
Treatment with explanations and teach me this topic please
bilateral hemisacralization L5 spondylosis treatment management
https://www.healthline.com/health/sacralization
X-Ray Report Analysis & Complete Teaching Guide
Patient Summary
Understanding the Spine (Foundation)
Breaking Down Each Finding
1. Lumbar Curvature is Almost Straightened
2. Mild Osteophytes at L4-L5
- Mild osteophytes at L4-L5 indicate early-to-moderate degenerative disc disease at that level
- They can eventually compress nerve roots exiting between L4 and L5, causing pain radiating into the legs (radiculopathy)
- The L4-L5 level is one of the most commonly affected in lumbar degeneration because it bears the greatest rotational and bending forces
3. Partial Sacralization of L5 (Bilateral) = Hemisacralization
What is Sacralization?
- Complete sacralization - L5 is fully fused bilaterally - the patient functionally has only 4 mobile lumbar vertebrae
- Hemisacralization - the fusion is partial (pseudo-articulation, not complete bony union), and in this case it is bilateral (both sides)
- This falls under Castellvi Classification Type II-b: bilateral enlarged transverse processes forming a pseudo-joint with the sacral ala
The Biomechanical Problem
- The L5-S1 motion segment loses mobility
- Mechanical stress is redistributed UPWARD to L4-L5, which now bears more movement and load than normal
- This explains why this patient has osteophytes at L4-L5 (adjacent segment disease)
- The reduced disc space at L5-S1 (see finding #5) is also directly related
4. Spina Bifida Occulta at L5
5. Reduced Disc Space at L5-S1
- Loss of disc height causes the facet joints above to override each other (facet arthropathy)
- Nerve roots (L5, S1) can become compressed in the narrowed foramina
- Pain from the disc itself (discogenic pain) - deep, aching, worsened by sitting and bending forward
6. SI Joints are Normal
The Big Picture: How Everything Connects
Congenital anomaly: Bilateral hemisacralization of L5
|
v
L5-S1 hypomobility + abnormal stress distribution
|
|--- Direct effect at L5-S1: Reduced disc space (disc degeneration)
|
|--- Compensatory overload at L4-L5: Osteophyte formation (spondylosis)
|
|--- Muscle spasm response: Straightening of lumbar lordosis
|
+--- Co-existing: Spina bifida occulta L5 (congenital, incidental)
Treatment
Step 1: Conservative (First-line - most patients respond)
| Approach | Details |
|---|---|
| Rest modification | Avoid prolonged sitting, heavy lifting, repetitive bending. Short rest during flares only (prolonged bed rest is harmful). |
| NSAIDs | Ibuprofen 400-600 mg TID or Diclofenac 50 mg BD with meals - reduce inflammation and pain at osteophytes and disc. Take for 2-4 weeks during flares. |
| Muscle relaxants | Cyclobenzaprine or Methocarbamol for the muscle spasm causing loss of lordosis. Short-term use only (2 weeks max). |
| Analgesics | Paracetamol 500-1000 mg TID as background pain control. |
| Topical agents | Diclofenac gel or counterirritation creams (capsaicin) over the lower back. |
Step 2: Physical Therapy (Very important - long-term benefit)
- Core strengthening exercises (McKenzie method, lumbar stabilization) - strengthen the deep stabilizers (multifidus, transversus abdominis) to compensate for the hypermobile segments
- Stretching - hip flexors, hamstrings, piriformis - all are tight in patients with lumbar pathology
- Posture correction - restoring lumbar lordosis, ergonomic training
- Heat therapy before exercise to relax muscles; cold packs during acute flares
- TENS (transcutaneous electrical nerve stimulation) - useful for chronic pain
Step 3: Interventional (If conservative fails after 6-12 weeks)
- Fluoroscopy-guided injection at the pseudoarticulation (the L5-sacrum false joint) - local anesthetic + corticosteroid injected directly into the abnormal joint formed by the sacralized transverse process. This is both diagnostic AND therapeutic.
- Sacroiliac joint injection - if SI joint is involved
- Epidural steroid injection (ESI) - if there is nerve root compression causing leg pain/sciatica
- Radiofrequency ablation - for chronic facet or pseudoarticulation pain not responding to injections
- Electric denervation of L5-S1 space - a minimally invasive option reported in the literature
Step 4: Surgical (Rarely needed - only ~43 cases reported in literature)
- Failed conservative therapy for >6-12 months
- Progressive neurological deficit (weakness, bladder/bowel dysfunction)
- Significant nerve root compression confirmed on MRI
- Resection of the enlarged transverse process (release the pseudo-joint) - for unilateral Bertolotti's causing asymmetric pain
- Discectomy + fusion at L5-S1 if disc herniation/instability is the dominant problem
Summary for This Patient (Amena Begum, 40F)
- Bilateral hemisacralization - born with partial fusion of L5 to sacrum on both sides (congenital, not her fault)
- This has caused mechanical overload at adjacent levels over 40 years
- Osteophytes at L4-L5 + reduced L5-S1 disc space = spondylosis (degenerative wear)
- Spina bifida occulta L5 - incidental, asymptomatic congenital variant at the same vertebra
- Muscle spasm causing loss of lumbar lordosis
Can u repeat 🙏
X-Ray Report: Complete Teaching Guide
The Patient
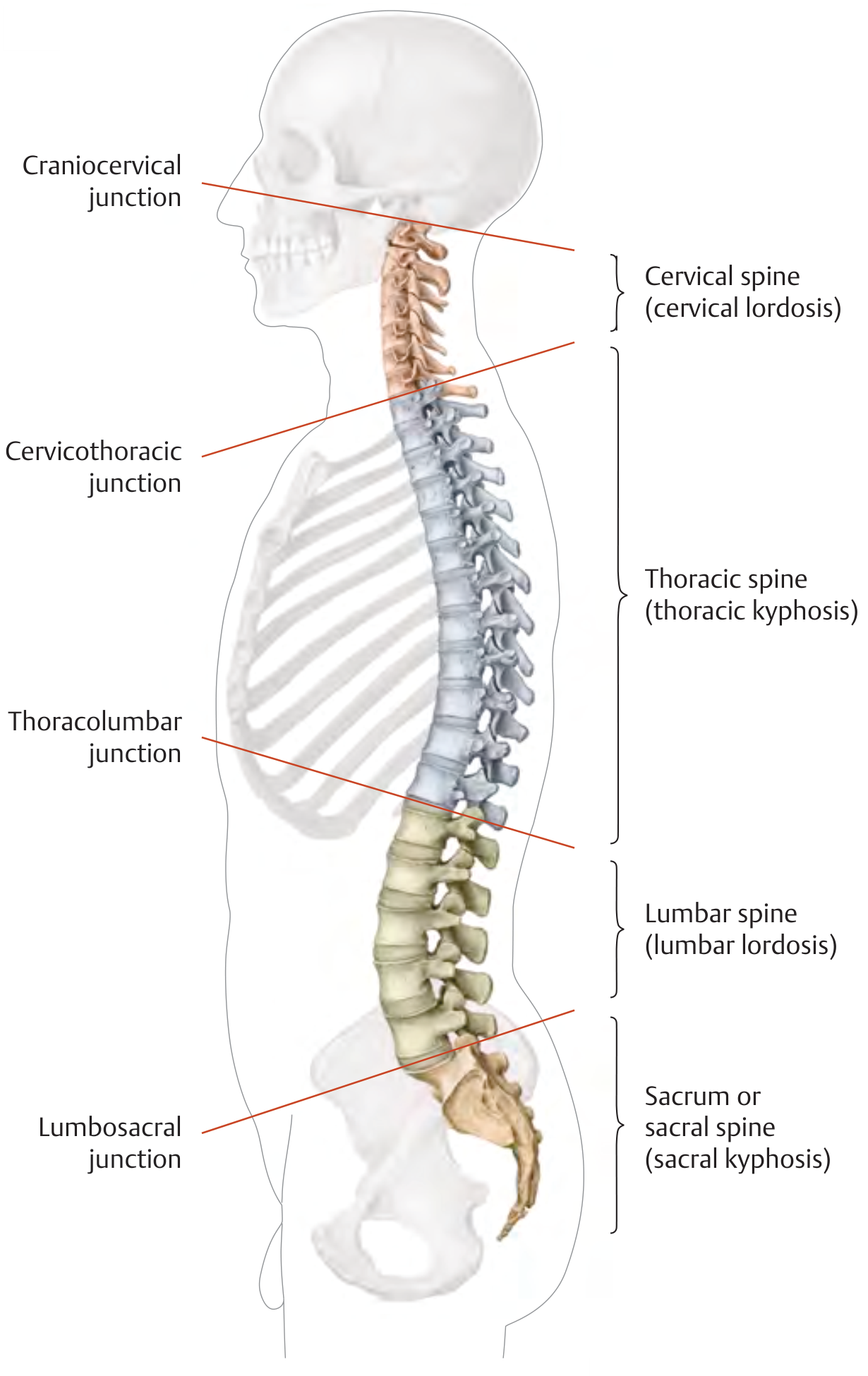
First - Understand the Normal Spine
- Cervical (neck) - 7 vertebrae
- Thoracic (chest) - 12 vertebrae
- Lumbar (lower back) - 5 vertebrae (L1-L5)
- Sacrum (fused bone at base) + Coccyx
Now Let's Go Through Each Finding One by One
Finding 1: Lumbar Curvature Almost Straightened
What is normal?
What happened here?
Why does this happen?
What it tells us clinically:
Finding 2: Mild Osteophytes at L4-L5
What are osteophytes?
Why do they form?
- The disc loses height and becomes less able to absorb force
- The vertebral body edges experience abnormal stress
- The body responds by laying down extra bone at the edges - like reinforcing a weak joint
- These extra bits of bone = osteophytes
Why at L4-L5 specifically?
Danger of osteophytes:
- Pain radiating down the leg
- Numbness/tingling in the leg
- In severe cases, weakness
Finding 3: Partial Sacralization of L5 - Both Sides (= Bilateral Hemisacralization)
This is the MOST IMPORTANT finding. Let's teach it properly.
Step A: What is the normal L5?
Step B: What is Sacralization?
| Type | Meaning |
|---|---|
| Complete sacralization | L5 fully fused to sacrum on both sides - patient effectively has only 4 mobile lumbar vertebrae |
| Partial / Hemisacralization | Incomplete fusion - a false joint (pseudoarticulation) forms instead of complete bony union |
| Unilateral | Only one side affected |
| Bilateral | Both sides affected - as in this patient |
Step C: What is the biomechanical consequence?
Normal: L4-L5 moves normally
L5-S1 moves normally
Stress shared equally
With sacralization:
L5-S1 is STIFF / hypomobile (partially fused)
All excess movement shifts UP to L4-L5
L4-L5 becomes HYPERMOBILE
→ L4-L5 disc degenerates faster
→ Osteophytes form at L4-L5
→ L5-S1 disc degenerates under compression
Step D: What is Bertolotti's Syndrome?
Finding 4: Spina Bifida Occulta at L5
What is it?
- "Occulta" = hidden
- The skin over it is completely normal
- The spinal cord and nerves are NOT herniated - they are safe inside
- There is just a small gap/defect in the back of the vertebra that you can see on X-ray
Is it dangerous?
When to be concerned:
- Tuft of hair
- Dimple or pit
- Hemangioma (birthmark)
- Lipoma (fatty lump)
Why does it occur at L5 here?
Finding 5: Reduced Disc Space at L5-S1
What is a normal disc space?
What happened here?
Why?
- Nucleus pulposus - the soft, jelly-like center (mostly water)
- Annulus fibrosus - the tough outer ring
Consequences of reduced disc space:
- Less shock absorption at L5-S1
- Vertebral bodies get closer together - osteophytes form at the edges
- The foramen (hole where nerve exits) becomes narrower - nerve root compression risk
- Facet joints (small joints at the back of vertebrae) override each other - painful arthropathy
Finding 6: SI Joints Normal
- Ankylosing spondylitis (inflammatory arthritis that fuses SI joints)
- Sacroiliitis from other inflammatory arthropathies (psoriatic arthritis, reactive arthritis, IBD-related)
How All Findings Connect Together
CONGENITAL (born with it):
Bilateral Hemisacralization of L5
+ Spina Bifida Occulta of L5
|
|
v
BIOMECHANICAL CONSEQUENCE (develops over years):
L5-S1 hypomobility
|
|-----> L5-S1 disc under compression --> REDUCED L5-S1 DISC SPACE
|
|-----> Excess load shifts to L4-L5 --> OSTEOPHYTES at L4-L5 (Spondylosis)
|
v
CLINICAL RESPONSE:
Pain --> Muscle spasm --> STRAIGHTENING OF LUMBAR LORDOSIS
SI joints = Normal (no inflammatory disease)
TREATMENT
Goals:
- Relieve pain and muscle spasm
- Restore function and movement
- Prevent progression
- Address nerve compression if present
Stage 1: Medications (Acute phase)
| Drug | Dose | Purpose |
|---|---|---|
| Diclofenac (NSAID) | 50 mg twice daily with food | Reduce inflammation and pain at osteophytes/disc |
| Ibuprofen (NSAID) | 400-600 mg three times daily | Alternative NSAID |
| Paracetamol | 500-1000 mg three times daily | Background pain control |
| Muscle relaxant (e.g., Methocarbamol, Tizanidine) | As prescribed | Relieve paravertebral muscle spasm - helps restore lordosis |
| Pantoprazole/Omeprazole | 20-40 mg daily | Protect stomach while taking NSAIDs |
| Vitamin D + Calcium | Supplement | Support bone health (important in women aged 40+) |
Stage 2: Physical Therapy (Most important for long-term)
- Targets the multifidus and transversus abdominis - the deep stabilizing muscles of the lumbar spine
- Compensates for the stiffened L5-S1 segment
- Reduces load on osteophyte-forming L4-L5
- McKenzie extension exercises
- Pelvic tilts
- Dead bugs
- Bird-dog exercises
- Gentle swimming or walking
- Hip flexor stretches
- Hamstring stretches
- Piriformis stretches (All these muscle groups are typically tight in lower back pain)
- Correct sitting posture - use lumbar support
- Ergonomic advice for daily activities
- Avoid prolonged sitting (especially important since she is 40F and likely has a desk job or household duties with repetitive bending)
- Heat (hot water bottle/pad) before exercise - relaxes muscles
- Cold pack during acute painful flares - reduces inflammation
Stage 3: Interventional (If conservative fails after 6-8 weeks)
| Procedure | Target | How it works |
|---|---|---|
| Fluoroscopy-guided pseudoarticulation injection | The false joint formed by sacralized L5 transverse process | Steroid + local anesthetic injected directly into the abnormal joint - most specific treatment for this condition |
| Epidural steroid injection (ESI) | Nerve root compression at L4-L5 or L5-S1 | Steroid bathes inflamed nerve roots, reduces swelling and pain |
| Facet joint injection | Facet arthropathy | Direct injection into degenerated facet joints |
| Radiofrequency ablation | Chronic facet/pseudoarticulation pain | Heat destroys the small pain-carrying nerves - gives long-lasting relief |
Stage 4: Surgery (Rarely needed)
- Complete failure of all conservative + interventional treatment (6-12+ months)
- Progressive neurological signs: weakness in legs, foot drop, loss of bladder/bowel control
- Severe nerve compression confirmed on MRI
- Resection of enlarged transverse process - releases the abnormal pseudoarticulation
- Discectomy - removes herniated disc material pressing on nerves
- Spinal fusion at L4-L5 or L5-S1 - last resort for instability
What to Do Next for This Patient
-
Get MRI lumbar spine - X-ray shows bones; MRI shows the disc, nerves, and soft tissues much better. This will determine if there is nerve compression, disc herniation, or canal stenosis that X-ray cannot show.
-
Start NSAIDs + muscle relaxant for the acute pain and spasm
-
Refer to physiotherapy - core strengthening program
-
Lifestyle modifications:
- Weight management (excess weight increases lumbar load)
- Avoid high heels
- Use a firm mattress
- Use a lumbar roll when sitting
- Avoid prolonged bending/lifting
-
Follow-up in 6-8 weeks to assess response and decide if injections are needed
Quick Revision Summary Table
| Finding | Type | Cause | Treatment |
|---|---|---|---|
| Straightened lordosis | Secondary | Muscle spasm from pain | Muscle relaxants + physiotherapy |
| Osteophytes L4-L5 | Degenerative | Adjacent segment overload from sacralization | NSAIDs + physiotherapy + injection if needed |
| Bilateral hemisacralization L5 | Congenital | Embryological anomaly | Cannot be corrected; treat symptoms |
| Spina bifida occulta L5 | Congenital | Posterior arch closure failure | Usually no treatment needed |
| Reduced disc space L5-S1 | Degenerative | Disc degeneration from sacralization-related stress | Conservative + ESI if nerve involved |
| Normal SI joints | Normal | Confirms NO inflammatory arthritis | Reassurance |

Are these medicines necessary. Breakdown with cause please
Tab Bonigen calcium vitamin D Tab Arth A TS glucosamine chondroitin Tab Flexibac baclofen muscle relaxant uses
Tab Xalcort methylprednisolone 6mg short course back pain Tab Neuro B thiamine B6 B12 neuropathy
Prescription Analysis - Complete Breakdown
The Prescription (from the image):
- Tab Bonigen 1+0+1 for 15 days → then Tab Arth A TS 1+0+0 for 30 days
- Tab Nabumet 500 mg 1+0+1 for 15 days
- Tab Flexibac 5 mg 1+0+1 for 7 days
- Tab Neuro B 1+0+1 for 30 days
- Tab Xalcort 6 mg 2+0+0 for 5 days
- Cap Exium 20 mg 1+0+1 for 10 days
YES - All 6 medicines are necessary. Here is exactly why:
1. Tab Bonigen → then Tab Arth A TS
What are they?
- Bonigen = Calcium + Vitamin D3 supplement
- Arth A TS = Glucosamine + Chondroitin Sulfate (joint cartilage supplement)
Why prescribed?
- Bone density continues to fall
- Osteophytes worsen
- Disc degeneration accelerates
- Risk of osteoporosis increases
- They help slow cartilage breakdown at L4-L5 and L5-S1
- May reduce joint pain and stiffness from spondylosis
- Support the disc's ability to hold water and maintain height
2. Tab Nabumet 500 mg (1+0+1 for 15 days)
What is it?
Why prescribed?
- Osteophytes at L4-L5 - bone spurs cause local inflammation
- Reduced disc space at L5-S1 - degenerating disc releases inflammatory chemicals
- Muscle spasm straightening her lumbar curve - inflammation drives this spasm
3. Tab Flexibac 5 mg (1+0+1 for 7 days only)
What is it?
Why prescribed?
- Causes significant pain on its own
- Prevents normal movement and posture
- Reduces blood flow to the area, worsening healing
- Keeps the lumbar curve straightened
4. Tab Neuro B (1+0+1 for 30 days)
What is it?
Why prescribed?
- Osteophytes at L4-L5 can compress nerve roots
- Reduced disc space at L5-S1 can compress the L5 and S1 nerve roots
- The straightened lumbar curve puts traction on nerve roots
- They become demyelinated (lose their protective coating)
- Nerve signal transmission slows or fails
- The patient experiences tingling, numbness, burning pain in the legs (radiculopathy)
- B1 (Thiamine): Supports energy production in nerve cells
- B6 (Pyridoxine): Essential for neurotransmitter synthesis and nerve conduction
- B12 (Cyanocobalamin): Rebuilds the myelin sheath - the protective coating around nerves. This is the most important one for nerve recovery.
5. Tab Xalcort 6 mg (2+0+0 for 5 days only)
What is it?
Why prescribed?
- Significant nerve root irritation from compressed disc/osteophytes
- Acute inflammatory flare causing severe spasm
- Multiple sources of inflammation (disc, osteophytes, pseudo-joints from sacralization)
- Blocking the production of ALL inflammatory mediators (prostaglandins, leukotrienes, cytokines)
- Rapidly reducing nerve root swelling - this is the key benefit for spinal conditions
- Decreasing edema around the compressed nerve roots, giving them room to breathe
- Blood sugar rises
- Blood pressure increases
- Immune system is suppressed
- Bone density reduces (ironic in this case!)
- Adrenal gland suppression
6. Cap Exium 20 mg (1+0+1 for 10 days)
What is it?
Why prescribed?
| Medicine | Stomach Risk |
|---|---|
| Nabumet (NSAID) for 15 days | NSAIDs damage the stomach lining by blocking COX-1, which normally produces protective mucus |
| Xalcort (steroid) for 5 days | Steroids reduce the stomach's protective mucus layer |
| Both together | Combination of NSAID + steroid = very high risk of gastric ulcer or bleeding |
- The stomach lining is attacked from both sides
- Ulcers, gastritis, or even GI bleeding can occur
- The patient would have stomach pain, nausea, and heartburn
- Stomach acid is suppressed
- The lining heals and is protected
- The patient can safely take the NSAID and steroid without stomach damage
Summary Table - The Full Picture
| # | Medicine | Drug Class | Why Given | Duration |
|---|---|---|---|---|
| 1a | Bonigen | Calcium + Vit D3 | Bone density support, especially 40F with spinal degeneration | 15 days |
| 1b | Arth A TS | Glucosamine + Chondroitin | Cartilage repair support at degenerated discs | 30 days |
| 2 | Nabumet 500 | NSAID | Core anti-inflammatory for osteophytes + disc pain | 15 days |
| 3 | Flexibac 5mg | Muscle relaxant (Baclofen) | Relieve paravertebral spasm causing straightened lordosis | 7 days only |
| 4 | Neuro B | B1+B6+B12 vitamins | Nerve root protection + myelin repair from compression | 30 days |
| 5 | Xalcort 6mg | Oral steroid | Rapid powerful anti-inflammatory, reduce nerve root swelling | 5 days only |
| 6 | Exium 20mg | Proton pump inhibitor | Protect stomach from NSAID + steroid combination damage | 10 days |
How They Work Together as a Team
ACUTE PHASE (Days 1-5):
Xalcort (steroid) + Nabumet (NSAID) + Flexibac (muscle relaxant)
→ Rapidly kill inflammation + relax spasm
→ Exium protects the stomach throughout
TRANSITION PHASE (Days 6-15):
Nabumet continues → sustains pain/inflammation control
Flexibac stops at day 7 → spasm should be resolved by now
Bonigen running throughout → building bone/nerve support
LONG-TERM PHASE (Days 16-45):
Arth A TS → cartilage support
Neuro B → nerve healing
Important: Always take Nabumet and Exium with food to further protect the stomach. Take Xalcort in the morning only as prescribed. Do not stop any medicine early without consulting the doctor.
What should she do when medicines finish? Does she need physiotherapy next?
What Should Amena Begum Do After Medicines Finish?
First - Understand What the Medicines Did vs. What They Didn't Do
- ✅ Reduce inflammation (Nabumet + Xalcort)
- ✅ Relax the muscle spasm (Flexibac)
- ✅ Protect the stomach (Exium)
- ✅ Start nerve and bone support (Neuro B + Bonigen)
- ❌ Fix the sacralization (congenital - cannot be changed)
- ❌ Rebuild the disc space at L5-S1
- ❌ Reverse the osteophytes
- ❌ Strengthen the muscles supporting the spine
- ❌ Prevent the pain from coming back
Timeline After Medicines Finish
Day 1-30 (medicines running)
↓
Day 31 onwards: PHYSIOTHERAPY begins
↓
Month 3: Review with doctor + MRI if needed
↓
Month 6: Reassess - if good, maintain exercises lifelong
If not improving → consider injections
YES - She Needs Physiotherapy. Here Is Exactly What and Why:
Phase 1: First 2 Weeks of Physiotherapy
1. Heat Therapy (Thermotherapy)
- Apply a hot water bag or heating pad to the lower back for 15-20 minutes before any exercise
- Heat increases blood flow, relaxes the remaining muscle tightness, and makes the muscles more flexible before exercise
- Do this every morning
2. TENS (Transcutaneous Electrical Nerve Stimulation)
- Done by the physiotherapist
- Small electrical pulses are sent through pads placed on the lower back
- Blocks pain signals traveling to the brain
- Gives significant relief without any medicines
- Typically done 3 times per week in the clinic
3. Ultrasound Therapy (Physiotherapy clinic)
- Deep sound waves are directed into the lumbar area
- Reduces deep inflammation in the disc and facet joints
- Promotes tissue healing
- Cannot be done at home - needs a physiotherapist
4. Gentle Stretching (can do at home)
- Lie flat on back
- Pull one knee gently toward the chest
- Hold 20-30 seconds
- Repeat other side
- Do 10 repetitions each side, twice daily
- Why: Stretches the piriformis, hip flexors, and releases lower lumbar tension
- On all fours (hands and knees)
- Arch back up like a cat (hold 5 seconds)
- Then drop belly down like a cow (hold 5 seconds)
- 10 repetitions twice daily
- Why: Gently mobilizes the stiff L5-S1 and L4-L5 segments, restores lumbar movement
- Sit back on heels, reach arms forward on the floor
- Hold 30 seconds, 5 repetitions
- Why: Decompresses the lumbar spine, relieves pressure on osteophytes and disc
Phase 2: Weeks 3-6
1. Pelvic Tilt
- Lie on back, knees bent
- Flatten the lower back against the floor by tightening the abdominal muscles
- Hold 10 seconds, release
- 15 repetitions, twice daily
- Why: This is the foundation exercise - teaches the deep abdominal muscles to support the lumbar spine
2. Dead Bug Exercise
- Lie on back, arms pointing to the ceiling, knees bent at 90 degrees
- Slowly lower one arm behind head while straightening the opposite leg - without letting the lower back lift off the floor
- Return, repeat other side
- 10 repetitions each side
- Why: Trains the deep core (transversus abdominis + multifidus) to stabilize L4-L5 and L5-S1 without putting compressive force on the spine
3. Bird Dog
- On all fours
- Extend right arm forward and left leg back simultaneously
- Hold 5 seconds, switch sides
- 10 repetitions each side
- Why: The gold standard exercise for lumbar stabilization - directly strengthens the multifidus muscle, which is the main stabilizer of each individual vertebra
4. Bridge Exercise
- Lie on back, knees bent, feet flat on floor
- Lift hips off the floor until body is in a straight line from shoulders to knees
- Hold 5-10 seconds, lower slowly
- 15 repetitions, twice daily
- Why: Strengthens gluteus maximus and hamstrings, which reduce the load on the lumbar spine by taking over some of the weight-bearing function
5. Walking
- Start with 20 minutes of flat walking daily
- Build up to 30-40 minutes by week 4
- Why: Walking is the single best overall exercise for lumbar spondylosis. It:
- Pumps nutrients into the discs (discs have no blood supply - they get nutrition only through movement/compression)
- Maintains the natural lumbar lordosis
- Keeps weight in check (every extra kg = 4x extra force on lumbar spine)
Phase 3: Month 2-3 Onwards
Swimming
- Excellent for this patient - water supports body weight, removing spinal load
- Backstroke and breaststroke are ideal
- Avoids the flexion forces that worsen disc disease
- If a pool is available, 2-3 sessions per week is ideal
Yoga (specific poses only - NOT all yoga)
- Legs up the wall (Viparita Karani)
- Supine twist (gentle)
- Supported bridge
- Forward bends touching toes
- Heavy twisting poses
- Any pose causing pain
What Medicines Continue After the Course?
| Medicine | Status after course | Reason |
|---|---|---|
| Bonigen (15 days) | Continue long-term | A 40-year-old woman should stay on Calcium + Vit D3 indefinitely. Ask doctor to prescribe a maintenance dose (usually once daily). |
| Arth A TS (30 days) | Can repeat 3-month courses | Glucosamine/Chondroitin works best with 3-month courses, rest, then repeat. Discuss with doctor. |
| Neuro B (30 days) | May continue for 3-6 months | Nerve healing is slow. Doctor may extend this for another 1-2 months based on whether leg symptoms improve. |
| Nabumet (15 days) | Stop - use only during flares | Don't take daily long-term. If pain returns, short course only. |
| Flexibac (7 days) | Stop completely | Only for acute spasm. Not for long-term use. |
| Xalcort (5 days) | Stop completely | Short burst course. Do not repeat without doctor's advice. |
| Exium (10 days) | Stop - only take if needed | Stop once NSAIDs/steroids are done. Take again only if she takes NSAIDs in future. |
Lifestyle Changes - Non-Negotiable
Sitting
- Never sit for more than 30-40 minutes continuously without getting up and walking briefly
- Use a chair with lumbar support (or place a small rolled towel at the small of the back)
- Sit with hips slightly higher than knees - use a small cushion under the sitting bones if needed
- Avoid low sofas and floor-sitting (cross-legged)
Sleeping
- Sleep on a firm mattress (not too soft)
- Best position: On the side with a pillow between the knees - this keeps the spine aligned and reduces L4-L5 stress
- Avoid sleeping flat on the stomach - this forces the lumbar spine into hyperextension
Lifting
- Never bend from the waist to pick something up
- Always squat down (bend the knees, keep back straight) then lift
- Keep the object close to the body
- No heavy lifting (>5 kg) for at least 2-3 months
Weight
- If she is overweight, every 1 kg of weight loss = 4 kg less force on the lumbar spine
- A healthy BMI significantly slows disc degeneration
Diet
- Increase calcium-rich foods: milk, yogurt, sesame seeds, fish with bones
- Increase Vitamin D: sunlight exposure 15-20 minutes daily (morning sun)
- Anti-inflammatory foods: turmeric (haldi), ginger, omega-3 fatty acids (fish, flaxseed)
- Reduce: processed food, excess sugar (drives systemic inflammation)
When to Go Back to the Doctor
| Symptom | Urgency |
|---|---|
| Pain not improving after 6-8 weeks of physiotherapy | Book appointment |
| Pain or numbness spreading down one or both legs | Book soon |
| Weakness in legs, difficulty walking | Go urgently |
| Loss of bladder or bowel control | Go to emergency immediately |
| Worsening at night or at rest (could suggest different diagnosis) | Book appointment |
The Big Picture Plan
NOW (Medicines running):
└── Take all medicines as prescribed
└── Rest - avoid aggravating activities
└── Gentle walking only
AFTER MEDICINES (Month 1-2):
└── Start physiotherapy 3x/week
└── Begin home exercises daily
└── Continue Calcium + Neuro B
└── Lifestyle changes (sitting, sleeping, lifting)
MONTH 3:
└── Review with doctor
└── MRI if still symptomatic
└── Consider injection if physiotherapy not enough
MONTH 6 ONWARDS:
└── Maintenance exercises become lifelong habit
└── Swimming, walking, core work
└── Annual bone density check (DEXA scan) - important for 40F
Generate a lifestyle/dietary guide document for her
mkdir -p /tmp/workspace/amena-guide && ls /tmp/workspace/amena-guide/
~/amena-guide/create_guide.py
from docx import Document
from docx.shared import Pt, Inches, RGBColor
from docx.enum.text import WD_ALIGN_PARAGRAPH
from docx.oxml.ns import qn
from docx.oxml import OxmlElement
doc = Document()
# ── Page margins ──────────────────────────────────────────────────────────────
for section in doc.sections:
section.top_margin = Inches(1.0)
section.bottom_margin = Inches(1.0)
section.left_margin = Inches(1.1)
section.right_margin = Inches(1.1)
# ── Base style ────────────────────────────────────────────────────────────────
normal = doc.styles["Normal"]
normal.font.name = "Arial"
normal.font.size = Pt(11)
# ── Helper: set paragraph shading ─────────────────────────────────────────────
def shade_paragraph(para, hex_color):
pPr = para._p.get_or_add_pPr()
shd = OxmlElement("w:shd")
shd.set(qn("w:val"), "clear")
shd.set(qn("w:color"), "auto")
shd.set(qn("w:fill"), hex_color)
pPr.append(shd)
# ── Helper: coloured heading ───────────────────────────────────────────────────
def add_colored_heading(doc, text, level, hex_rgb):
h = doc.add_heading(text, level=level)
h.alignment = WD_ALIGN_PARAGRAPH.LEFT
for run in h.runs:
run.font.color.rgb = RGBColor(*bytes.fromhex(hex_rgb))
return h
# ── Helper: bullet paragraph ──────────────────────────────────────────────────
def add_bullet(doc, text, bold_prefix=None):
p = doc.add_paragraph(style="List Bullet")
p.paragraph_format.left_indent = Inches(0.3)
if bold_prefix:
run = p.add_run(bold_prefix + ": ")
run.bold = True
run.font.size = Pt(11)
p.add_run(text).font.size = Pt(11)
else:
r = p.add_run(text)
r.font.size = Pt(11)
return p
# ── Helper: table with header row ─────────────────────────────────────────────
def add_table(doc, headers, rows, col_widths=None):
table = doc.add_table(rows=1 + len(rows), cols=len(headers))
table.style = "Table Grid"
# Header row
hdr = table.rows[0]
for i, h in enumerate(headers):
cell = hdr.cells[i]
cell.text = h
for run in cell.paragraphs[0].runs:
run.bold = True
run.font.color.rgb = RGBColor(0xFF, 0xFF, 0xFF)
run.font.size = Pt(10)
# Blue background
tc_pr = cell._tc.get_or_add_tcPr()
shd = OxmlElement("w:shd")
shd.set(qn("w:val"), "clear")
shd.set(qn("w:color"), "auto")
shd.set(qn("w:fill"), "1F4E79")
tc_pr.append(shd)
# Data rows
for r_idx, row_data in enumerate(rows):
row = table.rows[r_idx + 1]
fill = "D6E4F0" if r_idx % 2 == 0 else "FFFFFF"
for c_idx, val in enumerate(row_data):
cell = row.cells[c_idx]
cell.text = str(val)
cell.paragraphs[0].runs[0].font.size = Pt(10)
tc_pr = cell._tc.get_or_add_tcPr()
shd = OxmlElement("w:shd")
shd.set(qn("w:val"), "clear")
shd.set(qn("w:color"), "auto")
shd.set(qn("w:fill"), fill)
tc_pr.append(shd)
if col_widths:
for i, w in enumerate(col_widths):
for row in table.rows:
row.cells[i].width = Inches(w)
return table
# ══════════════════════════════════════════════════════════════════════════════
# COVER / TITLE BLOCK
# ══════════════════════════════════════════════════════════════════════════════
# Decorative top bar (shaded paragraph)
bar = doc.add_paragraph()
bar.paragraph_format.space_before = Pt(0)
bar.paragraph_format.space_after = Pt(0)
shade_paragraph(bar, "1F4E79")
bar.add_run(" ").font.size = Pt(6)
doc.add_paragraph() # spacer
title_p = doc.add_paragraph()
title_p.alignment = WD_ALIGN_PARAGRAPH.CENTER
tr = title_p.add_run("Lifestyle & Dietary Guide")
tr.bold = True
tr.font.size = Pt(24)
tr.font.color.rgb = RGBColor(0x1F, 0x4E, 0x79)
sub_p = doc.add_paragraph()
sub_p.alignment = WD_ALIGN_PARAGRAPH.CENTER
sr = sub_p.add_run("For: Amena Begum | Age: 40 years | Female")
sr.font.size = Pt(12)
sr.font.color.rgb = RGBColor(0x44, 0x72, 0xC4)
sr.bold = True
diag_p = doc.add_paragraph()
diag_p.alignment = WD_ALIGN_PARAGRAPH.CENTER
dr = diag_p.add_run("Diagnosis: Bilateral Hemisacralization with Lumbar Spondylosis")
dr.font.size = Pt(11)
dr.italic = True
dr.font.color.rgb = RGBColor(0x70, 0x70, 0x70)
doc.add_paragraph()
bar2 = doc.add_paragraph()
bar2.paragraph_format.space_before = Pt(0)
bar2.paragraph_format.space_after = Pt(0)
shade_paragraph(bar2, "1F4E79")
bar2.add_run(" ").font.size = Pt(6)
doc.add_paragraph()
# Intro note
intro = doc.add_paragraph()
intro_r = intro.add_run(
"This guide was prepared specifically for your diagnosis. Your spine has a congenital "
"anomaly (bilateral hemisacralization of L5) combined with degenerative changes "
"(spondylosis). While surgery is rarely needed for this condition, your daily habits "
"are the most powerful tool you have. Follow this guide consistently — it will reduce "
"pain, slow degeneration, and improve your quality of life long-term."
)
intro_r.font.size = Pt(11)
intro_r.font.italic = True
intro.paragraph_format.left_indent = Inches(0.2)
intro.paragraph_format.right_indent = Inches(0.2)
shade_paragraph(intro, "EBF3FB")
doc.add_paragraph()
# ══════════════════════════════════════════════════════════════════════════════
# SECTION 1 — POSTURE & DAILY HABITS
# ══════════════════════════════════════════════════════════════════════════════
add_colored_heading(doc, "1. Posture & Daily Habits", 1, "1F4E79")
add_colored_heading(doc, "Sitting", 2, "2E74B5")
add_bullet(doc, "Never sit for more than 30-40 minutes continuously. Stand up, walk briefly, then sit again.", "Time limit")
add_bullet(doc, "Use a chair with firm lumbar (lower back) support. If your chair lacks this, place a small rolled towel or cushion at the small of your back.", "Chair support")
add_bullet(doc, "Sit with hips slightly higher than knees. Use a small cushion under the sitting bones if needed.", "Hip position")
add_bullet(doc, "Keep both feet flat on the floor — avoid crossing your legs.", "Foot position")
add_bullet(doc, "Avoid low sofas, floor-sitting, and sitting cross-legged (these all increase lumbar flexion stress).", "Avoid")
add_colored_heading(doc, "Sleeping", 2, "2E74B5")
add_bullet(doc, "Sleep on a FIRM mattress. A mattress that is too soft lets the spine sag and worsens pain.", "Mattress")
add_bullet(doc, "Best sleeping position: On your side with a pillow between your knees. This keeps the spine aligned and reduces L4-L5 and L5-S1 stress.", "Best position")
add_bullet(doc, "Second option: On your back with a pillow under your knees (not under the head alone).", "Alternative")
add_bullet(doc, "Avoid sleeping on your stomach — this forces the lumbar spine into hyperextension and worsens your condition.", "Avoid")
add_colored_heading(doc, "Lifting & Bending", 2, "2E74B5")
add_bullet(doc, "NEVER bend forward from the waist to pick something up. This is the single most damaging movement for your spine.", "Critical rule")
add_bullet(doc, "Always squat down (bend the knees, keep back straight and upright), then lift. Keep the object close to your body.", "Correct technique")
add_bullet(doc, "Avoid lifting objects heavier than 5 kg for at least the first 2-3 months.", "Weight limit")
add_bullet(doc, "When carrying bags or shopping, divide the weight equally between both hands.", "Carrying")
add_colored_heading(doc, "Standing", 2, "2E74B5")
add_bullet(doc, "Avoid standing in one position for more than 20-30 minutes. Shift your weight or walk in place.", "Time limit")
add_bullet(doc, "When working at a kitchen counter or sink, place one foot on a small step or footrest to reduce lumbar stress.", "Kitchen tip")
add_bullet(doc, "Wear flat, cushioned shoes — avoid high heels completely. High heels tilt the pelvis and increase lumbar lordosis stress.", "Footwear")
doc.add_paragraph()
# ══════════════════════════════════════════════════════════════════════════════
# SECTION 2 — EXERCISE & PHYSIOTHERAPY
# ══════════════════════════════════════════════════════════════════════════════
add_colored_heading(doc, "2. Exercise & Physiotherapy Plan", 1, "1F4E79")
note_p = doc.add_paragraph(
"Physiotherapy is not optional — it is the treatment that prevents pain from returning. "
"Start after completing your medicines. A physiotherapist should supervise the first few sessions."
)
note_p.runs[0].italic = True
note_p.runs[0].font.size = Pt(11)
shade_paragraph(note_p, "FFF2CC")
doc.add_paragraph()
add_colored_heading(doc, "Phase 1 — Weeks 1-2 After Medicines (Restore Movement)", 2, "2E74B5")
add_bullet(doc, "Apply a hot water bag or heating pad to the lower back for 15-20 minutes every morning before exercise.", "Heat therapy")
add_bullet(doc, "Knee-to-Chest Stretch: Lie on back, pull one knee gently to chest, hold 20-30 seconds, switch sides. 10 reps each side, twice daily.", "Stretch 1")
add_bullet(doc, "Cat-Cow: On all fours, arch back up (hold 5 sec), then drop belly down (hold 5 sec). 10 reps twice daily.", "Stretch 2")
add_bullet(doc, "Child's Pose: Sit back on heels, reach arms forward. Hold 30 seconds, 5 repetitions.", "Stretch 3")
add_bullet(doc, "Walking: Start with 15-20 minutes of flat walking daily. Builds disc nutrition and maintains lordosis.", "Walking")
add_colored_heading(doc, "Phase 2 — Weeks 3-6 (Core Strengthening — MOST IMPORTANT)", 2, "2E74B5")
add_bullet(doc, "Pelvic Tilt: Lie on back, knees bent. Flatten lower back against floor by tightening abdomen. Hold 10 sec. 15 reps twice daily.", "Exercise 1")
add_bullet(doc, "Dead Bug: Lie on back, arms up, knees at 90°. Lower one arm + opposite leg slowly, keeping back flat. 10 reps each side.", "Exercise 2")
add_bullet(doc, "Bird-Dog: On all fours, extend right arm + left leg simultaneously. Hold 5 sec. 10 reps each side.", "Exercise 3")
add_bullet(doc, "Bridge: Lie on back, lift hips until body is straight from shoulders to knees. Hold 5-10 sec. 15 reps twice daily.", "Exercise 4")
add_bullet(doc, "Increase walking to 30-40 minutes daily.", "Walking")
add_colored_heading(doc, "Phase 3 — Month 2 Onwards (Long-term Maintenance)", 2, "2E74B5")
add_bullet(doc, "Swimming: 2-3 sessions per week. Backstroke and breaststroke are ideal. Water supports body weight and removes spinal load.", "Swimming")
add_bullet(doc, "Continue core exercises (Bird-Dog, Bridge, Dead Bug) as a permanent daily habit — even after pain is gone.", "Maintenance")
add_bullet(doc, "Continue 30-40 minutes of walking 5-7 days per week.", "Walking")
add_colored_heading(doc, "Exercises to AVOID", 2, "C00000")
add_bullet(doc, "Toe-touching / forward bending exercises")
add_bullet(doc, "Sit-ups and crunches (high lumbar flexion stress)")
add_bullet(doc, "Running or jogging on hard surfaces")
add_bullet(doc, "Heavy weight lifting (gym deadlifts, squats with weights)")
add_bullet(doc, "Any exercise that causes pain — stop immediately")
doc.add_paragraph()
# ══════════════════════════════════════════════════════════════════════════════
# SECTION 3 — DIETARY GUIDE
# ══════════════════════════════════════════════════════════════════════════════
add_colored_heading(doc, "3. Dietary Guide", 1, "1F4E79")
add_colored_heading(doc, "Foods to Eat Daily (Anti-inflammatory & Bone-Supporting)", 2, "2E74B5")
add_table(
doc,
headers=["Food Group", "Examples", "Why It Helps"],
rows=[
("Calcium-rich foods", "Milk, yogurt, cheese, small fish with bones, sesame seeds (til), almonds",
"Maintains bone density; critical for 40-year-old woman"),
("Vitamin D sources", "Egg yolk, fatty fish (salmon, hilsa/ilish), fortified milk, morning sunlight 15-20 min/day",
"Without Vit D, calcium cannot be absorbed. Sunlight is the best source."),
("Anti-inflammatory", "Turmeric (haldi) in meals, ginger tea, green leafy vegetables, berries",
"Reduces systemic inflammation that drives disc pain and osteophyte growth"),
("Omega-3 fatty acids", "Fish (especially fatty fish), flaxseed (tisi), walnuts, mustard oil",
"Powerfully anti-inflammatory; protects disc and nerve tissue"),
("Vitamin B12 foods", "Eggs, milk, fish, meat, yogurt",
"Supports nerve myelin repair; important alongside Neuro B supplement"),
("Magnesium-rich foods", "Spinach, pumpkin seeds, bananas, dark chocolate (small amount), lentils (dal)",
"Reduces muscle cramps and spasm; supports bone mineral matrix"),
("Collagen & joint foods", "Bone broth, chicken skin soup, gelatin",
"Provides building blocks for disc cartilage repair"),
("Hydration", "8-10 glasses of water daily",
"Intervertebral discs are 70-90% water when healthy. Dehydration accelerates disc degeneration."),
],
col_widths=[1.5, 2.5, 2.5]
)
doc.add_paragraph()
add_colored_heading(doc, "Foods to REDUCE or AVOID", 2, "C00000")
add_table(
doc,
headers=["Avoid / Reduce", "Why"],
rows=[
("Processed & packaged foods (chips, instant noodles, fast food)",
"High in sodium and trans fats — drive systemic inflammation, worsen joint pain"),
("Excess sugar, soft drinks, sweetened juices",
"Sugar promotes inflammatory cytokines that directly worsen disc degeneration"),
("Red meat in large amounts",
"Contains arachidonic acid which increases inflammatory prostaglandins"),
("Caffeine (excess tea/coffee — more than 2 cups/day)",
"Blocks calcium absorption; can worsen bone loss especially in women over 40"),
("Alcohol",
"Inhibits calcium absorption, damages bone density, interferes with nerve healing"),
("High-salt foods (pickles, salted crackers, canned food)",
"Excess sodium causes calcium excretion through urine, weakening bones"),
("Carbonated drinks",
"Phosphoric acid in sodas directly leaches calcium from bones"),
],
col_widths=[2.8, 3.7]
)
doc.add_paragraph()
add_colored_heading(doc, "Sample Daily Meal Plan", 2, "2E74B5")
add_table(
doc,
headers=["Meal", "Suggested Foods"],
rows=[
("Early morning (on waking)",
"1 glass warm water + 5 soaked almonds + 1 tsp turmeric in warm milk (golden milk)"),
("Breakfast",
"2 eggs (boiled/scrambled) + 1-2 roti with vegetables + 1 glass milk OR oats with milk and banana"),
("Mid-morning snack",
"1 small cup yogurt (dahi) + a handful of sesame seeds OR a small bowl of mixed nuts"),
("Lunch",
"Rice/roti + dal (lentil soup) + fish curry (ilish/small fish with bones) + green vegetable sabzi + salad"),
("Afternoon",
"1 cup ginger tea (not too strong) + fruit (banana, orange, or papaya)"),
("Dinner",
"Roti/rice + chicken or fish + cooked vegetables + 1 small bowl yogurt"),
("Before bed",
"1 glass warm milk (calcium absorption is best at night)"),
],
col_widths=[2.0, 4.5]
)
doc.add_paragraph()
# ══════════════════════════════════════════════════════════════════════════════
# SECTION 4 — WEIGHT MANAGEMENT
# ══════════════════════════════════════════════════════════════════════════════
add_colored_heading(doc, "4. Weight Management", 1, "1F4E79")
wt_p = doc.add_paragraph(
"Every extra 1 kg of body weight = approximately 4 kg of additional force on the lumbar spine. "
"This directly worsens the osteophytes at L4-L5 and accelerates disc degeneration at L5-S1. "
"Weight management is therefore a medical necessity for your condition, not just cosmetic."
)
wt_p.runs[0].font.size = Pt(11)
shade_paragraph(wt_p, "EBF3FB")
doc.add_paragraph()
add_bullet(doc, "Calculate your BMI (weight in kg ÷ height in m²). Target: 18.5-24.9.", "Target BMI")
add_bullet(doc, "If overweight: aim to lose 0.5-1 kg per week through diet + walking. Do not crash diet.", "Weight loss rate")
add_bullet(doc, "Daily walking (30-40 min) is your best calorie-burning exercise that does not stress the spine.", "Best exercise")
add_bullet(doc, "Avoid skipping meals — this leads to overeating and poor nutrient absorption.", "Meal regularity")
add_bullet(doc, "Eat slowly and chew well — this improves digestion and prevents overeating.", "Eating habit")
doc.add_paragraph()
# ══════════════════════════════════════════════════════════════════════════════
# SECTION 5 — MEDICINES & SUPPLEMENTS AFTER COURSE
# ══════════════════════════════════════════════════════════════════════════════
add_colored_heading(doc, "5. Medicines & Supplements After the Course Ends", 1, "1F4E79")
add_table(
doc,
headers=["Medicine", "After Course — What to Do"],
rows=[
("Bonigen (Calcium + Vit D3)",
"CONTINUE long-term. 40-year-old women need ongoing calcium support. Ask doctor for a maintenance once-daily dose."),
("Arth A TS (Glucosamine + Chondroitin)",
"Repeat 3-month courses with a break in between. Discuss timing with doctor."),
("Neuro B (Vitamin B1+B6+B12)",
"May continue for 3-6 months total if leg tingling/numbness is still present. Ask doctor."),
("Nabumet (NSAID)",
"STOP regular use. Only take during painful flares, short-term, with food."),
("Flexibac (Baclofen)",
"STOP completely. Not for long-term use."),
("Xalcort (Steroid)",
"STOP completely. Do not repeat without doctor's prescription."),
("Exium (Esomeprazole PPI)",
"STOP. Take again only if/when you restart NSAIDs."),
],
col_widths=[2.0, 4.5]
)
doc.add_paragraph()
# ══════════════════════════════════════════════════════════════════════════════
# SECTION 6 — WARNING SIGNS
# ══════════════════════════════════════════════════════════════════════════════
add_colored_heading(doc, "6. Warning Signs — When to See the Doctor Urgently", 1, "1F4E79")
warn_p = doc.add_paragraph(
"Go to the doctor immediately if you experience ANY of the following:"
)
warn_p.runs[0].bold = True
warn_p.runs[0].font.color.rgb = RGBColor(0xC0, 0x00, 0x00)
add_bullet(doc, "Pain spreading down one or both legs (sciatica/radiculopathy getting worse)")
add_bullet(doc, "Numbness, tingling, or weakness in the legs or feet")
add_bullet(doc, "Difficulty walking or leg gives way")
add_bullet(doc, "Loss of bladder or bowel control — GO TO EMERGENCY IMMEDIATELY")
add_bullet(doc, "Severe pain that is not relieved by rest or medicines")
add_bullet(doc, "Pain that is worse at night and at rest (this suggests a different diagnosis)")
add_bullet(doc, "Fever with back pain (could indicate spinal infection)")
doc.add_paragraph()
# ══════════════════════════════════════════════════════════════════════════════
# SECTION 7 — FOLLOW-UP SCHEDULE
# ══════════════════════════════════════════════════════════════════════════════
add_colored_heading(doc, "7. Follow-up & Review Schedule", 1, "1F4E79")
add_table(
doc,
headers=["When", "What to Do"],
rows=[
("After medicines finish (Day 30-35)",
"Start physiotherapy. Begin home exercises. Continue Calcium + Neuro B."),
("6-8 weeks after starting physiotherapy",
"Review with doctor. Report progress. Doctor may order MRI lumbar spine at this point."),
("Month 3",
"Reassess pain levels and function. If improved — continue exercises. If not — discuss injection therapy."),
("Month 6",
"Full review. Consider DEXA bone density scan (important for women over 40 with spinal issues)."),
("Annually",
"Annual check-up. Repeat bone density if needed. Continue lifestyle habits permanently."),
],
col_widths=[2.0, 4.5]
)
doc.add_paragraph()
# ══════════════════════════════════════════════════════════════════════════════
# CLOSING NOTE
# ══════════════════════════════════════════════════════════════════════════════
add_colored_heading(doc, "A Final Note", 1, "1F4E79")
close_p = doc.add_paragraph(
"Your condition — bilateral hemisacralization with spondylosis — is manageable. "
"You were born with the spinal anomaly, but how quickly the degeneration progresses "
"is largely in your hands. The exercises, dietary changes, and posture habits in this "
"guide are not temporary fixes. Make them a permanent part of your life and you will "
"see a significant and lasting improvement in your pain, mobility, and quality of life.\n\n"
"Be consistent. Be patient. The spine heals slowly, but it does heal."
)
close_p.runs[0].font.size = Pt(11)
close_p.runs[0].italic = True
shade_paragraph(close_p, "E2EFDA")
doc.add_paragraph()
# Bottom bar
bar3 = doc.add_paragraph()
bar3.paragraph_format.space_before = Pt(0)
bar3.paragraph_format.space_after = Pt(0)
shade_paragraph(bar3, "1F4E79")
bar3.add_run(" ").font.size = Pt(6)
# ── Save ──────────────────────────────────────────────────────────────────────
out_path = "/tmp/workspace/amena-guide/Amena_Lifestyle_Dietary_Guide.docx"
doc.save(out_path)
print(f"Saved: {out_path}")
cd /tmp/workspace/amena-guide && python3 create_guide.py
python3 -c " from docx import Document doc = Document('/tmp/workspace/amena-guide/Amena_Lifestyle_Dietary_Guide.docx') for p in doc.paragraphs[:30]: if p.text.strip(): print(f'[{p.style.name}] {p.text[:80]}') "
Amena Lifestyle Dietary Guide
Word Document · DOCX
What's Inside the Document
| Section | Content |
|---|---|
| 1. Posture & Daily Habits | Sitting, sleeping, lifting, standing rules with specific tips |
| 2. Exercise & Physiotherapy Plan | 3-phase exercise program (Weeks 1-2, 3-6, Month 2+) with exercises to avoid |
| 3. Dietary Guide | Full color table of foods to eat daily + foods to avoid + a complete sample daily meal plan |
| 4. Weight Management | Why weight matters for her spine + practical tips |
| 5. Medicines After Course | What to continue, what to stop, what to repeat |
| 6. Warning Signs | Red flag symptoms requiring urgent medical attention |
| 7. Follow-up Schedule | Month-by-month review timeline from Day 30 to annually |
Please repeat
Amena Lifestyle Dietary Guide
Word Document · DOCX
What's Inside the Document
| Section | Content |
|---|---|
| 1. Posture & Daily Habits | Sitting, sleeping, lifting, and standing rules with specific practical tips |
| 2. Exercise & Physiotherapy Plan | 3-phase exercise program (Weeks 1-2, Weeks 3-6, Month 2+) with a list of exercises to avoid |
| 3. Dietary Guide | Color table of foods to eat daily + foods to avoid + a complete sample daily meal plan |
| 4. Weight Management | Why weight matters for her spine + practical tips |
| 5. Medicines After Course | What to continue, what to stop, what to repeat with doctor |
| 6. Warning Signs | Red flag symptoms that need urgent medical attention |
| 7. Follow-up Schedule | Month-by-month review timeline from Day 30 all the way to annually |