Non union or delayed union for long question answer for university examination
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
non-union fracture X-ray classification hypertrophic atrophic
I now have all the material needed for a comprehensive university examination answer. Here is the full long-answer response:
Non-Union and Delayed Union of Fractures
DEFINITIONS
Delayed Union occurs when a fracture takes an unduly longer time than is normally expected for union of that particular fracture at that particular site, yet still retains the potential to heal without operative intervention. The fracture is progressing toward union, just at a slower rate.
Non-Union means that bony union of the fracture is not possible without operative intervention. The fracture healing process has completely ceased. The bone ends become joined by fibrous tissue instead of bone. There is no potential for spontaneous healing.
Temporal thresholds used conventionally: >3 months for delayed union; >6–8 months for non-union — though these are arbitrary and context-dependent (Rockwood & Green, 10th ed.).
NORMAL FRACTURE HEALING (Brief Recap)
Understanding deviations requires knowing the norm:
- Haematoma formation → fibrous callus
- Primary (soft) callus — cartilaginous bridging
- Secondary (hard) callus — ossification
- Remodelling — Wolff's law
Non-union occurs when there is cessation of the reparative process antecedent to bony union. In delayed union, it is specifically the failure of the periosteal (not the endosteal) healing response prior to fracture bridging.
INCIDENCE
- Overall rate of non-union is approximately 4.9% of all fractures.
- Combined prevalence of impaired fracture healing (delayed union + non-union) is estimated at 6.9%.
- In open fractures with extensive soft tissue damage, the incidence of non-union approaches 20%.
- Non-union has health-related quality of life scores worse than stroke, diabetes, and AIDS — reflecting the serious disability it imposes.
CAUSES / RISK FACTORS
Causes are best grouped into three categories:
A. Patient (Host) Factors
| Factor | Mechanism |
|---|---|
| Advanced age | Reduced osteogenic potential |
| Diabetes mellitus | Impaired vascularity, neuropathy, immune dysfunction |
| Smoking | Vasoconstriction → ↓ blood supply; directly inhibits osteoblasts |
| Malnutrition / Vitamin D deficiency | Deficient substrate for mineralisation |
| Osteoporosis | Poor bone stock |
| Renal disease | Impaired Ca²⁺/phosphate metabolism |
| NSAIDs, steroids, chemotherapy, opioids, anticoagulants | Pharmacologic inhibition of healing |
| Obesity | Mechanical overload; hormonal effects |
| Collagen/metabolic bone disease | Structurally deficient matrix |
B. Local / Injury Factors
- Infection: The most common cause of non-union; infection leads to persistent bone resorption and prevents bridging
- Interposition of soft tissue (muscle or periosteum) between bone ends
- Inadequate blood supply: e.g. lower half of tibia, femoral neck, scaphoid waist, talar neck — watershed or end-arterial zones
- Wide separation of fragments: e.g. fracture of patella, olecranon (distracted by muscle pull), or excessive traction
- High energy injury: periosteal stripping, soft tissue devascularisation
- Local irradiation: radiotherapy impairs local vascularity
C. Treatment Factors
- Inadequate immobilisation: most important preventable cause of delayed union
- Excessive or rigid internal fixation: strips periosteum and disturbs the fracture haematoma (the scaffold for callus)
- Intact fellow bone: when one bone of the forearm or leg is unbroken, the fractured bone is splinted against union (e.g. isolated radius/fibula fracture)
- Poor reduction: malalignment and gap
- Inadequate treatment of delayed union: failure to maintain prolonged immobilisation allows delayed union to progress to non-union
CLASSIFICATION OF NON-UNION
By Biological Activity (Weber & Cech Classification)
| Type | Also Called | Radiographic Appearance | Biology |
|---|---|---|---|
| Hypertrophic | "Elephant foot" | Abundant callus, flared bone ends, no bridging | Biologically active (good vascularity), mechanically unstable |
| Oligotrophic | — | Minimal callus at bone ends | Intermediate activity |
| Atrophic | Avascular / avital | No callus, sclerotic/tapered bone ends with a gap | Biologically inactive, poor blood supply |
| Pseudoarthrosis (Synovial) | False joint | Synovial cavity between ends, smooth bone caps | Fibrocartilaginous synovium-lined cavity |
By Infection Status
- Aseptic (sterile) non-union
- Septic (infected) non-union — most challenging; requires elimination of infection before or alongside fixation
FRACTURE-SPECIFIC SITES PRONE TO NON-UNION
| Bone | Site | Reason |
|---|---|---|
| Femur | Neck (subcapital) | Intracapsular, disrupts retinacular vessels |
| Tibia | Lower 1/3 shaft | Poor soft tissue coverage, watershed blood supply |
| Scaphoid | Waist | Retrograde blood supply; proximal pole avascular |
| Talus | Neck | Tenuous vascular supply |
| Humerus | Shaft (mid) | Radial nerve and vasculature involvement |
| 5th Metatarsal | Proximal metaphyseal-diaphyseal junction (Jones fracture) | Watershed area |
| Clavicle | Mid-shaft | Especially with displacement |
CLINICAL FEATURES
Delayed Union
- Pain and tenderness over fracture site beyond expected healing time
- Abnormal mobility at fracture site
- No radiographic evidence of bridging callus at expected time
- X-ray: incomplete callus formation, visible fracture line, no sclerosis
Non-Union
- Persistent pain and tenderness at fracture site
- Abnormal mobility / false joint: painless or painful movement at fracture site
- Limb shortening (if bone ends resorb)
- Deformity
- Functional impairment
DIAGNOSIS
Clinical
- Pain on stressing the fracture site
- Palpable mobility at the fracture site
Radiological
Plain X-ray (cornerstone):
| Feature | Delayed Union | Non-Union |
|---|---|---|
| Fracture line | Visible, less clear | Clearly persistent |
| Callus | Present but incomplete | Minimal/absent (atrophic) or exuberant without bridging (hypertrophic) |
| Bone ends | No sclerosis | Sclerosis at bone ends (hallmark), rounded/tapered ends |
| Gap | May be present | Gap between bone ends (hallmark) |
CT Scan: Most accurate for assessing bridging; helpful when plain X-ray is inconclusive. Can detect occult callus and quantify bone contact.
MRI: Useful for detecting avascular necrosis (e.g. femoral head after neck fracture), bone oedema, infection, and soft tissue interposition.
Bone Scintigraphy (Technetium-99m):
- Nonunions show intense tracer uptake
- Synovial pseudoarthrosis: cold cleft between two hot areas
- 67Ga or 111In scans help identify infected non-unions
Laboratory Investigations (especially for infected non-union):
- WBC count, ESR, CRP, serum procalcitonin
- Wound/bone culture and sensitivity
TREATMENT
I. Treatment of Delayed Union
The key principle is optimise conditions to allow spontaneous healing:
- Prolonged immobilisation in a cast or splint — the most important step
- Correct the cause: treat infection, improve nutrition, stop NSAIDs/smoking
- Functional bracing (e.g. Sarmiento brace for tibial shaft) — compression during weight bearing stimulates osteoblastic activity
- Electrical stimulation: PEMF (Pulsed Electromagnetic Field) or capacitive coupling — stimulates angiogenesis and osteoid formation; useful adjunct in cooperative patients
- Low-intensity pulsed ultrasound (LIPUS): FDA-approved non-invasive adjunct
- If no progress → treat as non-union
II. Treatment of Non-Union
General Principles
- ABCS framework: Address Alignment, Biology, Compression, Stability
- Eliminate infection if present
- Correct nutritional/metabolic deficiencies
- Stop smoking; optimise diabetes control
A. Electrical Stimulation (Non-operative)
- Four modalities: direct current (implanted), PEMF, capacitive coupling, combined magnetic fields
- Effective for hypertrophic aseptic non-unions where alignment is acceptable
- Contraindicated in: atrophic non-union, pseudoarthrosis, active infection, severe comminution, failed prior grafting
- Over 400,000 non-unions treated with electrical stimulation globally
B. Bone Grafting (Cornerstone of Surgical Treatment)
Autogenous (autologous) bone graft — gold standard
- Source: iliac crest (most common), fibula, rib, tibia
- Provides: osteoconductivity (scaffold) + osteoinductivity (growth factors: BMP-2, BMP-7, TGF-β) + osteogenicity (living osteoblasts)
Types of bone graft:
| Type | Properties |
|---|---|
| Cancellous | Maximally osteogenic/inductive; rapid incorporation |
| Cortical | Structural support; slower incorporation |
| Corticocancellous | Both properties |
| Vascularised (free fibula) | Used for large defects (>6 cm) or infected/atrophic sites |
Bone graft substitutes:
- DBM (Demineralised Bone Matrix): osteoconductive + weakly osteoinductive
- BMP-2 and BMP-7 (rhBMP): recombinant growth factors; powerful osteoinductive stimulus
- Calcium phosphate / hydroxyapatite ceramics: osteoconductive scaffolds
- Platelet-Rich Plasma (PRP): growth factor concentrate
C. Internal Fixation
Principles:
- Debride/refresh bone ends (remove sclerotic bone, open medullary canal)
- Achieve rigid stability
- Supplement with bone graft (especially for atrophic non-unions)
Methods:
| Method | Indication |
|---|---|
| Intramedullary (IM) nail (with reaming) | Diaphyseal non-unions (tibia, femur, humerus); reaming releases endosteal growth factors and cells; dynamisation can compress non-union |
| Dynamic compression plate (DCP) / LCP | Periarticular non-unions; atrophic non-unions needing rigid stability + bone graft |
| Tension band wiring | Olecranon, patella |
Principles for Atrophic Non-Union:
- Excise avascular bone ends
- Open medullary canal
- Rigid fixation + mandatory bone graft
Principles for Hypertrophic Non-Union:
- Abundant biology already present; simply needs mechanical stability
- Rigid fixation (IM nail or plate) without necessarily grafting
- Often heals well once stability is provided
D. External Fixation
-
Ilizarov ring fixator / Circular fixator: powerful tool for complex non-unions
- Corrects deformity, compensates for bone loss via distraction osteogenesis
- Used for infected non-union, non-unions with malalignment, bone loss >2 cm
- Pin site care is mandatory
- Technique: corticotomy + bone transport to regenerate lost bone
-
Monolateral external fixator (e.g. Taylor Spatial Frame): computer-assisted deformity correction
E. Arthroplasty
- Reserved for periarticular non-unions in elderly with associated joint damage
- e.g. Hemiarthroplasty for femoral neck non-union; total elbow arthroplasty for distal humeral non-union
- Advantages: immediate weight bearing, treats co-existing arthritis
- Less favoured in young patients due to implant longevity concerns
F. Treatment of Infected Non-Union (Septic Non-Union)
The most challenging scenario. Principles:
- Eradicate infection first: aggressive debridement, sequestrum removal (sequestrectomy), dead space management
- Antibiotics: culture-guided systemic + local (antibiotic-impregnated beads or spacers)
- Stabilise the bone: external fixator preferred (avoids implant in infected field)
- Reconstruct: once infection controlled → bone graft + definitive fixation
- Soft tissue cover: flap reconstruction (e.g. free muscle flap) when required
The Papineau technique (open cancellous bone grafting) remains a reliable option for infected non-unions.
COMPLICATIONS OF NON-UNION (Untreated)
- Progressive deformity and malalignment
- Implant failure (plate breakage, screw pull-out)
- Pseudoarthrosis with chronic instability
- Chronic pain and disability
- Limb shortening
- Osteomyelitis (especially in open fractures)
SUMMARY TABLE
| Feature | Delayed Union | Non-Union |
|---|---|---|
| Definition | Slow healing, potential intact | No healing possible without intervention |
| Time criterion | >3 months | >6–8 months (arbitrary) |
| Bone ends (X-ray) | No sclerosis | Sclerosis present |
| Bone gap | May be absent | Usually present |
| Callus | Reduced | Absent (atrophic) or non-bridging |
| Treatment | Prolonged immobilisation, electrical stimulation | Surgery (fixation ± bone graft) |
RADIOLOGICAL IMAGES
Hypertrophic non-union (distal tibia, Ilizarov fixator):
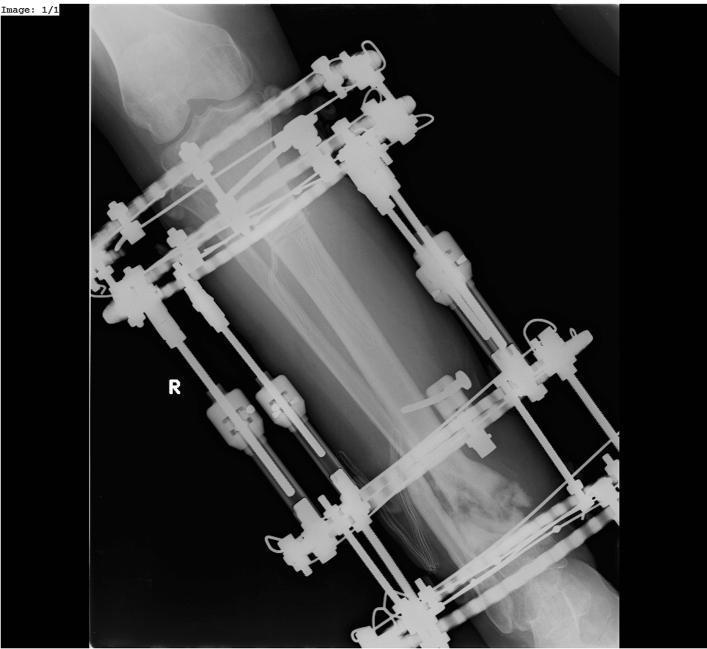 AP X-ray showing hypertrophic non-union of distal tibia: exuberant callus with persistent fracture line, stabilised with circular external fixator.
AP X-ray showing hypertrophic non-union of distal tibia: exuberant callus with persistent fracture line, stabilised with circular external fixator.
Atrophic non-union (clavicle):
 AP X-ray showing atrophic non-union of mid-shaft clavicle: bone ends tapered, rounded, sclerotic with a significant gap and no callus formation.
AP X-ray showing atrophic non-union of mid-shaft clavicle: bone ends tapered, rounded, sclerotic with a significant gap and no callus formation.
Hypertrophic non-union (humerus, IM nail):
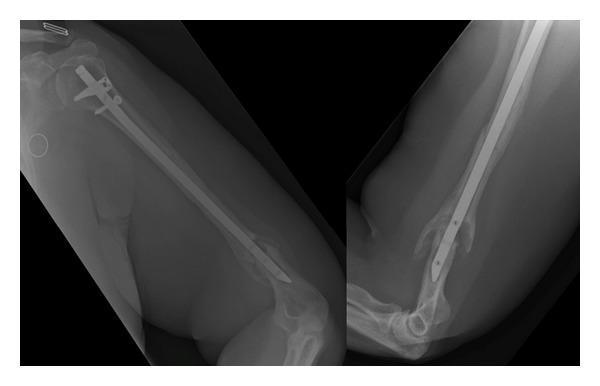 AP X-ray: hypertrophic non-union of distal humeral shaft after IM nailing. Exuberant periosteal callus with widened flared bone ends and a visible fracture line — indicating biological vitality but inadequate mechanical stability.
AP X-ray: hypertrophic non-union of distal humeral shaft after IM nailing. Exuberant periosteal callus with widened flared bone ends and a visible fracture line — indicating biological vitality but inadequate mechanical stability.
Sources: S Das: A Manual on Clinical Surgery, 13th ed. | Rockwood and Green's Fractures in Adults, 10th ed. (2025)
This is a shared conversation. Sign in to Orris to start your own chat.