hemi diaphragm
Reading File
Finding Sources
Searching the Web
elevated hemidiaphragm causes clinical significance radiology
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information to give a thorough answer. Let me compile everything.
Hemidiaphragm
The term "hemidiaphragm" refers to one half (left or right) of the dome-shaped musculotendinous diaphragm that separates the thoracic and abdominal cavities. Clinically, it is most commonly encountered as the elevated hemidiaphragm - an important radiological sign with a broad differential.
Anatomy
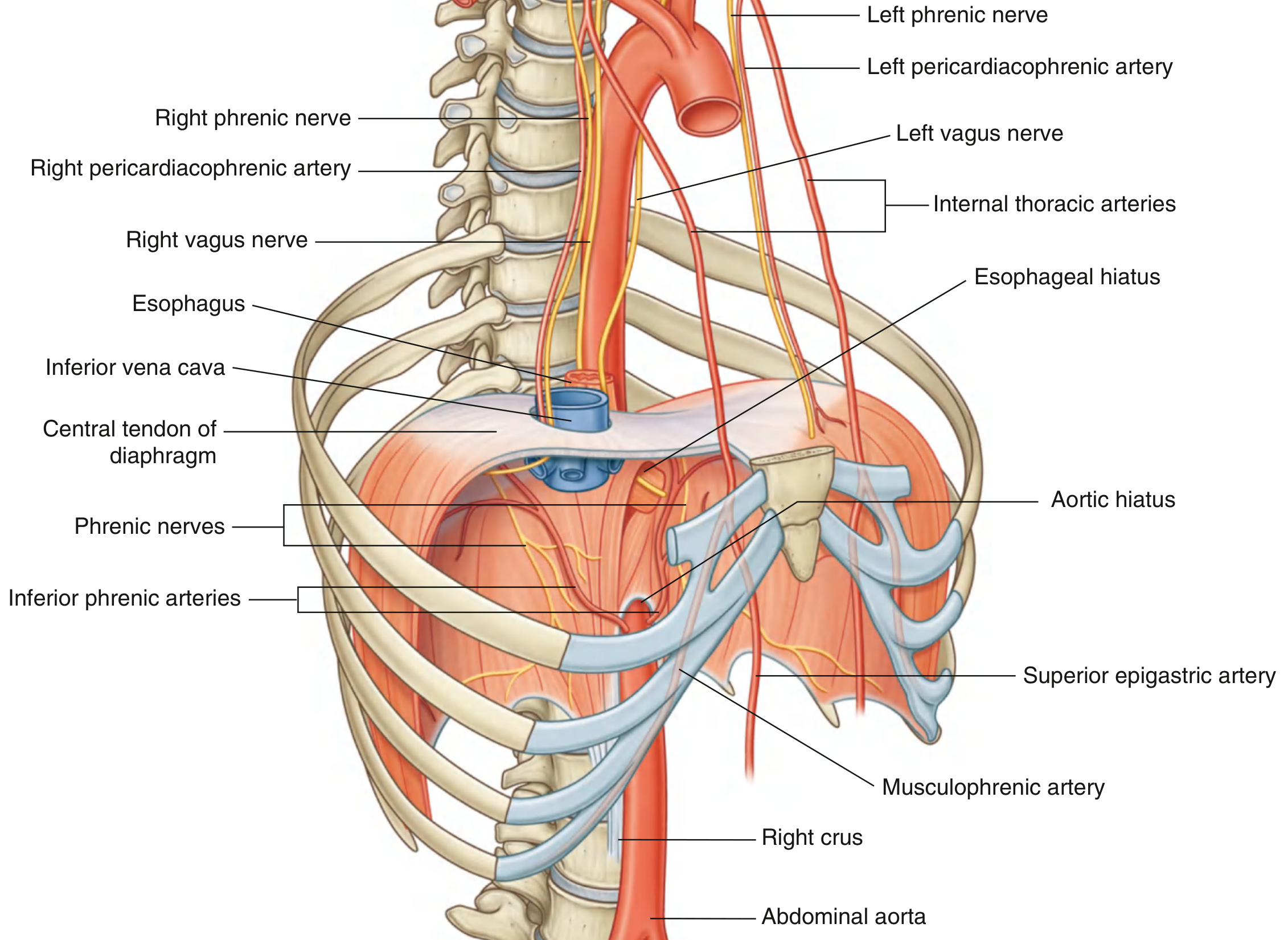
The diaphragm is a thin musculotendinous structure filling the inferior thoracic aperture. Peripheral muscle fibers converge on a central tendon, to which the pericardium is attached.
Attachments:
- Sternal - xiphoid process
- Costal - 6th to 12th ribs (costal margin + ends of ribs XI and XII)
- Lumbar - arcuate ligaments, right crus to L3, left crus to L2; median arcuate ligament crosses the aorta
Key openings (hiatuses):
| Opening | Level | Contents |
|---|---|---|
| Caval hiatus (central tendon) | T8 | Inferior vena cava, right phrenic nerve |
| Oesophageal hiatus | T10 | Oesophagus, vagus nerves |
| Aortic hiatus (posterior to diaphragm) | T12 | Aorta, thoracic duct, azygos/hemiazygos veins |
Innervation: Phrenic nerves (C3, C4, C5) - "C3, 4, 5 keep the diaphragm alive." They innervate the diaphragm from its abdominal surface. The sensory supply of the periphery is from the lower intercostal nerves (T5-T11), which is why subphrenic irritation can refer pain to the shoulder tip (phrenic) or the anterior thoracic/abdominal wall (intercostal).
Blood supply:
-
From above: pericardiacophrenic and musculophrenic arteries (branches of internal thoracic arteries); superior phrenic arteries from the thoracic aorta
-
From below: inferior phrenic arteries (the largest supply, directly from the abdominal aorta)
-
Gray's Anatomy for Students, p. 198
Normal Radiological Appearances
On a PA chest X-ray, each hemidiaphragm is a smooth, curved line convex upward. The right typically lies at the level of the 5th or 6th anterior rib interspace at full inspiration.
-
In >90% of normal people, the right hemidiaphragm is higher than the left (difference ~15 mm, up to 30 mm is still normal). This is because the liver elevates the right, and the gastric air bubble lowers the left.
-
The left hemidiaphragm is often partially obscured anteriorly by the heart.
-
The costophrenic angle should be sharply defined and acute - blunting suggests pleural fluid.
-
Grainger & Allison's Diagnostic Radiology, p. 78
Elevated Hemidiaphragm
Diaphragmatic paralysis should be suspected when an entire hemidiaphragm is elevated by >2 cm compared with the contralateral side.
Unilateral Elevation - Causes
The causes are organized by anatomical level:
Pulmonary/pleural (above the diaphragm):
- Pulmonary collapse / atelectasis
- Pulmonary hypoplasia
- Pneumonia or pleurisy
- Pulmonary thromboembolism
Diaphragm itself:
- Phrenic nerve palsy (most important - see below)
- Eventration (congenital focal weakness, forming a focal bulge)
- Diaphragmatic rupture / traumatic hernia
Subphrenic (below the diaphragm):
- Subphrenic abscess or infection
- Subphrenic mass (liver tumour, hepatomegaly, splenic mass)
- Gaseous distension of stomach or colon
Positional/structural:
- Lateral decubitus position (dependent side)
- Dorsal scoliosis
- Rib fracture and other painful conditions
Mimics of elevated hemidiaphragm:
-
Subpulmonary pleural effusion
-
Large well-defined tumour adjacent to the dome
-
Combined middle and lower lobe collapse
-
Grainger & Allison's Diagnostic Radiology, Table 3.4
Bilateral Elevation - Causes
| Cause |
|---|
| Supine position |
| Poor inspiratory effort |
| Obesity |
| Pregnancy |
| Abdominal distension (ascites, obstruction, mass) |
| Diffuse pulmonary fibrosis |
| Lymphangitis carcinomatosa |
| Disseminated SLE |
| Bilateral basal pulmonary emboli |
| Painful conditions (e.g., post-abdominal surgery) |
| Bilateral diaphragmatic paralysis |
- Grainger & Allison's Diagnostic Radiology, Table 3.3
Diaphragmatic Paralysis
Unilateral diaphragmatic paralysis (phrenic nerve palsy) is the most clinically significant cause of an elevated hemidiaphragm.
Common causes of phrenic nerve palsy:
- Malignancy (lung cancer invading the mediastinum is the most common)
- Cardiac/thoracic surgery (post-operative phrenic nerve injury - occurs in 2-20% of cardiac surgeries)
- Cervical spine disease
- Neuralgic amyotrophy (Parsonage-Turner syndrome)
- Mediastinal pathology (lymphoma, aortic aneurysm)
- Idiopathic
Diagnosis:
-
CXR: hemidiaphragm elevated by >2 cm compared with the normal side
-
Fluoroscopic sniff test (gold standard): paradoxical upward (cephalad) motion of the paralyzed hemidiaphragm with a sharp sniff maneuver, while the normal side descends
-
Ultrasound: paralyzed hemidiaphragm is thinner at rest (~1-2 mm vs normal ~2-3 mm), shows little thickening during inspiration, and may move paradoxically. The contralateral working hemidiaphragm thickens more than normal to compensate.
-
Fishman's Pulmonary Diseases and Disorders; Murray & Nadel's Textbook of Respiratory Medicine
Eventration
Eventration is a focal weakness or thinning of the diaphragmatic muscle resulting in a focal bulge or protrusion, most commonly on the right side (the most common diaphragmatic abnormality overall). A minor eventration is often an incidental finding. A large eventration (especially left-sided) can simulate diaphragmatic hernia and may contain viscera.
Diaphragmatic Hernias
When a hemidiaphragm is newly elevated following blunt trauma, traumatic diaphragmatic rupture with herniation must be excluded. Features:
- More common on the left (the liver protects the right side)
- Herniation of abdominal viscera may occur days to years after the trauma
- CT/MRI in coronal and sagittal planes is the reference standard
Other hernia types: Hiatal (most common, through the oesophageal hiatus), Morgagni (anterior/medial), Bochdalek (posterior/central - more often diagnosed in infancy).
- Fishman's Pulmonary Diseases and Disorders, p. 519
Quick Summary Table
| Feature | Right Hemidiaphragm | Left Hemidiaphragm |
|---|---|---|
| Normal height | Higher (liver underneath) | Lower (gastric bubble) |
| Landmarks | 5th-6th anterior rib space | Slightly lower than right |
| Distinction | Right dome clearly visible | Partially obscured by heart anteriorly |
| Phrenic nerve palsy | More commonly right (cardiac surgery) | Lung cancer invasion |
This is a shared conversation. Sign in to Orris to start your own chat.