How to manage the exess Cortisol production in a female body
Reading File
Finding Sources
Searching PubMed
"Cushing syndrome"[MeSH Terms] AND "treatment"[MeSH Terms]
Searching the Web
excess cortisol Cushing syndrome management women 2025 guidelines
Finding Sources
Searching PubMed
"Cushing syndrome" AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive guide to managing excess cortisol production (Cushing's syndrome) in women.
Managing Excess Cortisol Production (Cushing's Syndrome) in Women
Why Women Are More Affected
Cushing's syndrome is 3–6× more common in women than men. The classic presentation — first described by Harvey Cushing in 1912 in a young female — includes truncal/visceral obesity, hirsutism, amenorrhea, muscle weakness, easy bruising, moon face, dorsocervical fat pad ("buffalo hump"), purple abdominal striae, and insulin resistance. Untreated, it carries a 5× excess mortality, primarily cardiovascular. — Sabiston Textbook of Surgery
Step 1: Identify the Cause First
Management is entirely dependent on the underlying cause. The algorithm below guides the workup:
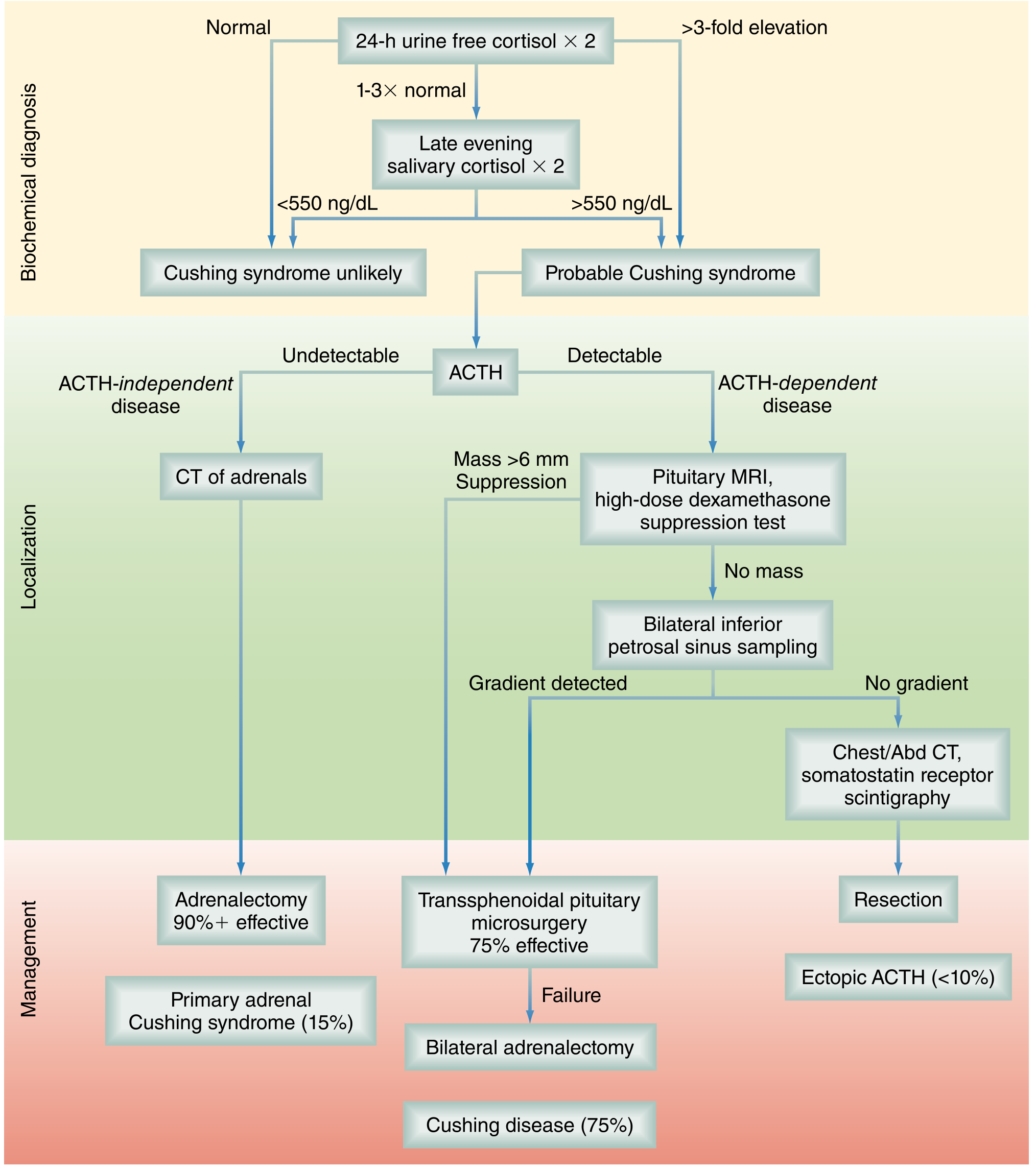
| Cause | Frequency | Key Feature |
|---|---|---|
| Cushing disease (ACTH-secreting pituitary adenoma) | ~75% | ACTH detectable, pituitary mass on MRI |
| Primary adrenal adenoma/carcinoma | ~15% | Undetectable ACTH |
| Ectopic ACTH (neuroendocrine tumors) | <10% | ACTH detectable, no pituitary suppression |
| Exogenous steroids | Most common overall | History of glucocorticoid use |
Step 2: Surgical Treatment (First-Line)
A. Cushing Disease (Pituitary Source — 75%)
Transsphenoidal selective adenomectomy (TSS) is first-line and ~75% effective.
- Postoperative: cortisol is withheld to assess remission; a subnormal morning cortisol on POD 1–2 confirms cure.
- Glucocorticoid supplementation continues until the HPA axis recovers — often ≥6 months.
- If TSS fails: bilateral adrenalectomy is the next step.
B. Primary Adrenal Cushing (ACTH-Independent — 15%)
Adrenalectomy (laparoscopic preferred) is >90% effective.
- Perioperative stress-dose steroids required: hydrocortisone 100 mg IV q8h × 24 h.
- Post-op HPA axis suppression can last >1 year — slow taper is essential.
C. Ectopic ACTH (<10%)
Resection of the offending tumor (lung, thymic, or pancreatic neuroendocrine tumor). If occult or unresectable → bilateral adrenalectomy as a life-preserving measure.
Step 3: Medical Therapy (Adjunct or When Surgery Is Not Possible)
Used when surgery fails, is not feasible, or as a bridge to surgery/radiation. Median cortisol control rate with medical therapy ~75%. — Mulholland and Greenfield's Surgery
Adrenal Steroidogenesis Inhibitors (Most Commonly Used)
| Drug | Mechanism | Key Notes |
|---|---|---|
| Ketoconazole | Inhibits CYP11B1/CYP17 (17α-hydroxylase, 11β-hydroxylase) | Most widely used (~26.5% of centers); hepatotoxic — monitor LFTs |
| Metyrapone | Blocks 11β-hydroxylase → reduces cortisol | Useful as a bridge; may cause hirsutism and hypertension in women |
| Osilodrostat | Potent 11β-hydroxylase inhibitor | Newer, FDA-approved; faster onset |
| Mitotane | Adrenolytic + steroidogenesis inhibitor | Used mainly for adrenocortical carcinoma; slow to act |
| Etomidate | IV, rapid onset; inhibits 11β-hydroxylase | For acute, severe hypercortisolism crises |
Cortisol Receptor Blocker
| Drug | Mechanism | Notes for Women |
|---|---|---|
| Mifepristone | Cortisol + progesterone receptor blocker | FDA-approved for Cushing's with hyperglycemia; causes uterine hyperplasia — monitor endometrium; not suitable in pregnancy |
Pituitary-Targeted Agents (Cushing Disease Only)
| Drug | Mechanism | Notes |
|---|---|---|
| Pasireotide | Somatostatin receptor agonist (SSTR 1,2,3,5) | 0.3–0.9 mg SC twice daily; 73% develop hyperglycemia |
| Cabergoline | Dopamine agonist | ~30% remission rate; not FDA-approved for Cushing's; control may escape after 2 years |
Combination therapy is used when monotherapy fails to normalize hypercortisolemia.
Step 4: Radiation Therapy
A third-line option when surgery fails and medical therapy is poorly tolerated. Stereotactic radiosurgery (Gamma Knife) takes months to years to normalize cortisol, so medical therapy bridges the gap.
Step 5: Managing Comorbidities (Critical in Women)
Cushing's causes multi-system damage that requires concurrent treatment:
| Comorbidity | Management |
|---|---|
| Hypertension (>70% of cases) | ACE inhibitors, spironolactone (also addresses hypokalemia) |
| Osteoporosis | Bisphosphonates, calcium/vitamin D; bone mineral density monitoring |
| Hyperglycemia/Type 2 diabetes | Metformin, insulin; especially vigilant if on pasireotide |
| Dyslipidemia | Statins |
| Thromboembolism | Consider prophylactic anticoagulation, especially perioperatively |
| Psychiatric symptoms | ~50% develop depression, anxiety, cognitive dysfunction; treat concurrently |
| Amenorrhea/infertility | Usually resolves with cortisol normalization; counsel on recovery timeline |
| Hirsutism | Often improves with cortisol control; anti-androgens if persistent |
Female-Specific Considerations
- Pregnancy: Cushing's is rare in pregnancy but life-threatening. Surgery (adrenalectomy in 2nd trimester if possible) is preferred over medical therapy. Metyrapone and ketoconazole have teratogenic risks.
- Mifepristone is contraindicated in women who are or wish to become pregnant (progesterone antagonism).
- Metyrapone can worsen hirsutism in women by increasing androgen precursors — weigh against alternatives.
- Oral contraceptives raise cortisol-binding globulin, which can interfere with interpretation of serum cortisol levels during monitoring.
Key References
- Sabiston Textbook of Surgery, Chapter 75 — Cushing Syndrome
- Mulholland and Greenfield's Surgery, Chapter 78 — Cushing Disease medications table
- Katzung's Basic & Clinical Pharmacology, 16th Ed. — Metyrapone
- Nieman LK et al., "Cushing syndrome." Nat Rev Dis Primers 2025 Jan — PMID: 39848955
- Reincke M, Fleseriu M. "Cushing Syndrome: A Review." JAMA 2023 — PMID: 37432427
This is a shared conversation. Sign in to Orris to start your own chat.