Treatment of mi
Reading File
Finding Sources
Searching PubMed
"myocardial infarction"[MeSH Terms] AND "therapy"[MeSH Terms]
Finding Sources
Searching PubMed
"myocardial infarction" AND treatment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything I need for a comprehensive answer. Here is the full treatment of MI:
Treatment of Myocardial Infarction (MI)
MI is divided into STEMI (ST-elevation MI) and NSTEMI/UA (non-ST-elevation ACS), which differ in urgency and reperfusion strategy.
1. Immediate General Measures (All MI Types)
| Intervention | Details |
|---|---|
| Aspirin | 160-325 mg chewed (buccal absorption) immediately; then 75-162 mg/day orally. Rapid inhibition of COX-1 reduces thromboxane A2. Essential across all ACS. |
| Supplemental O2 | Only if SpO2 <90%. Not recommended routinely when saturations are normal. |
| Nitroglycerin (NTG) | Sublingual 0.4 mg q5 min x3 for ischemic pain; reduces preload and dilates coronary vessels. Avoid if SBP <90 mmHg or suspected RV infarction (inferior STEMI). IV NTG if symptoms return after sublingual. |
| Morphine | For refractory pain (some caution exists due to possible P2Y12 inhibitor interaction). |
| IV access + monitoring | Continuous ECG, vitals, oximetry. |
- Washington Manual of Medical Therapeutics, p. 148-156; Harrison's Principles of Internal Medicine 22E, p. 2160
2. Reperfusion Therapy (STEMI)
This is the cornerstone of STEMI management. "Time is myocardium."
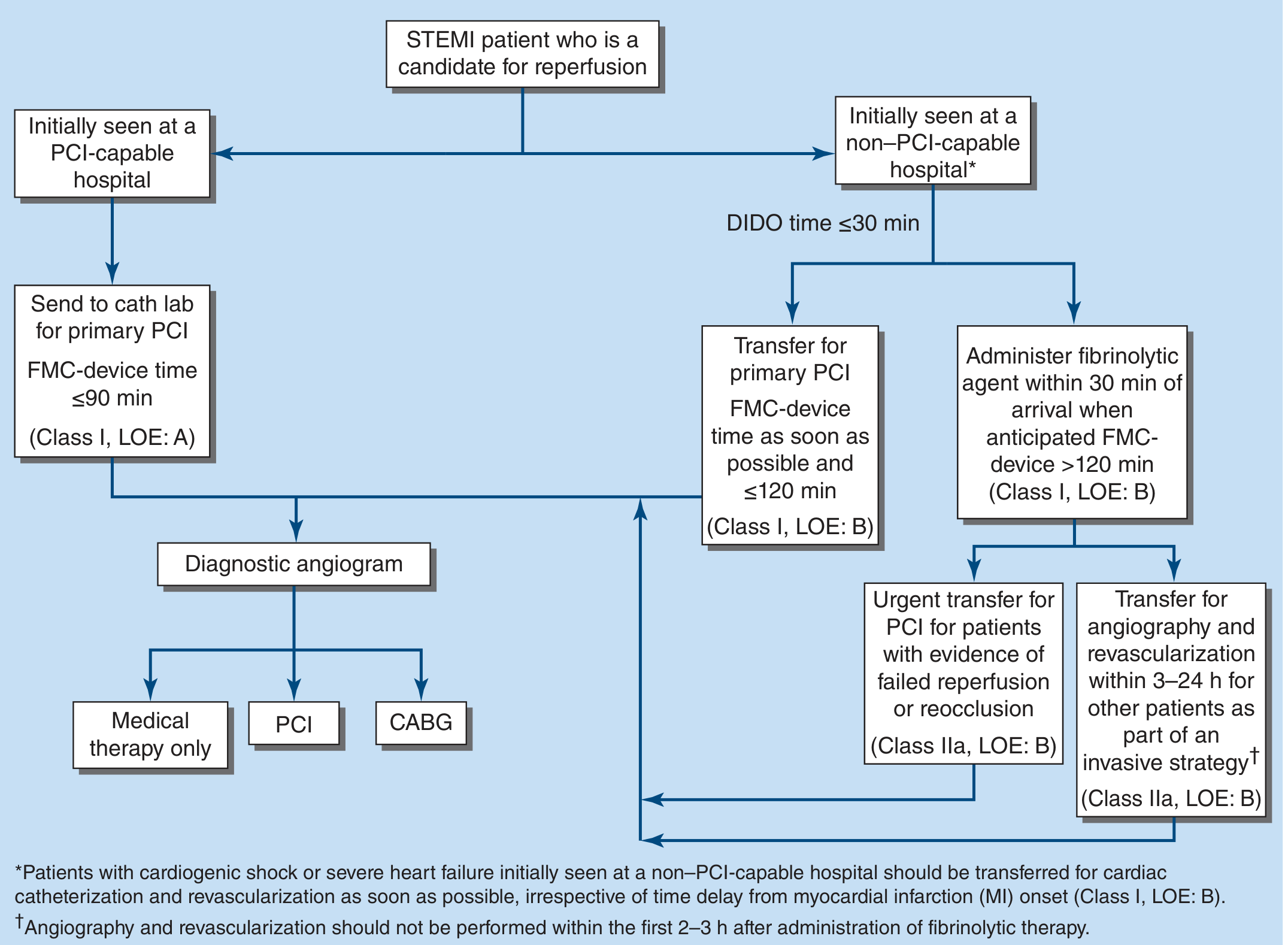
Primary PCI (Preferred)
- Gold standard when available within 90 min of first medical contact (FMC-to-device ≤90 min at PCI-capable center; ≤120 min if transfer required).
- Superior to fibrinolysis: better vessel patency (TIMI 3 flow), less reinfarction, lower intracranial hemorrhage risk, improved survival regardless of age or infarct location.
- Best for symptom onset <12 hours; still offered at 12-24 hours if ongoing symptoms.
- Transradial access is preferred - reduces bleeding and may have a mortality benefit over transfemoral.
- Complete revascularization of non-culprit lesions (either at index procedure or staged) reduces cardiovascular death and future MI.
- CULPRIT-SHOCK exception: In cardiogenic shock, culprit-lesion-only PCI (not multivessel) reduces all-cause mortality and need for renal replacement therapy.
- Coronary stenting (DES preferred) is superior to balloon angioplasty alone.
Fibrinolytic Therapy
- Used when PCI cannot be achieved within 120 min (non-PCI-capable center with anticipated FMC-to-device >120 min).
- Administer within 30 min of hospital arrival ("door-to-needle" ≤30 min).
- Agents: tPA (alteplase), reteplase, tenecteplase (fibrin-specific preferred over streptokinase).
- After successful fibrinolysis: transfer for angiography and revascularization within 3-24 hours.
- Failed reperfusion (persistent ST elevation or hemodynamic instability): urgent transfer for rescue PCI.
Absolute contraindications to fibrinolysis: prior intracranial hemorrhage, ischemic stroke within 3 months, active bleeding, suspected aortic dissection, severe uncontrolled hypertension, intracranial neoplasm.
- Washington Manual of Medical Therapeutics, p. 156; Harrison's 22E, p. 2160-2162
3. Antiplatelet and Anticoagulant Therapy
Dual Antiplatelet Therapy (DAPT)
- Aspirin (see above) +
- P2Y12 inhibitor:
- Ticagrelor 180 mg load then 90 mg BID (preferred in ACS if no contraindication)
- Prasugrel 60 mg load then 10 mg/day (avoid if prior TIA/stroke, age >75, weight <60 kg)
- Clopidogrel 300-600 mg load then 75 mg/day (used when ticagrelor/prasugrel contraindicated, or with fibrinolysis)
- DAPT duration: typically 12 months after ACS/PCI; may be shortened/extended based on bleeding vs. ischemic risk.
- Cessation of P2Y12 inhibitor within 30 days of stent placement carries a 30- to 100-fold increase in stent thrombosis risk.
Anticoagulation (Acute Phase)
- Unfractionated heparin (UFH): IV bolus + infusion; or
- Enoxaparin (LMWH): subcutaneous, often preferred in NSTEMI/UA
- Bivalirudin: direct thrombin inhibitor; alternative in PCI
- Fondaparinux: NSTEMI/medical management; do not use alone for primary PCI
- Anticoagulation is continued until revascularization is complete or through the hospital stay in medically managed patients.
4. Adjunctive Medical Therapy
Beta-Blockers
- Start within 24 hours if no contraindications (HF, low output state, heart block, active bronchospasm).
- Reduce myocardial O2 demand, limit infarct size, reduce ventricular arrhythmias.
- Oral agents preferred (metoprolol, carvedilol); IV beta-blocker if hypertensive or tachycardic without HF.
- Continued indefinitely post-MI for LV dysfunction.
ACE Inhibitors / ARBs
- Start within 24 hours in STEMI, especially anterior MI or EF <40%.
- Prevent ventricular remodeling, reduce mortality.
- ACE inhibitors are "ideal" for long-term management of ventricular dysfunction after STEMI.
- Use ARB if ACE inhibitor intolerant.
- Aldosterone antagonist (eplerenone/spironolactone): add if EF ≤40% with symptomatic HF or diabetes; monitor K+ and renal function.
Statins (High-Intensity)
- Start in-hospital regardless of baseline LDL.
- Atorvastatin 40-80 mg or rosuvastatin 20-40 mg.
- Fasting lipid panel recommended as baseline (note: lipids may fall in first 24-48 hours post-MI).
Nitrates
- Long-term oral nitrates for ongoing angina or HF symptoms.
- Not for routine use post-MI without ongoing ischemia or HF.
5. Management of Specific Complications
Cardiogenic Shock (Killip Class IV)
- Defined by hypotension + evidence of end-organ hypoperfusion.
- Occurs when ≥40% of LV myocardium is infarcted.
- Primary PCI is always preferred even with time delays.
- Inotropes: dobutamine (improves contractility, reduces peripheral resistance).
- Mechanical circulatory support: IABP, Impella, ECMO.
- Swan-Ganz catheter for hemodynamic monitoring in refractory cases.
- In cardiogenic shock with multivessel disease: culprit-only PCI first (CULPRIT-SHOCK trial).
Right Ventricular (RV) Infarction
- Occurs with proximal RCA occlusion causing inferior STEMI.
- Classic triad: hypotension + elevated JVP + clear lung fields.
- ECG: ST elevation ≥1 mm in V1 or V4R lead.
- Management: IV fluids (RV is preload-dependent); avoid nitrates and diuretics.
- If unresponsive: dobutamine + IABP; right-sided mechanical support if needed.
- Temporary pacing if AV block present.
Heart Failure Post-MI
- Loop diuretics (furosemide IV) for pulmonary congestion.
- Nitrates to reduce preload without reducing plasma volume.
- ACE inhibitors for long-term LV dysfunction.
- Digitalis is not useful in post-MI HF.
Arrhythmias
- VF/VT: immediate defibrillation; IV amiodarone or lidocaine for recurrent VT.
- Complete heart block (especially inferior MI - RCA): temporary pacing; resolves in most.
- AF: rate control with beta-blockers; anticoagulation per CHA2DS2-VASc.
LV Thrombus
- Risk in anterior MI with apical akinesis.
- Anticoagulate if thrombus detected.
- Warfarin not routinely prescribed for apical hypokinesis without confirmed thrombus (increased bleeding and death without clear benefit).
6. NSTEMI / Unstable Angina Management
| Strategy | When |
|---|---|
| Early invasive (angiography within 24-48 h) | High-risk: elevated troponins, dynamic ECG changes, TIMI/GRACE score elevated, refractory symptoms |
| Selective invasive (ischemia-guided) | Low-risk, stable patients |
- Same antiplatelet + anticoagulant therapy as STEMI.
- No role for immediate fibrinolysis in NSTEMI.
7. Secondary Prevention (Discharge Medications - "ABCDE")
| Letter | Drug Class | Goal |
|---|---|---|
| A | Aspirin + P2Y12 (DAPT) | Prevent stent thrombosis and recurrent ACS |
| A | ACE inhibitor/ARB | LV remodeling prevention |
| B | Beta-blocker | Reduce mortality, arrhythmia |
| C | Cholesterol (statin, high-intensity) | LDL reduction, plaque stabilization |
| D | Diabetes management / Diet | Modify risk factors |
| E | Exercise rehabilitation | Cardiac rehab program |
Cardiac rehabilitation reduces mortality by ~20-25% and improves functional capacity.
8. CABG
Indicated when:
- Anatomy is unsuitable for PCI (left main disease, multivessel disease with complex anatomy, especially in diabetics).
- Failed PCI with ongoing ischemia.
- Mechanical complications requiring surgical repair (VSR, papillary muscle rupture).
Key Time Targets Summary
| Target | Goal |
|---|---|
| FMC-to-balloon (primary PCI) | ≤90 min (PCI center) / ≤120 min (transfer) |
| Door-to-needle (fibrinolysis) | ≤30 min |
| PCI after fibrinolysis | 3-24 hours (successful lysis) |
| Rescue PCI (failed lysis) | Immediately / urgently |
- Harrison's Principles of Internal Medicine 22E (2025), p. 2160-2170
- Goldman-Cecil Medicine, p. 3557-3560
- Washington Manual of Medical Therapeutics, p. 148-162
This is a shared conversation. Sign in to Orris to start your own chat.