial ablation, any method |
| 58565 | Hysteroscopic sterilization (Essure) |
— Pfenninger and Fowler's, p. 983
13. Recent Evidence (2023–2026)
| Study | Key Finding | PMID |
|---|---|---|
| Wang et al., Front Endocrinol, 2024 | Meta-analysis: hysteroscopy improves fertility outcomes in infertile women with intrauterine pathology | 39736864 |
| Riemma et al., Am J Obstet Gynecol, 2025 | Systematic review: hysteroscopic criteria for chronic endometritis diagnosis — strawberry pattern, micropolyps, and hyperemia show best diagnostic accuracy | 40073921 |
| Munro et al., Hum Reprod Update, 2025 | Systematic review/meta-analysis: epidemiology and prevention of intrauterine adhesions following surgically induced endometrial trauma — supports strategies to minimize trauma and optimize post-operative care | 40914965 |
Key Takeaways
- Gold standard for uterine cavity evaluation — superior to HSG and comparable to SIS, with the added advantage of simultaneous treatment ("see and treat")
- Office hysteroscopy is feasible and safe for most diagnostic and many operative indications using small-diameter scopes with local anesthesia
- Distension media selection must be matched to the energy system used — isotonic saline for bipolar/diagnostic; electrolyte-free for monopolar RF; strict fluid deficit monitoring is mandatory
- Vaginoscopic (no-touch) approach reduces pain and eliminates the need for tenaculum in most patients
- Complication rate for diagnostic hysteroscopy is very low; operative procedures carry higher risk proportional to the complexity of the procedure and depth of myometrial involvement
- Tissue-specific interpretation is essential — atrophic postmenopausal endometrium, normal proliferative phase, and pathologic conditions all have distinct appearances that guide management
Primary sources: Berek & Novak's Gynecology (9781496380357); Pfenninger and Fowler's Procedures for Primary Care, 3rd ed. (9780323052672); Schwartz's Principles of Surgery, 11th ed.; Tintinalli's Emergency Medicine, 9th ed.
Stage IV Pelvic Endometriosis with Bilateral Ovarian Abscesses
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.