Diarrhoea
Reading File
Finding Sources
Searching PubMed
"diarrhea"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I have comprehensive content now. Let me compile the full, detailed response.
Diarrhoea
Definition
Diarrhoea is defined as the passage of 3 or more loose or watery stools per day, or more frequently than is normal for the individual. A more precise stool-weight definition used in clinical research is >200 g/day in Western populations. The term derives from the Greek "to run through."
Duration defines the clinical subtype:
- Acute diarrhoea - <2 weeks
- Persistent diarrhoea - 2-4 weeks
- Chronic diarrhoea - >4 weeks (affects ~6.6% of the adult population at any given time)
(Sleisenger and Fordtran's Gastrointestinal and Liver Disease)
Pathophysiology
Normal intestinal fluid balance involves approximately 9 litres entering the gut daily (2 L oral intake + 7 L secretions), with all but ~100-200 mL being absorbed. Diarrhoea results from any disruption in this balance. Four major mechanisms operate:
1. Osmotic Diarrhoea
Non-absorbable solutes in the lumen retain water osmotically. Classic example: lactase deficiency, where undigested lactose remains in the gut and draws water in. Key feature: stops with fasting. The osmotic gap is elevated (stool osmotic gap >125 mOsm/kg).
2. Secretory Diarrhoea
Active ion secretion into the lumen exceeds absorptive capacity. The prototype is cholera, where the toxin enters crypt epithelial cells, activates adenylyl cyclase via the Gs protein, raises cAMP, and opens apical Cl⁻ channels. Na⁺ and H₂O follow passively:
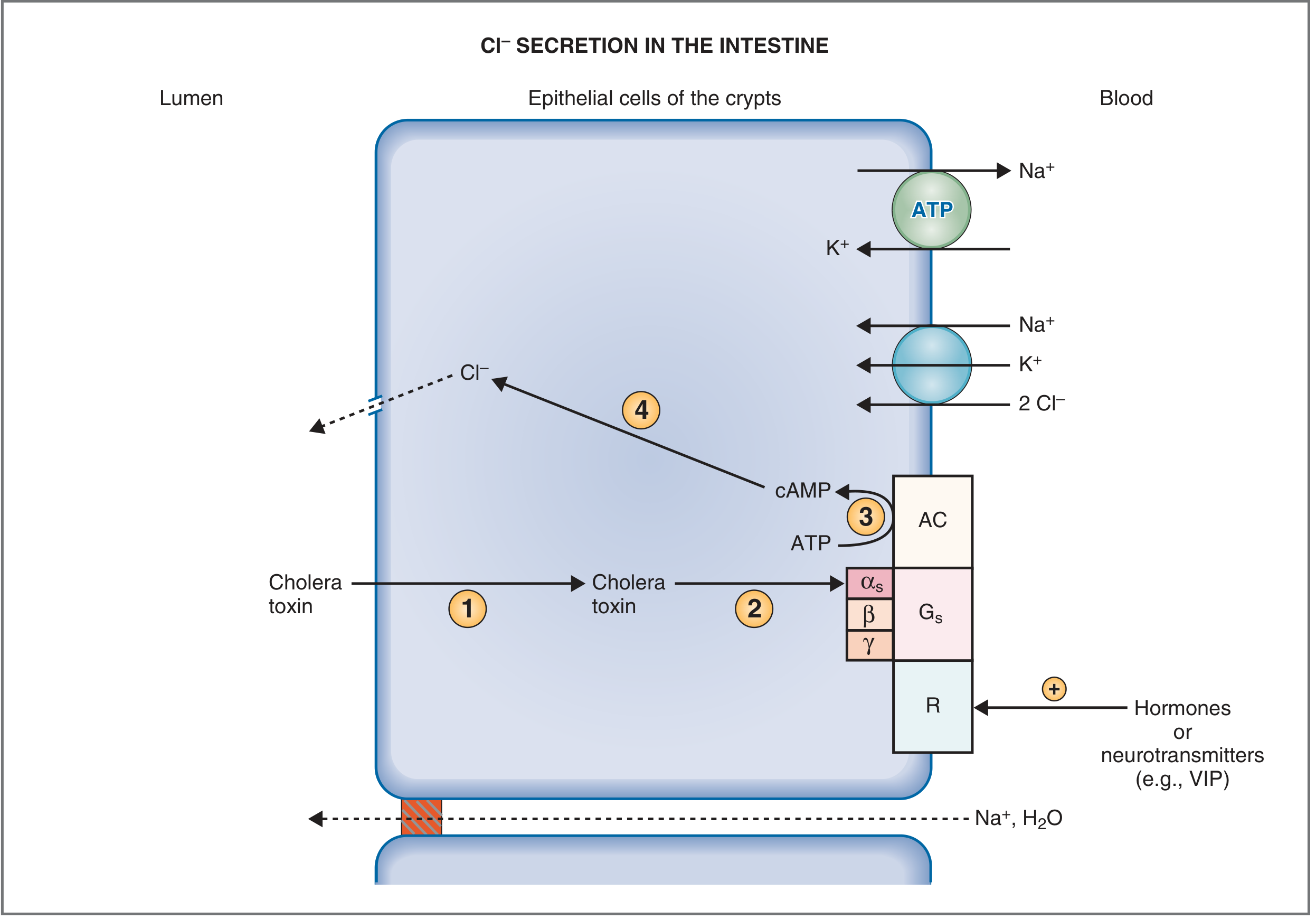
Fig: Mechanism of Cl⁻ and fluid secretion. Cholera toxin activates adenylyl cyclase, raises cAMP, and opens apical Cl⁻ channels. VIP and other hormones use the same pathway. (Costanzo Physiology, 7th Ed.)
Key feature: persists with fasting, large-volume, no osmotic gap.
3. Reduced Absorptive Surface Area
Infection, inflammation (celiac disease, IBD), or surgical resection reduces surface area available for absorption. Ileocecal resection permanently impairs NaCl absorption against a concentration gradient that no other bowel segment can compensate for.
4. Abnormal Motility
- Rapid transit ("intestinal hurry") - oral-cecal transit may be as short as 10 minutes, preventing adequate absorption. Seen in diabetic autonomic neuropathy, post-vagotomy, hyperthyroidism
- Slow transit - promotes small intestinal bacterial overgrowth (SIBO), causing secondary secretory diarrhoea (e.g., scleroderma)
(Sleisenger and Fordtran's)
Electrolyte Consequences
Diarrhoeal fluid is rich in HCO₃⁻ (from pancreatic/intestinal secretions) and K⁺ (colonic flow-rate-dependent secretion). Consequences:
- Metabolic acidosis - hyperchloraemic, normal anion gap (loss of HCO₃⁻)
- Hypokalemia - K⁺ loss in stool
- Volume depletion / circulatory collapse - in severe cases (e.g., cholera)
Clinical Classification
By Duration
| Type | Duration | Common Causes |
|---|---|---|
| Acute | <2 weeks | Infection (viral, bacterial, parasitic), food poisoning, medications |
| Persistent | 2-4 weeks | May indicate ongoing infection or early chronic disease |
| Chronic | >4 weeks | IBD, IBS, malabsorption, endocrinopathy, neoplasia |
By Stool Character (Watery / Fatty / Inflammatory)
Watery diarrhoea - either osmotic or secretory. Large-volume if small bowel origin; small-volume if colonic.
Fatty (steatorrhoeic) diarrhoea - pale, bulky, offensive, floats. Indicates:
- Malabsorption: celiac disease, Whipple disease, short bowel syndrome
- Maldigestion: pancreatic exocrine insufficiency, inadequate bile acids, SIBO
Inflammatory diarrhoea - mucus, pus, blood ("dysentery"). Indicates mucosal ulceration:
- IBD (Crohn disease, ulcerative colitis)
- Infectious: Shigella, Campylobacter, C. difficile, CMV, E. histolytica, tuberculosis
- Ischaemic colitis, colon cancer
Differential Diagnosis
Acute Diarrhoea
- Infections (most common): rotavirus, norovirus, Salmonella, Shigella, Campylobacter, C. difficile, E. coli (ETEC, EHEC)
- Food allergies / food poisoning
- Medications (antibiotics, laxatives, metformin, NSAIDs, immune checkpoint inhibitors)
- Initial presentation of a chronic disorder
Chronic Watery Diarrhoea
Secretory causes:
- Endocrinopathies: VIPoma, gastrinoma (ZES), carcinoid syndrome, medullary thyroid carcinoma, phaeochromocytoma, Addison disease, hyperthyroidism
- Microscopic colitis (collagenous or lymphocytic)
- IBD
- Ileal bile acid malabsorption
- IBS-D, functional diarrhoea
- Brainerd (epidemic secretory) diarrhoea
Osmotic causes:
- Carbohydrate malabsorption (lactase deficiency, fructose)
- Osmotic laxatives (Mg²⁺, PO₄³⁻, SO₄²⁻)
Chronic Fatty Diarrhoea
- Malabsorption: celiac disease, tropical sprue, Whipple disease, short bowel syndrome, SIBO
- Maldigestion: chronic pancreatitis, cystic fibrosis, cholestasis
Chronic Inflammatory Diarrhoea
- Crohn disease, ulcerative colitis
- Microscopic colitis
- Radiation enteritis
- Vasculitis
- Colon carcinoma, lymphoma
(Sleisenger and Fordtran's, Box 16.2)
Evaluation
History
Key questions: onset and duration, stool frequency/consistency/volume, blood or mucus, associated symptoms (fever, vomiting, weight loss, tenesmus), travel history, dietary history, medications, immunosuppression, sexual history, family history of IBD.
"Alarm features" prompting urgent workup:
- Blood in stool
- Nocturnal diarrhoea (waking from sleep)
- Unintentional weight loss >5 kg
- Fever >38.5°C
- Duration >4 weeks
- Age >50, or family history of colorectal cancer/IBD
Physical Examination
- Hydration status (skin turgor, mucous membranes, capillary refill, BP/HR)
- Abdominal tenderness, distension, bowel sounds
- Rectal examination
- Signs of systemic disease (goitre, flushing, lymphadenopathy)
Investigations
Acute diarrhoea (most is self-limited - no tests needed):
- Stool culture + microscopy if: bloody stool, fever, immunocompromised, traveller, >7 days duration, community outbreak
- C. difficile toxin PCR if: recent antibiotics or hospitalisation
Chronic diarrhoea:
| Investigation | Purpose |
|---|---|
| FBC, CRP, ESR | Inflammation |
| TSH | Hyperthyroidism |
| Coeliac serology (anti-TTG IgA) | Celiac disease |
| Stool calprotectin | IBD vs functional |
| Stool fat / 72-hr collection | Steatorrhoea |
| Colonoscopy + biopsy | IBD, microscopic colitis, neoplasia |
| Upper GI endoscopy + duodenal biopsy | Celiac disease, Whipple disease |
| Hydrogen breath test | SIBO, lactose intolerance |
| Urine 5-HIAA, serum VIP, gastrin, calcitonin | Secreting tumours |
| CT abdomen/pelvis | Pancreatic disease, lymphoma, neoplasia |
Treatment
Acute Diarrhoea
Rehydration is the cornerstone. Oral rehydration solution (ORS) replaces fluid, Na⁺, K⁺, and HCO₃⁻. WHO/UNICEF standard ORS contains 75 mmol/L sodium, 75 mmol/L glucose, 20 mmol/L potassium, 30 mmol/L bicarbonate.
Loperamide (opioid receptor agonist at myenteric plexus): reduces motility and secretion. Use in non-bloody, non-febrile traveller's diarrhoea. Avoid in suspected inflammatory/invasive diarrhoea (risk of toxic megacolon).
Antibiotics: indicated for:
- Traveller's diarrhoea (azithromycin, rifaximin)
- Suspected Shigella (azithromycin, ciprofloxacin)
- C. difficile - oral vancomycin or fidaxomicin (metronidazole no longer first-line for severe disease)
- Giardia - metronidazole or tinidazole
- E. histolytica - metronidazole 750 mg q8h + luminal amebicide (iodoquinol or paromomycin)
- Cryptosporidium in immunocompetent - nitazoxanide 500 mg BD
- Cyclospora - trimethoprim-sulfamethoxazole
Zinc supplementation in children (20 mg/day x 10-14 days) - reduces duration and severity, recommended by WHO. A recent systematic review (Ali et al., 2024) confirms benefit for acute and persistent watery diarrhoea.
Probiotics - a 2025 meta-analysis (Alsabri et al.) found probiotics reduce duration and severity of acute gastroenteritis in children.
Chronic Diarrhoea
Treatment is directed at the underlying cause:
- IBD: mesalazine, corticosteroids, immunomodulators, biologics
- Celiac disease: gluten-free diet
- Microscopic colitis: budesonide
- Bile acid diarrhoea: cholestyramine, colesevelam
- IBS-D: low-FODMAP diet, loperamide, rifaximin, tricyclic antidepressants
- VIPoma/carcinoid: somatostatin analogues (octreotide)
- Pancreatic exocrine insufficiency: pancreatic enzyme replacement
- SIBO: rifaximin, rotating antibiotics
Special Scenarios
Diarrhoea in HIV/AIDS
Pre-HAART: occurred in up to 90% of patients. Now more often HAART-induced or unrelated to HIV. Main pathogens depend on CD4 count: Cryptosporidium, Microsporidium, MAC, CMV, C. difficile. (Sleisenger and Fordtran's)
Traveller's Diarrhoea
Most common illness in travellers. Usually ETEC, but also Campylobacter, Shigella, norovirus. Self-limited in 3-5 days. Azithromycin is preferred (ciprofloxacin resistance rising in South/SE Asia).
Paediatric Diarrhoea
Leading cause of death in children under 5 in low-income countries. Rotavirus is the most common severe cause globally; rotavirus vaccine has dramatically reduced burden. Management: ORS + zinc + continued feeding. (Rosen's Emergency Medicine)
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Costanzo Physiology, 7th Ed.; Rosen's Emergency Medicine; Harriet Lane Handbook, 23rd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.