Saddle nose Deformity - essay answer PG exam with diagrams under 800 words
Reading File
Finding Sources
Finding Sources
Searching Images
saddle nose deformity causes classification
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Saddle nose Deformity - essay answer PG exam with diagrams under 800 words
Reading File
Finding Sources
Finding Sources
Searching Images
saddle nose deformity nasal bridge collapse clinical photo
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
I now have all the material needed. Here is the complete PG exam essay:
Saddle Nose Deformity
Definition
Saddle nose deformity is a concave depression of the nasal dorsum resulting from loss of structural support of the nasal framework — bony, cartilaginous, or both — with subsequent collapse. The profile resembles the shape of a horse saddle, with depression of the mid-dorsum and a relatively prominent tip and radix.
Anatomy of the Nasal Framework
The nasal dorsum is supported by three components in continuity:
- Bony vault — nasal bones
- Middle vault — upper lateral cartilages (ULC) + dorsal septum (L-strut)
- Lower vault — lower lateral cartilages (LLC) + columellar strut
The L-strut (dorsal + caudal limb of the septum) is the critical central support. Its destruction is the common pathway in most saddle deformities.
Normal nasal profile (lateral):
___
/ \ ← Bony dorsum
/ \___ ← Cartilaginous dorsum
| __/ ← Tip
\____/
Saddle deformity:
___
/ \
/ ↓ \ ← Dorsal collapse (concavity)
| _ __/ ← Prominent tip
\_____/
Aetiology
Mnemonic:ISTIC
| Category | Examples |
|---|---|
| Iatrogenic | Over-resection of septal cartilage, rhinoplasty over-reduction |
| Septal haematoma | Untreated → avascular necrosis of septal cartilage |
| Trauma | Nasal fracture with disruption of L-strut |
| Infective / Inflammatory | Syphilis (tertiary — gumma), leprosy, TB, cocaine-induced midline destructive lesion (CIMDL), GPA (Wegener's), Relapsing polychondritis |
| Congenital | Congenital syphilis, chondrodysplasias |
| Cartilage destruction | Malignancy, septal abscess |
Key exam point: Septal haematoma is the most preventable cause — urgent drainage prevents cartilage ischemia and subsequent saddle deformity.
Clinical Features
Fig 1. Saddle nose deformity (lateral view) — note the concave dorsal profile with relative prominence of the nasal tip

Fig 2. Lateral profile demonstrating dorsal depression in post-rhinoplasty saddle deformity
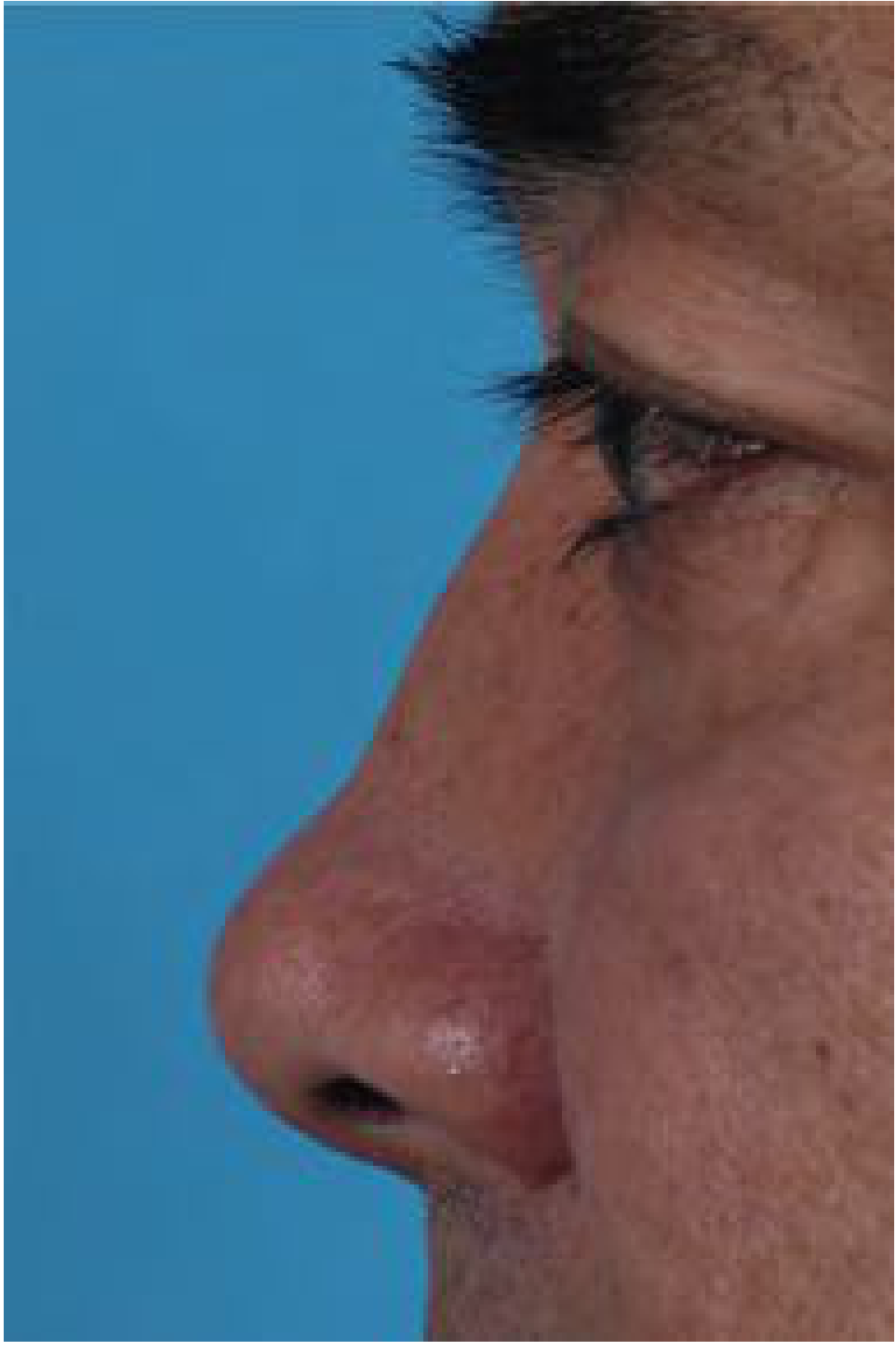
Symptoms:
- Cosmetic: dorsal concavity, tip over-rotation, columellar retraction, widened dorsum on frontal view
- Functional: nasal obstruction (due to internal nasal valve collapse), septal perforation
Classification (Becker/Romo)
| Grade | Involvement |
|---|---|
| Type I | Supratip soft tissue loss only |
| Type II | Cartilaginous vault collapse |
| Type III | Bony and cartilaginous vault collapse |
| Type IV | Combined with external skin deficit |
Assessment
- Full rhinological history (trauma, cocaine use, prior surgery)
- Workup for systemic disease: ANCA (GPA), VDRL/TPHA (syphilis), skin biopsy (leprosy)
- Nasal endoscopy — septal perforation, mucosal disease
- CT scan — extent of bony vs cartilaginous loss
- Standardised photography (lateral, base, frontal views)
Surgical Management
Principle: Re-establish the septal L-strut to restore dorsal height and structural integrity.
Step-wise approach:
1. Graft Material Selection (Preferred: Autologous)
- Septal cartilage — first choice (limited if septum already destroyed)
- Auricular cartilage — small defects
- Costal (rib) cartilage — preferred for large defects requiring structural support
- Calvarial bone / iliac crest — bony vault reconstruction
- Alloplasts (Gore-Tex, Silastic) — if autologous unavailable; higher extrusion risk
2. Surgical Techniques
- Extended spreader grafts — widen and elevate the middle vault, reconstruct the dorsal septum
- Caudal septal replacement graft — re-creates the caudal L-strut
- Canoe-shaped dorsal onlay graft — placed in a subperiosteal pocket; cephalic margin at nasal starting point, caudal margin at supratip; lateral edges beveled to minimize visibility
- Osteotomies — to close open roof if dorsal reduction precedes augmentation
- Temporalis fascia overlay — camouflages contour irregularities in thin-skinned patients
Fig 3. Intraoperative view: extended costal cartilage spreader grafts + caudal septal replacement graft reconstructing the L-strut

Staging: In severe cases with extensive septal surgery + osteotomies, a two-stage approach is preferred — structural reconstruction first, augmentation implant at second sitting.
Prevention
- Drain septal haematoma within 24–48 hours
- During rhinoplasty: preserve minimum 1 cm L-strut (dorsal + caudal limbs)
- Avoid over-resection of cartilaginous dorsum (>3 mm reduction compromises the middle vault)
Summary Box
| Aspect | Key Point |
|---|---|
| Definition | Dorsal concavity from loss of nasal framework support |
| Commonest preventable cause | Untreated septal haematoma |
| Systemic causes | GPA, syphilis, cocaine, relapsing polychondritis |
| Preferred graft | Autologous cartilage (rib for large defects) |
| Core surgical principle | Reconstruct L-strut; extended spreader + caudal replacement grafts |
Sources: Cummings Otolaryngology Head and Neck Surgery; Harrison's Principles of Internal Medicine 22e; KJ Lee's Essential Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.