Respiratory anatomy of lungs
Reading File
Finding Sources
Finding Sources
Searching the Web
respiratory anatomy of lungs lobes bronchi alveoli overview
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive content and all key diagrams. Let me compose a thorough, well-illustrated answer.
Respiratory Anatomy of the Lungs
Overview of Respiratory Regions
The respiratory system is divided into three interconnected regions:
- Upper airway - nose/nasal cavity, mouth, pharynx, larynx
- Conducting airway - trachea down to terminal bronchioles (first 16 generations)
- Alveolar (respiratory) airway - respiratory bronchioles, alveolar ducts, alveolar sacs
The upper airway filters particles >30-50 µm, warms and humidifies air. Smaller particles (5-10 µm) enter the conducting airway and settle on mucous membranes. - Ganong's Review of Medical Physiology, p. 621
Lobes and Fissures
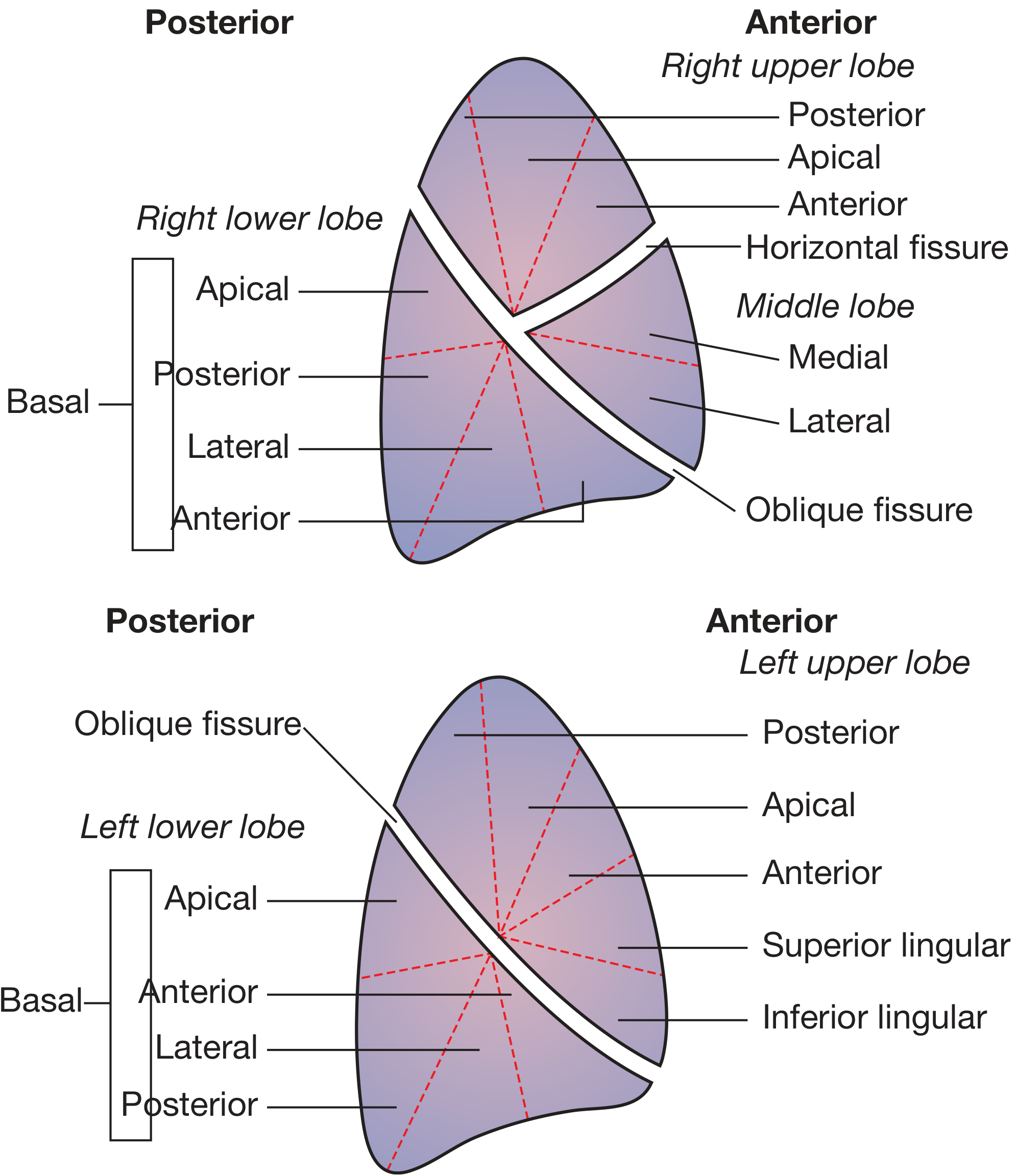
Figure: Lobar and segmental divisions of the lungs - right lung (above) and left lung (below), viewed from the side. (Bailey & Love's Short Practice of Surgery, 28th ed., Fig. 60.1)
Right lung - three lobes:
- Upper lobe (3 segments: apical, posterior, anterior)
- Middle lobe (2 segments: medial, lateral)
- Lower lobe (5 segments: apical, anterior/posterior/lateral/medial basal)
- Separated by the oblique fissure (lower vs upper+middle) and the horizontal fissure (upper vs middle)
Left lung - two lobes:
- Upper lobe (includes the lingula - the equivalent of the right middle lobe, with superior and inferior lingular segments)
- Lower lobe (4-5 segments)
- Separated only by the oblique fissure, which lies closer to vertical than horizontal - making the upper and lower lobes functionally anterior and posterior
The right lung has 10 bronchopulmonary segments; the left has 8 (though some British nomenclature recognizes 10 on the left as well). - Fischer's Mastery of Surgery, 8th ed., p. 2217
Bronchial Tree
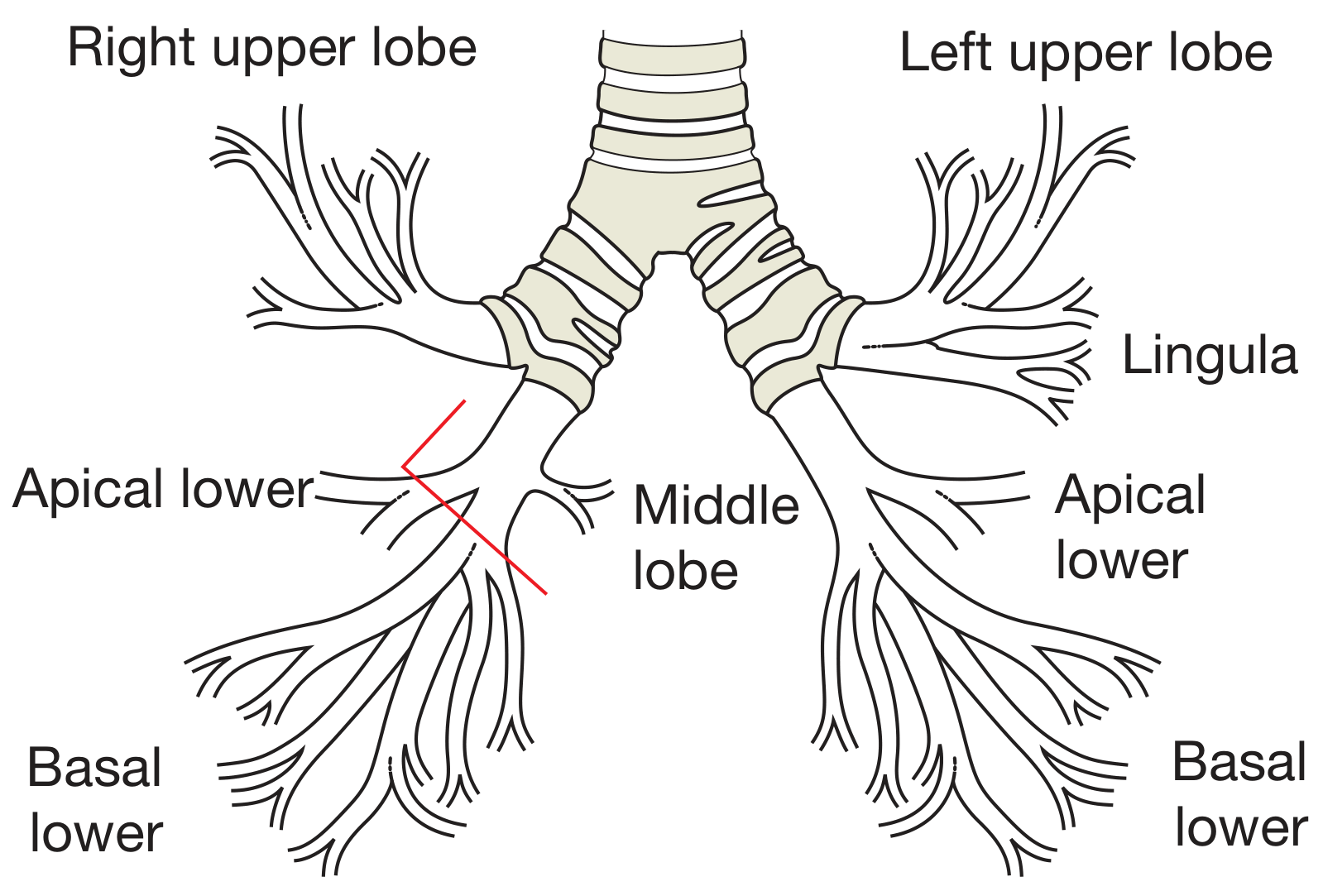
Figure: Surgical anatomy of the bronchial tree. The red line marks the apical bronchial segment of the right lower lobe, important for lobe-sparing surgery. (Bailey & Love's, Fig. 60.2)
Key bronchial anatomy:
-
The right main bronchus (RMB) is shorter, wider, and nearly vertical compared to the left - so inhaled foreign bodies preferentially enter the right side
-
The left main bronchus (LMB) is longer and more horizontal
-
The trachea and bronchi have a systemic blood supply from the bronchial arteries, which arise directly from the thoracic aorta
-
Lymphatic drainage follows the bronchi; nodes are organized by numbered stations and zones (important in lung cancer staging)
-
Bailey & Love's Short Practice of Surgery, 28th ed., p. 996
Conducting Zone: Airway Architecture
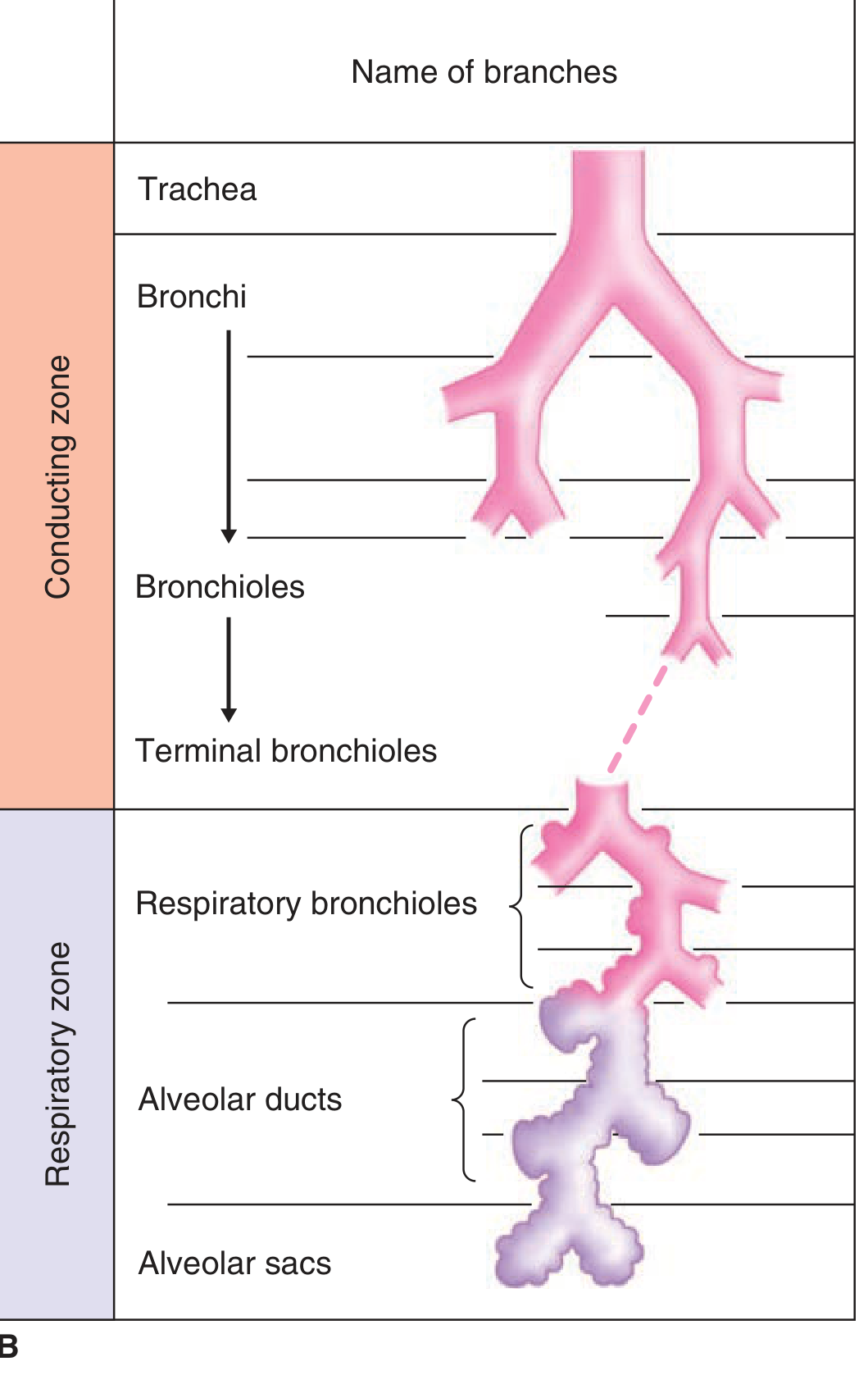
Figure: Conducting zone (trachea → bronchi → bronchioles → terminal bronchioles) and respiratory zone (respiratory bronchioles → alveolar ducts → alveolar sacs). (Ganong's, Fig. 34-1B)
The conducting airway starts at the trachea and branches dichotomously through 16 generations before reaching the respiratory zone. Each generation greatly expands the total surface area. Structural features by zone:
| Structure | Cartilage | Glands | Smooth Muscle | Epithelium |
|---|---|---|---|---|
| Trachea/Bronchi | Yes (rings/plates) | Yes (submucosal) | Present | Pseudostratified ciliated |
| Bronchioles | Absent | Absent | Prominent | Cuboidal |
| Terminal bronchioles | Absent | Absent | Prominent | Cuboidal + Club cells |
| Respiratory bronchioles | Absent | Absent | Present | Squamous (transitional) |
| Alveoli | Absent | Absent | Absent | Squamous (Type I & II) |
Club cells (formerly Clara cells) - non-ciliated cuboidal epithelial cells in the distal conducting airway that secrete defense markers and serve as progenitor cells for repair after injury. - Ganong's, p. 622
Mucociliary escalator: The ciliary mechanism moves particles away from the lungs at ≥16 mm/min. Impaired ciliary function (smoking, genetic defects like in cystic fibrosis) leads to chronic sinusitis, recurrent infection, and bronchiectasis.
Histological Transition: Trachea to Alveolus
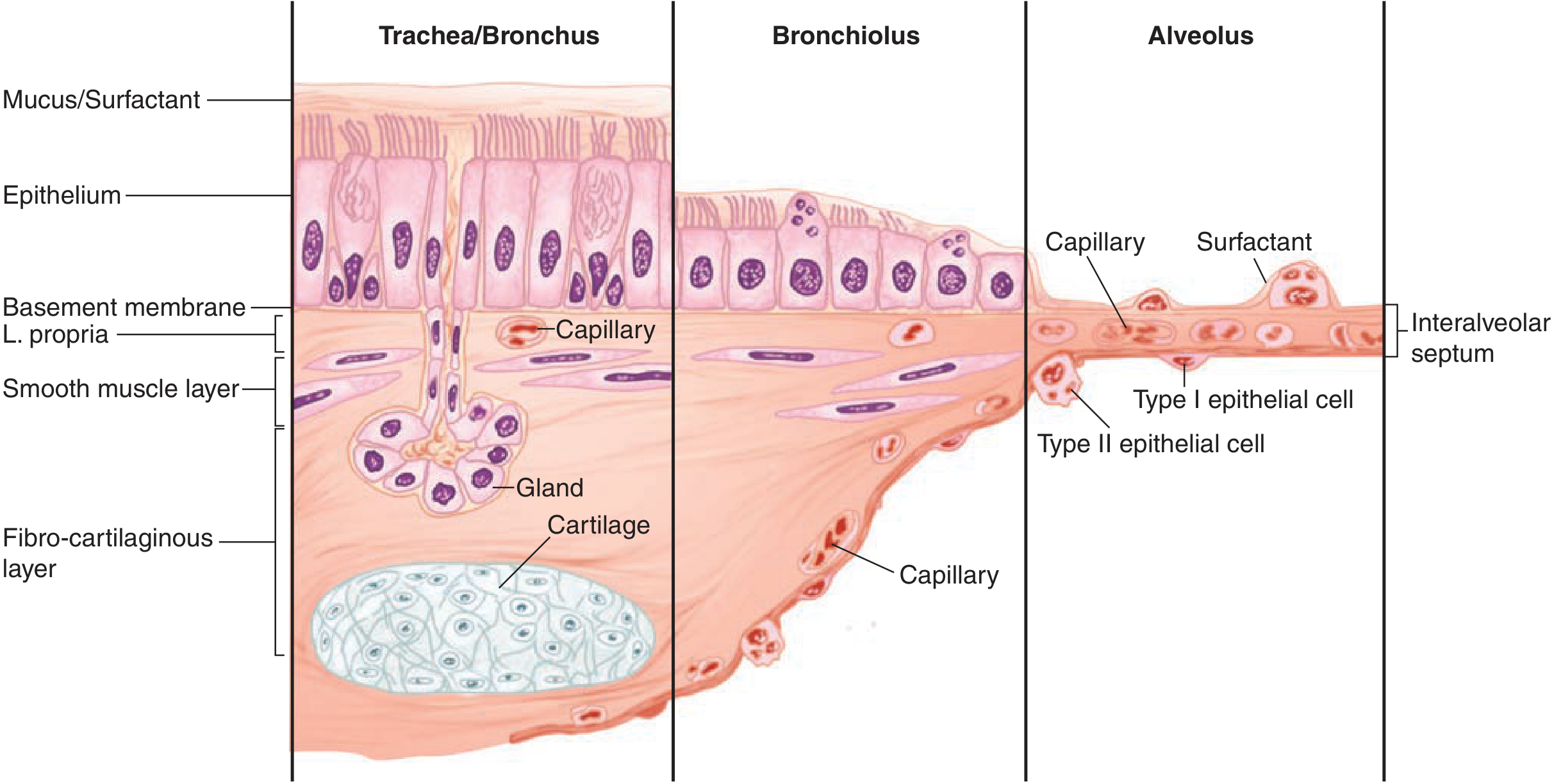
Figure: Cellular transition from conducting airway to alveolus. Epithelium changes from pseudostratified (trachea/bronchus) to cuboidal (bronchiolus) to squamous (alveolus). Cartilage and glands are lost as the airway progresses distally. (Ganong's, Fig. 34-2)
Alveolar (Respiratory) Zone
Between the trachea and the ~300 million alveoli in the adult human lung, there are approximately 23 generations of branching in total. The respiratory zone begins at the respiratory bronchioles, which have alveoli budding from their walls.
Alveolar cells:
- Type I pneumocytes - flat squamous cells, cover ~95% of alveolar surface, responsible for gas exchange
- Type II pneumocytes - cuboidal cells, secrete surfactant (reduces surface tension, prevents alveolar collapse), also serve as progenitor cells for type I repair
- Alveolar macrophages - roam the alveolar surface as the primary phagocytic defense
The interalveolar septum contains type I cells, a basement membrane, capillary endothelium, and surfactant - the blood-gas barrier for O₂/CO₂ exchange is only ~0.5 µm thick.
Hilar Anatomy
The hilum is where the structures enter and exit each lung. Key relationships:
Right hilum (anterior to posterior):
- Pulmonary veins (most anterior, course inferiorly and medially)
- Pulmonary artery (intermediate, transverse course)
- Bronchus (most posterior, course superolaterally)
Left hilum:
- Main pulmonary artery is superior to the bronchus, arching over it before dividing
- Pulmonary veins are anterior and inferior
- Bronchus is posterior
The right phrenic nerve runs in the mediastinal adventitia anterior to the hilum (anterior to the SVC and pericardium) - it is in a different tissue plane from the lung root and must not be inadvertently retracted. The vagus nerve travels posteriorly near the tracheal bifurcation and is associated with the esophagus below; it contributes to pulmonary plexuses. - Fischer's Mastery of Surgery, 8th ed., p. 2213
The azygos vein on the right arches from the posterior mediastinum to the SVC just above the right hilum.
Bronchopulmonary Segments
Segments are the surgical units of the lung - there is little to no communication between adjacent segments at the bronchial level (though cross-ventilation occurs at the parenchymal level). Each segment has:
- Its own segmental (3rd order) bronchus
- Its own branch of the pulmonary artery
- Pulmonary veins that are intersegmental (running between segments, not within them)
This intersegmental venous drainage is why pulmonary veins serve as reliable planes of surgical dissection between segments.
Mechanics of Breathing
Inspiration is an active process:
- Intercostal muscles contract → ribs move upward and outward → increases transverse and anteroposterior dimensions
- Diaphragm contracts and flattens → increases vertical chest cavity dimension
- Accessory muscles (sternocleidomastoid, scalenes, spinal muscles) recruited during exercise or respiratory distress
Expiration at rest is passive (elastic recoil), but becomes active during forced expiration or disease. - Bailey & Love's, p. 996
Autonomic Innervation
The bronchial walls receive autonomic innervation:
- β₂ adrenergic receptors mediate bronchodilation and increase bronchial secretions
- α₁ adrenergic receptors inhibit secretions
- Airway sensory neurons respond to dusts, cold air, noxious gases, and smoke - triggering cough and sneeze reflexes via the respiratory centers
Sources:
- Ganong's Review of Medical Physiology, 26th ed., pp. 621-623
- Bailey & Love's Short Practice of Surgery, 28th ed., pp. 995-996
- Fischer's Mastery of Surgery, 8th ed., pp. 2213-2218
This is a shared conversation. Sign in to Orris to start your own chat.