abg analysis from basic to clinicals
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Now I have comprehensive data. Let me compile the full, structured ABG analysis guide.
Arterial Blood Gas (ABG) Analysis: Basic to Clinical
1. What Is an ABG?
An arterial blood gas sample measures the partial pressures of oxygen and carbon dioxide, the pH, and the bicarbonate concentration in arterial blood. Together these values give you a real-time snapshot of a patient's respiratory function and acid-base status. The sample is drawn from a peripheral artery (most commonly the radial artery) and must be analyzed quickly to avoid gas equilibration changes.
2. Normal Values (Memorize These)
| Parameter | Normal Range |
|---|---|
| pH | 7.35 - 7.45 |
| PaCO2 | 35 - 45 mmHg |
| PaO2 | 80 - 100 mmHg |
| HCO3- | 22 - 26 mEq/L |
| SaO2 | 95 - 100% |
| Base Excess (BE) | -2 to +2 mEq/L |
- pH < 7.35 = acidemia
- pH > 7.45 = alkalemia
3. The Henderson-Hasselbalch Equation
This is the foundation of ABG interpretation:
pH = pKa + log ( [HCO3-] / α·PCO2 )
Where α = 0.0307 (CO2 solubility coefficient), pKa = 6.1.
The Kassirer-Bleich approximation is the quick bedside version:
[H+] = 24 × PCO2 / [HCO3-]
Units: H+ in nmol/L, PCO2 in mmHg, HCO3- in mEq/L. Use this to cross-check reported values:
- [H+] of 25 ≈ pH 7.6
- [H+] of 40 ≈ pH 7.4
- [H+] of 63 ≈ pH 7.2
(Murray & Nadel's Textbook of Respiratory Medicine)
4. The CO2-Bicarbonate Buffer System
This is the body's most important extracellular buffer:
CO2 + H2O ⇌ H2CO3 ⇌ H+ + HCO3-
- The lungs control CO2 (the respiratory component)
- The kidneys control HCO3- (the metabolic component)
- Carbonic anhydrase (CA) catalyzes this reaction in red blood cells, vascular endothelium, and renal tubules
The ratio [HCO3-] / [dissolved CO2] is normally 20:1, which keeps pH near 7.4. As long as this ratio is maintained at 20:1, the pH stays normal regardless of absolute values (a concept called the isohydric principle).
5. A Systematic 5-Step Approach to ABG Interpretation
Step 1 - Determine the pH status
- < 7.35 → acidemia
-
7.45 → alkalemia
- 7.35-7.45 → normal (but a disorder may still be present - check the other values)
Step 2 - Identify the primary disorder
Look at pH direction and match it with PCO2 or HCO3-:
| pH | Primary change | Disorder |
|---|---|---|
| Low | PCO2 high | Respiratory acidosis |
| High | PCO2 low | Respiratory alkalosis |
| Low | HCO3- low | Metabolic acidosis |
| High | HCO3- high | Metabolic alkalosis |
Step 3 - Assess compensation
The body always compensates in the direction that moves pH back toward normal but never overcorrects. Use these formulas:
| Primary Disorder | Expected Compensation |
|---|---|
| Metabolic acidosis | ΔPCO2 = 1.3 × ΔHCO3- (Winter's formula) |
| Metabolic alkalosis | ΔPCO2 = 0.6 × ΔHCO3- |
| Acute respiratory acidosis | ΔHCO3- = +1 per 10 mmHg ↑PCO2 |
| Chronic respiratory acidosis | ΔHCO3- = +4 per 10 mmHg ↑PCO2 |
| Acute respiratory alkalosis | ΔHCO3- = -2 per 10 mmHg ↓PCO2 |
| Chronic respiratory alkalosis | ΔHCO3- = -5 per 10 mmHg ↓PCO2 |
If compensation is more or less than predicted, a mixed disorder is present.
(Roberts and Hedges' Clinical Procedures in Emergency Medicine)
Step 4 - Calculate the Anion Gap (AG)
AG = Na+ - (Cl- + HCO3-) Normal = 8-12 mEq/L (with albumin-corrected normal ~12)
If pH is low and the primary process is metabolic, the AG tells you the cause:
- Elevated AG (>12): An unmeasured anion is consuming HCO3- → think MUDPILES/GOLDMARK
- Normal AG (hyperchloremic): HCO3- loss with Cl- retention
Step 5 - If AG is elevated, calculate Delta-Delta (ΔΔ)
ΔAG = measured AG - 12 Add ΔAG to the measured HCO3-
- Sum = 22-26 → pure AG metabolic acidosis
- Sum > 26 → concurrent metabolic alkalosis
- Sum < 22 → concurrent non-AG (hyperchloremic) metabolic acidosis
6. The Acid-Base Map
These two diagrams (from Murray & Nadel's and Roberts & Hedges') are standard references for plotting where a patient falls:
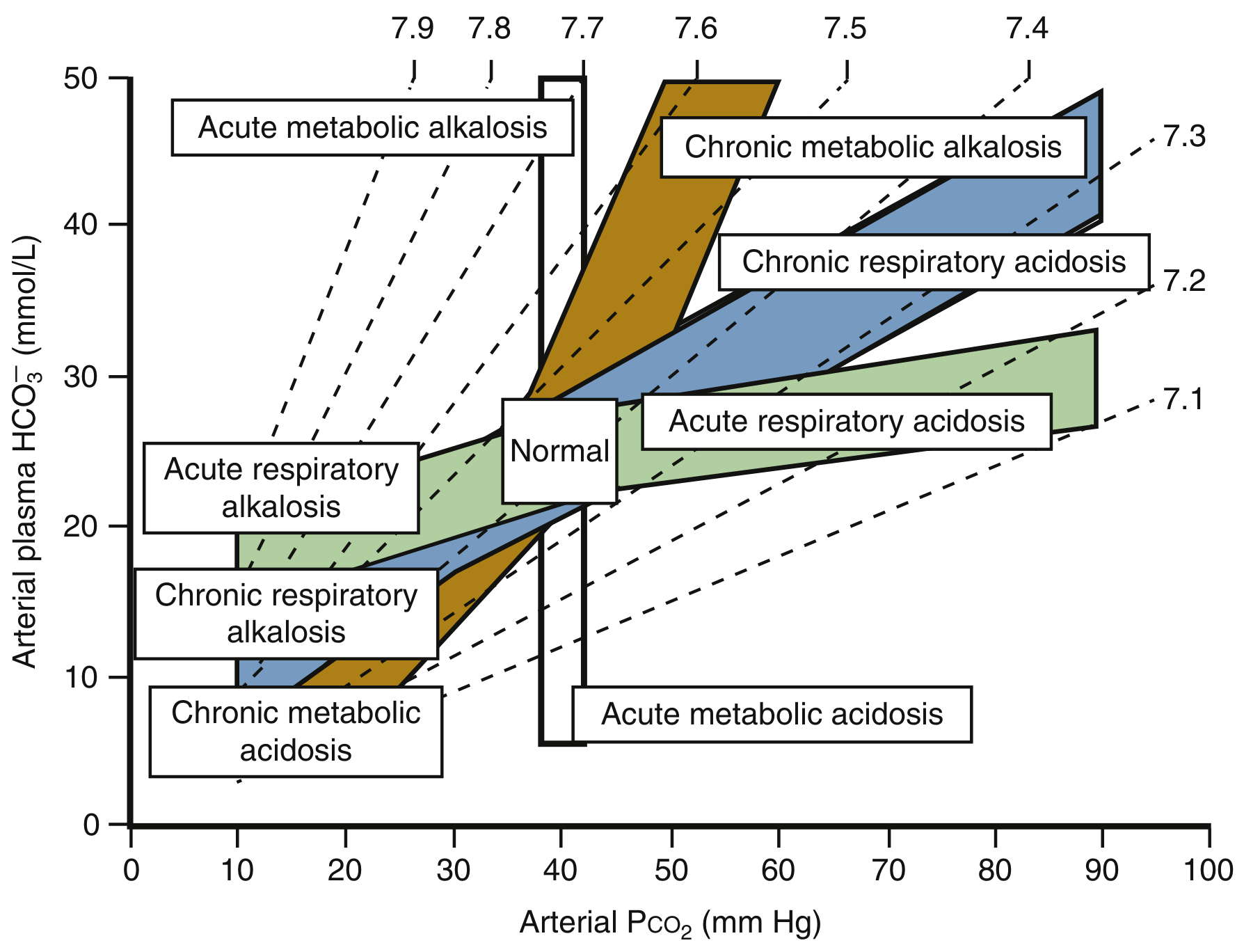
Arterial plasma HCO3- vs. PCO2 - each colored band represents the expected compensation zone for a simple (single) disorder. A point falling outside a band suggests a mixed disorder.
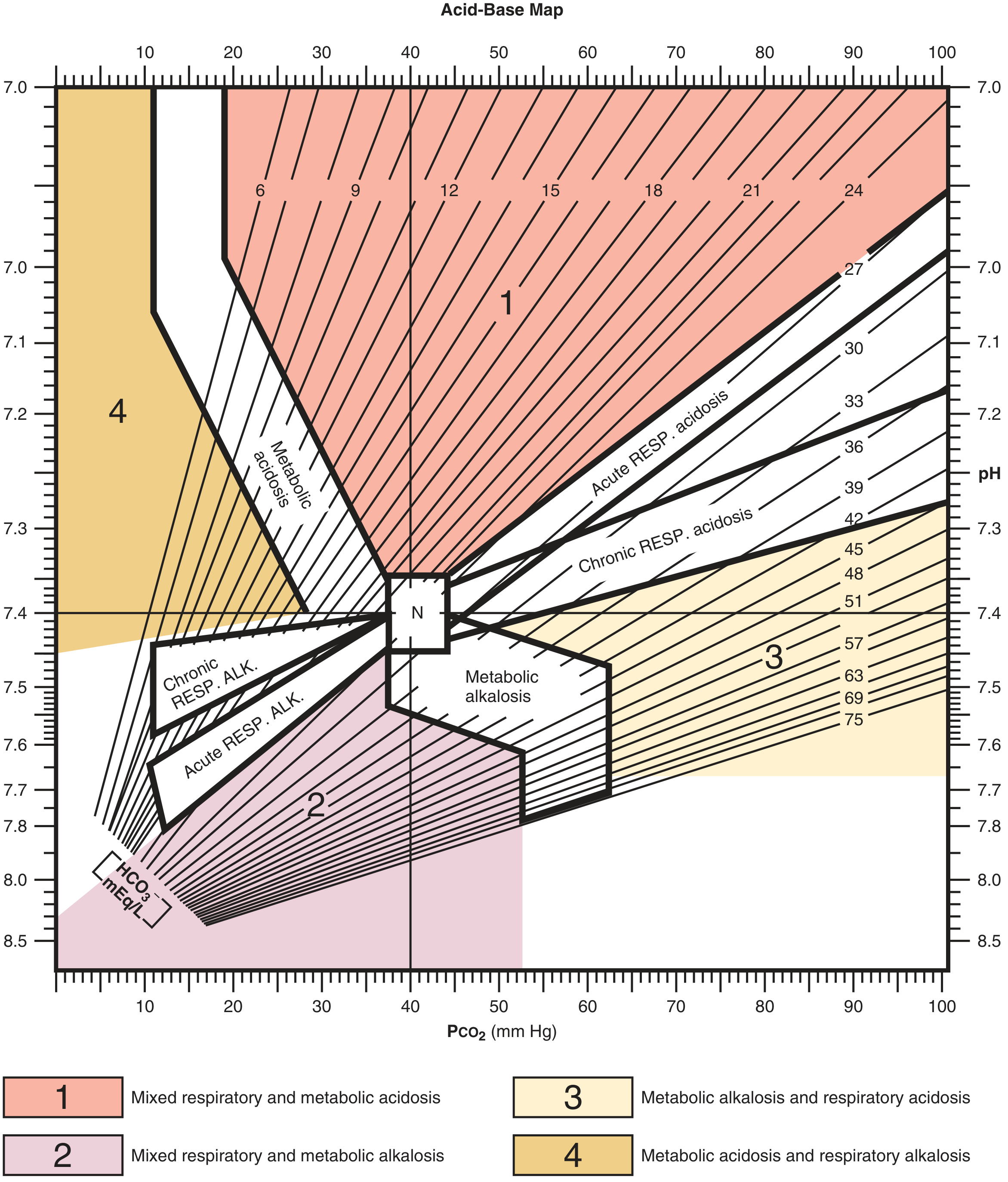
Zone 1 = mixed respiratory + metabolic acidosis; Zone 2 = mixed respiratory + metabolic alkalosis; Zone 3 = metabolic alkalosis + respiratory acidosis; Zone 4 = metabolic acidosis + respiratory alkalosis. "N" marks the normal point.
7. The Four Primary Disorders - In Detail
A. Metabolic Acidosis
Definition: Primary decrease in HCO3-, pH < 7.35
Compensation: Lungs hyperventilate - rapid (hours), Winter's formula: expected PCO2 = 1.5 × HCO3- + 8 ± 2, or ΔPCO2 = 1.3 × ΔHCO3-
Elevated AG Causes - "MUDPILES" or "GOLDMARK"
| Mnemonic | Cause |
|---|---|
| M ethanol | Formate accumulation |
| U remia | Uremic acids |
| D KA / starvation / alcoholic ketoacidosis | Ketone bodies |
| P ropylene glycol | Lactic acid + osmol gap |
| I soniazid / Iron | Lactic acidosis |
| L actic acidosis | Type A (hypoperfusion), Type B (drugs/mitochondrial) |
| E thylene glycol | Oxalate accumulation |
| S alicylates | Also causes concurrent respiratory alkalosis |
In DKA: lactic acid dissociates → H+ consumes HCO3-, lactate (conjugate base) accumulates → AG rises while Cl- is unchanged. β-hydroxybutyrate:acetoacetate ratio rises from 2:1 to >8:1 in severe cases. Note: the urine nitroprusside test only detects acetoacetate, not β-hydroxybutyrate, so apparent worsening on nitroprusside may actually be improvement.
Normal AG (Hyperchloremic) Causes
- Renal: RTA types 1, 2, 4; chronic kidney disease
- GI: Diarrhea (HCO3- loss), pancreatic fistula, ureterosigmoidostomy
- Iatrogenic: Excess IV normal saline, NH4Cl, hyperalimentation
Type 4 RTA - the most common RTA in adults: hypoaldosteronism (usually diabetic nephropathy with hyporeninemia) → hyperkalemia + mild acidosis. ACEi, ARBs, heparin, and K-sparing diuretics can precipitate it.
Clinical effects: Hyperventilation (Kussmaul breathing in severe cases), cardiac depression (at pH < 7.1), decreased response to catecholamines, hyperkalemia (H+/K+ exchange across cell membranes), bone resorption (chronic).
B. Metabolic Alkalosis
Definition: Primary increase in HCO3-, pH > 7.45
Compensation: Hypoventilation - PCO2 increases 0.6 mmHg per 1 mEq/L rise in HCO3-. This is limited by hypoxemic drive.
Key concept: Metabolic alkalosis has a generation phase (something causes HCO3- to rise) and a maintenance phase (usually the kidney's need to retain Na/volume overrides HCO3- excretion).
| Category | Urine Cl- | Cause |
|---|---|---|
| Chloride-responsive | < 20 mEq/L | Vomiting, NG suction, diuretics (past), post-hypercapnic alkalosis |
| Chloride-resistant | > 20 mEq/L | Hyperaldosteronism, Cushing's, Bartter/Gitelman syndrome, severe hypokalemia |
Clinical effects: Usually asymptomatic until pH > 7.5 or HCO3- > 45. Alkalosis shifts hemoglobin-O2 curve left (higher O2 affinity, less O2 release to tissues), decreased ventilation, peripheral vasoconstriction, neuromuscular irritability/tetany (Chvostek, Trousseau signs), ventricular arrhythmias.
Treatment:
- Chloride-responsive: replete volume + NaCl/KCl
- Chloride-resistant: treat underlying cause; spironolactone if hyperaldosteronism; acetazolamide for post-hypercapnic alkalosis; rarely HCl infusion (100-200 mEq/L via central line) for severe cases
C. Respiratory Acidosis
Definition: Primary increase in PCO2 (hypoventilation), pH < 7.35
Acute vs. Chronic:
- Acute: Non-HCO3- buffers absorb H+ → HCO3- rises by ~1 mEq/L per 10 mmHg ↑PCO2 (pH falls sharply)
- Chronic: Kidneys retain HCO3-, excrete H+ → HCO3- rises by ~4 mEq/L per 10 mmHg ↑PCO2 (pH near normal)
Causes:
- CNS depression: opioids, sedatives, stroke, obesity hypoventilation
- Neuromuscular: Guillain-Barré, myasthenia gravis, ALS, diaphragm paralysis
- Airway/lung: severe COPD, status asthmaticus, pneumothorax, massive pneumonia
Important: In COPD with chronic hypercapnia, central chemoreceptors adapt. High-flow O2 can suppress hypoxic (peripheral carotid body) drive → progressive CO2 retention and narcosis.
Clinical effects: Headache, papilledema, confusion, asterixis, CO2 narcosis at extreme levels. Sympathetic activation initially raises BP/HR.
D. Respiratory Alkalosis
Definition: Primary decrease in PCO2 (hyperventilation), pH > 7.45
Compensation:
- Acute: HCO3- falls 2 mEq/L per 10 mmHg ↓PCO2
- Chronic: HCO3- falls 5 mEq/L per 10 mmHg ↓PCO2
Causes (common):
- Hypoxemia (PE, high altitude, severe anemia) - hypoxic drive via carotid bodies
- Sepsis/SIRS - early, before lactic acidosis develops
- Salicylate toxicity - directly stimulates respiratory center (also causes metabolic acidosis → mixed picture)
- Anxiety/hyperventilation
- Liver failure (progesterone/ammonia stimulate respiration)
- Mechanical ventilation (over-ventilation)
- CNS: pain, pregnancy, intracranial hypertension
Clinical effects: Perioral numbness, paresthesias, light-headedness, carpopedal spasm. Cerebral vasoconstriction from hypocapnia can cause syncope.
8. Special Concepts
Base Excess (BE)
An alternative metabolic parameter. Defined as the amount of strong acid or alkali needed to titrate fully oxygenated blood to pH 7.4 at 37°C and PCO2 = 40 mmHg. Normal = -2 to +2 mEq/L.
- Negative BE (base deficit) = metabolic acidosis (common in trauma/shock resuscitation)
- Positive BE = metabolic alkalosis HCO3- is simpler to use clinically but BE is less affected by acute PCO2 changes.
Albumin Correction of AG
At normal albumin (4 g/dL), AG normal = 12. For every 1 g/dL fall in albumin below 4:
Corrected AG = measured AG + 2.5 × (4 - albumin)
This is critical in hypoalbuminemic patients (cirrhosis, nephrotic syndrome, malnutrition) - a hidden AG acidosis can be masked by the low albumin.
Osmolal Gap
Osmolal gap = measured serum osmolality - calculated osmolality Calculated = 2[Na+] + [glucose]/18 + [BUN]/2.8
Normal < 10 mOsm/kg. Elevated gap (>10-20) in the presence of AG acidosis suggests toxic alcohol ingestion (methanol, ethylene glycol, propylene glycol, isopropanol).
9. Worked Clinical Examples
Case 1 - DKA
ABG: pH 7.26, PCO2 13, HCO3- 5, Na+ 133, K+ 2.8, Cl- 118
- pH 7.26 → acidemia
- HCO3- 5 (low), PCO2 low (not elevated) → metabolic acidosis
- AG = 133 - (118 + 5) = 10 - wait, that is normal. Re-check: actually AG = Na - (Cl + HCO3) = 133 - 123 = 10. But consider albumin correction and clinical context (DKA + vomiting can mix disorders).
- Compensation (Winter's): expected PCO2 = 1.5 × 5 + 8 = 15.5 ± 2 → actual PCO2 13 is within range → simple metabolic acidosis with appropriate respiratory compensation.
Case 2 - Sepsis
ABG: pH 7.49, PCO2 25, HCO3- 22, Na+ 138, K+ 3.2, Cl- 105
- pH 7.49 → alkalemia
- PCO2 25 (low), HCO3- not elevated → respiratory alkalosis
- Expected decrease in HCO3- = 2 per 10 mmHg drop = 2 × 1.5 = 3 mEq/L drop → expected HCO3- = 24 - 3 = 21. Actual 22 ≈ predicted → simple acute respiratory alkalosis
- Clinical: E. coli bacteremia driving respiratory center → sepsis-induced hyperventilation
(Roberts and Hedges' Clinical Procedures in Emergency Medicine, case examples)
Case 3 - Mixed Disorder (COPD + Vomiting)
ABG: pH 7.44, PCO2 60, HCO3- 40
- pH 7.44 → near normal
- PCO2 60 → chronic respiratory acidosis
- Expected HCO3- compensation = 24 + 4 × (60-40)/10 = 24 + 8 = 32 mEq/L. Actual = 40 → higher than expected → concurrent metabolic alkalosis (e.g., vomiting, diuretics)
10. Oxygenation Assessment
ABG also evaluates oxygenation (separate from acid-base):
A-a Gradient (alveolar-arterial O2 difference):
PAO2 = FiO2 × (713) - PaCO2/0.8 (at sea level, normal breathing room air: FiO2 = 0.21) A-a gradient = PAO2 - PaO2
Normal A-a gradient = Age/4 + 4 (age-adjusted), roughly 5-15 mmHg on room air.
| Condition | PaO2 | A-a gradient |
|---|---|---|
| Hypoventilation alone | Low | Normal |
| V/Q mismatch (PE, pneumonia, COPD) | Low | Elevated |
| Diffusion defect (fibrosis) | Low | Elevated |
| Shunt (ARDS, intracardiac) | Low | Elevated, does not correct with O2 |
P/F ratio (PaO2/FiO2):
- Normal > 400
- Mild ARDS: 201-300
- Moderate ARDS: 101-200
- Severe ARDS: ≤ 100
Quick Reference Card
NORMAL VALUES
pH: 7.35-7.45
PCO2: 35-45 mmHg
HCO3-: 22-26 mEq/L
PaO2: 80-100 mmHg
BE: -2 to +2
STEP-BY-STEP
1. pH → acidemia or alkalemia?
2. Match: PCO2 ↑ + pH ↓ = resp. acidosis
PCO2 ↓ + pH ↑ = resp. alkalosis
HCO3- ↓ + pH ↓ = met. acidosis
HCO3- ↑ + pH ↑ = met. alkalosis
3. Check compensation formula
4. Calculate AG = Na - (Cl + HCO3)
5. If AG elevated → Delta-Delta ratio
COMPENSATION FORMULAS
Met. acidosis: ΔPCO2 = 1.3 × ΔHCO3-
Met. alkalosis: ΔPCO2 = 0.6 × ΔHCO3-
Resp. acid (ac): ΔHCO3 = +1 per 10mmHg ↑PCO2
Resp. acid (ch): ΔHCO3 = +4 per 10mmHg ↑PCO2
Resp. alk (ac): ΔHCO3 = -2 per 10mmHg ↓PCO2
Resp. alk (ch): ΔHCO3 = -5 per 10mmHg ↓PCO2
AG ACIDOSIS CAUSES: MUDPILES
Methanol / Metformin (lactic)
Uremia
DKA / alcoholic / starvation ketoacidosis
Propylene glycol / Paraldehyde
Isoniazid / Iron (lactic)
Lactic acidosis (type A, type B)
Ethylene glycol
Salicylates
Sources: Murray & Nadel's Textbook of Respiratory Medicine | Roberts and Hedges' Clinical Procedures in Emergency Medicine | Frameworks for Internal Medicine | Schwartz's Principles of Surgery | Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.