Varicose vein
Reading File
Finding Sources
Searching PubMed
"varicose veins"[MeSH Terms] AND treatment
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information. Let me compile a thorough response.
Varicose Veins
Definition
Varicose veins are abnormally dilated, tortuous, elongated superficial veins of the lower limb resulting from valvular incompetence and venous hypertension. The term comes from the Latin varix (twisted vein). They occur almost exclusively in humans, likely related to the upright posture.
Anatomy and Venous System
The superficial venous system of the lower limb consists of:
- Great saphenous vein (GSV) - the longest vein in the body, runs medially from the foot to the saphenofemoral junction (SFJ) in the groin
- Small saphenous vein (SSV) - runs posterolaterally from the foot to the saphenopopliteal junction behind the knee
- Anterior accessory great saphenous vein (AAGSV)
- Perforating (communicating) veins - connect the superficial to deep systems; normally allow blood to flow from superficial to deep
Epidemiology
- Affects ~30% of the adult population
- Women are affected more commonly (ratio ~10:1 in some series)
- Middle-aged individuals are the usual sufferers, though any age group can be affected
- Less common in primitive civilizations (Africa, Far East)
Aetiology / Pathophysiology
The fundamental defect is valvular incompetence, allowing retrograde (downward) flow with gravity (reflux). It is no longer thought to be caused solely by primary mechanical valve failure.
Vein wall changes include:
- Inflammatory cell infiltration and activation
- Dysfunctional smooth muscle cell proliferation
- Collagen deposition and decreased elastin content
- Increased matrix metalloproteinases
- Loss of compliance, dilatation, and elongation causing tortuosity
- Secondary valvular dysfunction
Predisposing factors:
- Prolonged standing (conductors, police, tram drivers)
- Pregnancy - hormonal (progesterone) and mechanical uterine compression
- Obesity
- Positive family history (strong genetic component)
- Previous deep vein thrombosis (DVT) - post-thrombotic veins
- Pelvic tumours (fibroid, ovarian cyst, colorectal cancer) causing venous obstruction
- Congenital arteriovenous fistula (in younger patients)
- May-Thurner syndrome (iliac vein compression)
Classification:
- Primary varicose veins - intrinsic valve/wall defect
- Secondary varicose veins - due to an identifiable cause (post-thrombotic, pelvic obstruction, AV fistula)
CEAP Classification
The standard clinical classification for chronic venous disease:
| Class | Features |
|---|---|
| C0 | No visible or palpable signs |
| C1 | Telangiectasias / reticular veins |
| C2 | Varicose veins |
| C3 | Oedema |
| C4a | Pigmentation / eczema |
| C4b | Lipodermatosclerosis / atrophie blanche |
| C5 | Healed venous ulcer |
| C6 | Active venous ulcer |
Symptoms
- Aching pain in the leg, worse towards end of day, worse with prolonged standing, relieved by elevation
- Night cramps
- Ankle swelling (oedema) towards the end of the day
- Itching (venous eczema)
- Skin discolouration (haemosiderin pigmentation)
- Heaviness / fatigue in the legs
- Bursting pain on walking - suggests underlying deep vein thrombosis
Note: Symptoms do not always correlate with the size of varicosities - severely symptomatic patients may have few visible veins and vice versa. - S Das, p.105
Clinical Examination
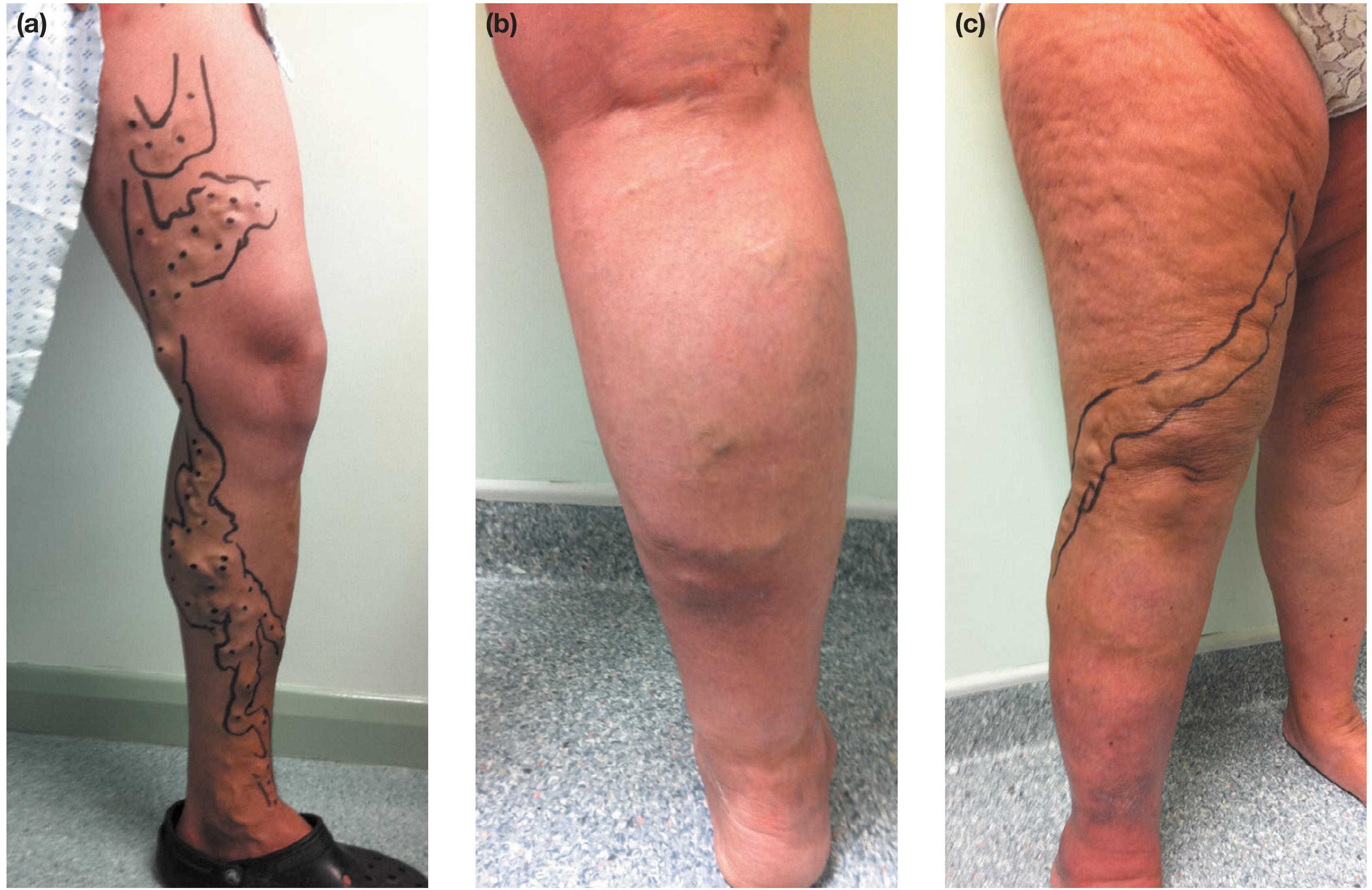
Inspection (patient standing)
- Distribution of varicosities guides source:
- Medial thigh and calf → GSV incompetence
- Posterolateral calf → SSV incompetence
- Anterolateral thigh/calf → AAGSV incompetence
- Skin changes: pigmentation, eczema, lipodermatosclerosis, ulceration
- Saphena varix - dilated SFJ presenting as a painless groin lump; disappears supine; impulse on coughing; can mimic inguinal hernia
Special Tests (Classical - mainly historical now)
| Test | Method | Significance |
|---|---|---|
| Trendelenburg test | Leg elevated, tourniquet applied at groin, patient stands - veins fill from below | Identifies SFJ incompetence |
| Multiple tourniquet test | Multiple tourniquets at different levels | Locates incompetent perforators |
| Schwartz test (Percussion) | Tap vein at one point, impulse felt at another | Incompetent valves between fingers |
| Morrissey cough impulse test | Leg elevated then patient coughs; impulse felt at saphenous opening | SFJ incompetence |
| Fegan's method | Palpate gaps in deep fascia along varicose line | Locates incompetent perforators |
| Perthes test | Tourniquet above knee while patient exercises | Assesses deep vein patency |
Abdominal Examination
Always examine the abdomen for secondary causes - pregnant uterus, fibroid, ovarian cyst, colorectal tumour - S Das, p.108.
Investigations
Duplex ultrasound scanning is the gold standard investigation and has replaced all handheld Doppler and tourniquet tests. It should be performed on all patients prior to intervention. - Bailey and Love, p.1052
Duplex aims to establish:
- Presence of reflux in deep and superficial systems
- Exact distribution and extent of reflux including affected junctions and perforators
- Presence of deep vein obstruction
- Suitability of incompetent veins for treatment (diameter, tortuosity, depth)
- Identification of re-entrant perforators
A 7.5-13 MHz linear transducer is used. The 'Mickey Mouse' sign (transverse view at groin) identifies the GSV and common femoral vein medial to the artery. The 'saphenous eye' sign is the transverse view of the GSV within its fascial compartment.
Complications
Chronic complications:
- Venous eczema (varicose eczema)
- Lipodermatosclerosis
- Haemosiderin pigmentation
- Atrophie blanche
- Venous (varicose) ulcer - classically at the medial malleolus ("gaiter area")
Acute complications:
- Superficial vein thrombosis (thrombophlebitis) - painful, indurated cord; rarely causes pulmonary embolism (thrombus firmly attached to wall)
- Bleeding - varicose vein rupture (can be severe; treat with leg elevation and direct pressure)
Treatment
Conservative (Non-Interventional)
- Compression hosiery (graduated stockings)
- Lifestyle advice: weight loss, avoid prolonged standing, leg elevation
- Emollients for skin care
Interventional Options
1. Endovenous Laser Ablation (EVLA)
- A laser fibre is introduced into the vein under ultrasound guidance
- Thermal energy (around 60-80 J/cm) is delivered to ablate the vein wall under tumescent anaesthesia
- No consensus on optimal power or pullback speed
- Good evidence of durable closure
- Performed as a day-case procedure
2. Radiofrequency Ablation (RFA)
- Same principle as EVLA but uses electromagnetic current
- Most popular device: ClosureFast™ (Medtronic) - reaches 120°C for 20-second treatment cycles, coil withdrawn in steps
- Available in 3 cm and 7 cm coil lengths
EVLA vs RFA: Evidence is generally equivocal. Both have very high 5-year closure rates. Choice often comes down to operator preference. Both are superior to conventional surgery in terms of recovery time, complications, and patient satisfaction. - Bailey and Love, p.1055
A 2024 meta-analysis (Jiang et al., J Vasc Surg Venous Lymphat Disord) compared radiofrequency ablation vs laser ablation and confirmed broadly equivalent outcomes with minor differences in technique-specific complications.
3. Ultrasound-Guided Foam Sclerotherapy (UGFS)
- A sclerosant (e.g., sodium tetradecyl sulphate, polidocanol) is mixed with gas to create foam
- Foam is injected under duplex guidance into the incompetent vein
- Less durable than thermal ablation but useful for tortuous veins, residual disease, and patients unsuitable for thermal treatment
- Can be repeated
4. Mechanical/Chemical Ablation (MOCA) and Cyanoacrylate Glue
- Newer non-thermal, non-tumescent techniques
- ClariVein (MOCA) - rotating wire tip plus liquid sclerosant
- VenaSeal - medical-grade cyanoacrylate glue injected to seal the vein
- Advantages: no tumescent anaesthesia needed, faster recovery, no nerve injury from heat
5. Conventional Surgery (now largely replaced)
- High ligation and stripping - ligation of the SFJ + stripping of the GSV
- Stab (ambulatory) phlebectomy - micro-incisions to remove varicosities (often combined with endovenous procedures)
- CPT codes: 37700 (ligation/division of GSV at SFJ), 37765-37766 (stab phlebectomy)
- Higher morbidity, longer recovery; reserved for when endovenous techniques are not suitable
Treatment for Recurrent Varicose Veins
A 2024 systematic review and meta-analysis (Bontinis et al., Int Angiol) examined interventions for recurrent varicose veins from SFJ/GSV and found endovenous techniques to be effective, though evidence for recurrent disease is less robust than for primary disease.
Management Summary
| Situation | Preferred Approach |
|---|---|
| Primary GSV/SSV incompetence | Endovenous thermal ablation (EVLA or RFA) ± phlebectomy |
| Tortuous/small veins | Foam sclerotherapy |
| Telangiectasias | Liquid sclerotherapy / laser |
| Unsuitable for endovenous | Surgery (high ligation + stripping) |
| Recurrent disease | UGFS or re-do endovenous/surgery |
| Post-DVT secondary varicosities | Conservative/compression (treat underlying disease first) |
Key Points
- Varicose veins affect ~30% of adults; female predominance
- Primary mechanism: valvular incompetence → reflux → venous hypertension
- GSV system is affected in ~60% of cases; SSV in ~20%
- Duplex ultrasound is mandatory before any intervention
- Endovenous techniques (EVLA, RFA) are the current standard of care - superior to open surgery
- EVLA and RFA have equivalent outcomes; choice is operator preference
- Compression hosiery is effective for symptom management but does not cure varicose veins
- Always exclude secondary causes (DVT, pelvic mass) before treating
Sources: Bailey and Love's Short Practice of Surgery, 28th Ed., pp.1049-1060; S Das Manual on Clinical Surgery, 13th Ed., pp.105-111; Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.