Types of vagotomy wt r we cutting
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete breakdown of the types of vagotomy and exactly what is cut in each:
Types of Vagotomy - What We Are Cutting
Vagotomy is performed to reduce gastric acid secretion by interrupting the vagal nerve supply to the stomach. It is used in peptic ulcer disease (PUD), historically as elective surgery and now mostly in complications (bleeding, perforation, gastric outlet obstruction) refractory to medical therapy.
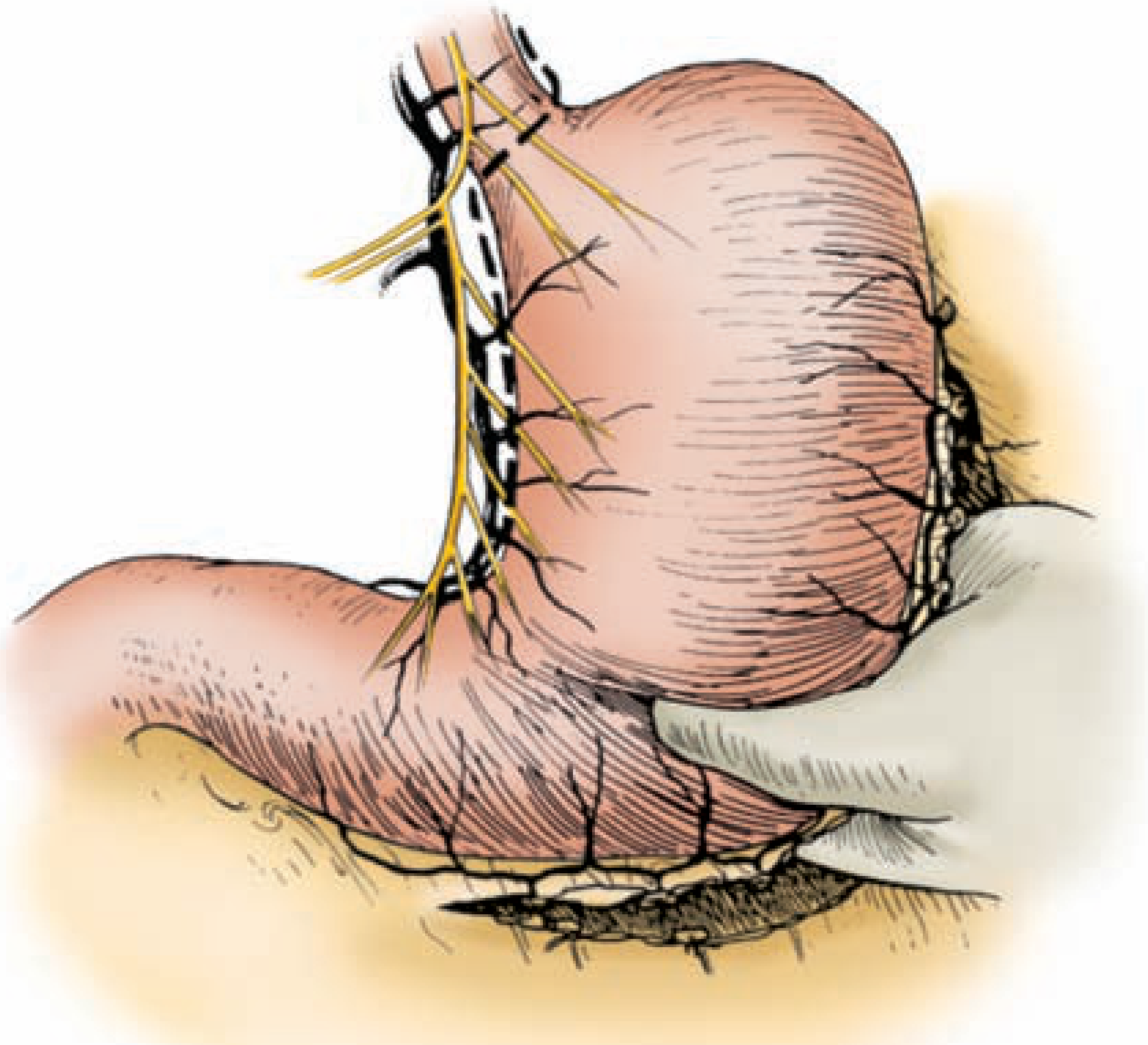
The Vagus Nerve Anatomy (Key to Understanding)
The vagus nerve runs as two trunks alongside the esophagus:
- Anterior vagal trunk (left vagus) - lies on the anterior surface of the esophagus
- Posterior vagal trunk (right vagus) - lies on the posterior surface
Each trunk gives off branches before reaching the stomach:
- Hepatic branches (from anterior trunk) - supply liver and gallbladder
- Celiac branches (from posterior trunk) - supply small bowel, pancreas, etc.
- Nerves of Latarjet (criminal nerve of Grassi) - run along the lesser curvature and supply the antrum/pylorus
The Three Main Types
1. Truncal Vagotomy (TV)
What is cut: Both the anterior AND posterior vagal trunks are divided at the level of the esophageal hiatus, ABOVE the origins of the hepatic and celiac branches.
Result: Complete, indiscriminate denervation of ALL abdominal viscera supplied by the vagus - stomach, liver, gallbladder, small intestine, pancreas, colon (up to splenic flexure).
Consequences:
- Eliminates antral peristalsis and pyloric coordination → gastric stasis
- Drainage procedure is MANDATORY (pyloroplasty or gastroenterostomy) to prevent gastric outlet obstruction
- Highest morbidity: dumping syndrome, diarrhea (from denervation of small bowel)
- Lowest recurrence rate
- Used in: emergency operations (bleeding/perforation), TV + antrectomy for refractory duodenal ulcer
2. Selective Vagotomy (SV)
What is cut: The vagal trunks are divided DISTAL to the origins of the hepatic and celiac branches, so only the gastric branches are divided.
Result: Complete gastric denervation (both fundus/body AND antrum), but hepatic, celiac, and other abdominal vagal branches are spared.
Consequences:
- Still denervates the antrum and pylorus → gastric emptying impaired
- Drainage procedure is still required
- Spares liver, gallbladder, small bowel, pancreas
- Clinical trials showed NO significant difference from truncal vagotomy in terms of dumping, diarrhea, or other side effects - so the added complexity did not translate to major benefit
- Intermediate in mortality/morbidity vs. truncal
3. Highly Selective Vagotomy (HSV)
(also called Parietal Cell Vagotomy / Proximal Gastric Vagotomy)
What is cut: Only the vagal fibers going to the acid-secreting parietal cells of the gastric body and fundus are divided. The nerves supplying the antrum, pylorus, and all other viscera are preserved.
Specifically, branches from the nerves of Latarjet to the proximal stomach (fundus/body) are cut, while:
- The terminal "crow's foot" of the nerve of Latarjet to the antrum is left intact
- The hepatic, celiac branches are left intact
- Innervation of the antrum/pylorus is preserved
Result: Selective denervation of only parietal cells that secrete HCl.
Consequences:
- Antral peristalsis and pyloric function are maintained → NO drainage procedure needed
- Lowest mortality and morbidity
- Highest recurrence rate (due to technical difficulty - incomplete denervation is common)
- Abolishes receptive relaxation (as do all types)
- Procedure of choice when elective vagotomy is indicated
Summary Table
| Type | What is Cut | Level of Cut | Drainage Needed? | Recurrence | Side Effects |
|---|---|---|---|---|---|
| Truncal | Both vagal trunks | Above hepatic + celiac branches (at esophageal hiatus) | Yes (mandatory) | Lowest | Highest (dumping, diarrhea) |
| Selective | Gastric vagal trunks only | Below hepatic + celiac branches | Yes (still needed) | Intermediate | Similar to truncal |
| Highly Selective (HSV) | Only parietal cell branches | Individual branches to fundus/body only; antrum spared | No | Highest | Lowest |
Key Point on All Three Types
All three types abolish receptive relaxation and gastric accommodation (relaxation of the gastric fundus in response to food). This is because the vagal fibers mediating this reflex run to the proximal stomach - which is denervated in every type.
The key differentiator is how much else you sacrifice: truncal cuts everything, selective spares the hepatic/celiac branches, and highly selective spares everything except the parietal cell branches.
Sources: Fischer's Mastery of Surgery 8th ed., p. 2904; Maingot's Abdominal Operations, Chapter 26
This is a shared conversation. Sign in to Orris to start your own chat.