Umbilical hernia repair
Reading File
Finding Sources
Searching PubMed
"umbilical hernia"[MeSH Terms] AND "herniorrhaphy"[MeSH Terms]
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of umbilical hernia repair drawn from Bailey & Love's Short Practice of Surgery (28th ed.) and Mulholland & Greenfield's Surgery (7th ed.).
Umbilical Hernia Repair
Background & Anatomy
Umbilical hernias result from failure of the umbilical ring to close after birth, or — in adults — from acquired weakening of the linea alba. The hernia neck is relatively narrow in relation to the sac size, making these hernias prone to incarceration, obstruction, and strangulation.
Predisposing factors (adults): obesity, multiple pregnancies, cirrhosis with ascites, large intra-abdominal tumors. Peak incidence of repair is around age 60. Male gender is a risk factor, but women are more frequently affected overall.
Differential diagnosis includes caput medusae (portal hypertension varicosities around the umbilicus) and Sister Mary Joseph's nodule (metastatic deposit).
Indications for Surgery
| Indication | Action |
|---|---|
| Hernia containing bowel | Surgery advised due to strangulation risk |
| Symptomatic (pain, obstruction) | Elective repair |
| Small asymptomatic hernia | May observe — can enlarge |
| Incarceration / strangulation | Emergency repair |
Children: ~80% close spontaneously by age 2; elective repair deferred to ~5 years of age. Early repair if incarceration occurs (rare) or the hernia is very large/distressing.
Pregnancy: Surgery strongly avoided before or during pregnancy; postpartum hernias may resolve with weight loss, pelvic floor exercises, and improved abdominal tone.
Open Repair
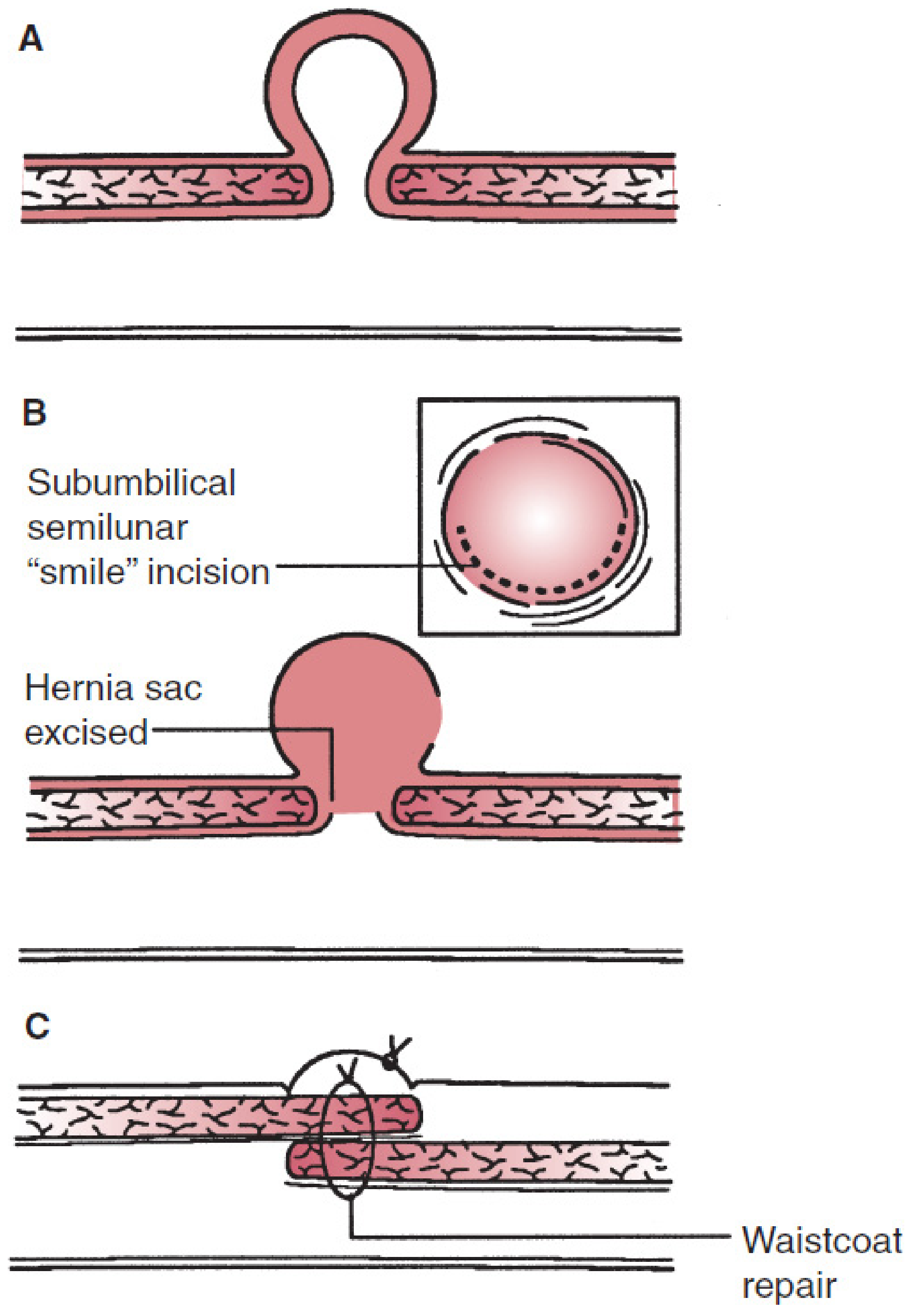
Mayo repair: A) defect, B) subumbilical "smile" incision with hernia sac excised, C) waistcoat-over-trousers (overlapping) fascial closure.
Defect < 1 cm
- Simple suture repair provided closure is tension-free.
- Alternatively, a darn repair: non-absorbable monofilament criss-crossed across the defect and anchored to fascia circumferentially.
Defects ≤ 2 cm — Mayo Repair
- Transverse incision over the hernia.
- Sac dissected, opened, contents reduced; peritoneum closed.
- Linea alba defect extended transversely.
- Fascial edges overlapped — superior flap over inferior ("waistcoat over trousers").
- Closed with non-absorbable sutures; redundant skin excised for cosmesis.
Mesh Use (Current Evidence)
Current evidence recommends mesh even for small defects, and mandatorily for all defects > 2 cm, due to high recurrence rates with suture-only repair. Options include:
- Onlay mesh (over closed fascia)
- Sublay / retromuscular mesh (preferred — reduces recurrence)
- Intraperitoneal mesh (requires tissue-separating, non-adherent mesh)
Laparoscopic Repair
Setup: Camera port + 2 lateral working ports, placed well away from the defect.
Steps:
- Hernia contents reduced by traction and external pressure.
- Falciform ligament (above) and median umbilical fold (below) may be taken down to create a smooth surface for mesh.
- Non-adherent intraperitoneal mesh disc introduced and centred over the defect.
- Fixed to peritoneum/posterior rectus sheaths with staples, tacks, or sutures.
Advantages: Fewer wound complications, allows large mesh overlap, preferred for:
- Obese patients
- Concomitant rectus divarication
- Multiple ventral defects
Disadvantages: Requires specialised equipment, expensive tissue-separating mesh, risk of bowel adhesions/erosion/fistulation. Intraperitoneal mesh can cause severe pain for 24–48 h post-op (can mimic peritonitis).
Emergency Repair
Indications: Incarceration, bowel obstruction, strangulation — driven by the narrow fibrous defect edge.
Key points:
- Delay leads to omental or bowel gangrene.
- Large hernias are often multiloculated — strangulated bowel may be in one loculus while others appear soft and non-tender; inspect all loculi.
- Most emergency repairs are open.
- If bowel is viable: reduce and proceed with repair.
- If bowel is non-viable: resect, close bowel ends (avoid mesh in contaminated field if possible), repair defect primarily or with biosynthetic mesh.
Special Circumstances
Cirrhosis with Ascites
- Very high perioperative mortality/morbidity (especially Child's B & C).
- Careful patient selection and hepatology support are essential.
- Control ascites medically before surgery where possible.
- Fascial repair with fine continuous sutures to minimise risk of post-op ascites leakage.
- Topical fibrin sealant has been used for leaking umbilical hernias with ascites.
Mesh Repair Options Summary
| Technique | Position | Notes |
|---|---|---|
| Onlay | Anterior to fascia | Simple but higher infection risk |
| Sublay (retromuscular) | Behind posterior rectus sheath | Preferred; low recurrence |
| IPOM (Intraperitoneal Onlay Mesh) | Inside peritoneal cavity | Used laparoscopically; requires non-adherent mesh |
Recurrence
Suture-only repair (especially Mayo) carries significant recurrence, particularly for defects > 2 cm. Mesh reinforcement substantially reduces recurrence. Obesity and ongoing elevated intra-abdominal pressure (uncontrolled ascites) are the main modifiable risk factors.
Sources: Bailey and Love's Short Practice of Surgery, 28th ed., Ch. 64; Mulholland & Greenfield's Surgery, 7th ed., Ch. 72
This is a shared conversation. Sign in to Orris to start your own chat.