Significance of JVP measurement
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Here is a comprehensive account of the significance of JVP measurement, drawn from Harrison's Principles of Internal Medicine (22nd ed.) and Braunwald's Heart Disease.
Jugular Venous Pressure (JVP) — Clinical Significance
Why JVP Matters
The JVP is the single most important bedside measurement for estimating a patient's volume status and right-sided cardiac filling pressure. It provides an indirect, non-invasive estimate of central venous pressure (CVP) / right atrial pressure and reflects the hemodynamic state of the heart.
The internal jugular vein is preferred over the external jugular vein because the external jugular is valved and not directly in line with the superior vena cava and right atrium.
How to Measure JVP
- Patient positioned semi-recumbent, typically at 30–45°
- Measure the vertical distance from the top of the jugular venous pulsation to the sternal angle (angle of Louis)
- Normal: ≤4.5 cm above the sternal angle at 30° elevation
- A >4.5 cm distance is considered abnormal (elevated CVP)
- The sternal angle reference tends to systematically underestimate CVP; the clavicle may be a more reliable landmark — venous pulsations above the clavicle in the sitting position are clearly abnormal (>10 cm from RA)
- Bedside estimates are in cmH₂O; convert to mmHg: 1 mmHg = 1.36 cmH₂O
The JVP Waveform and Its Components
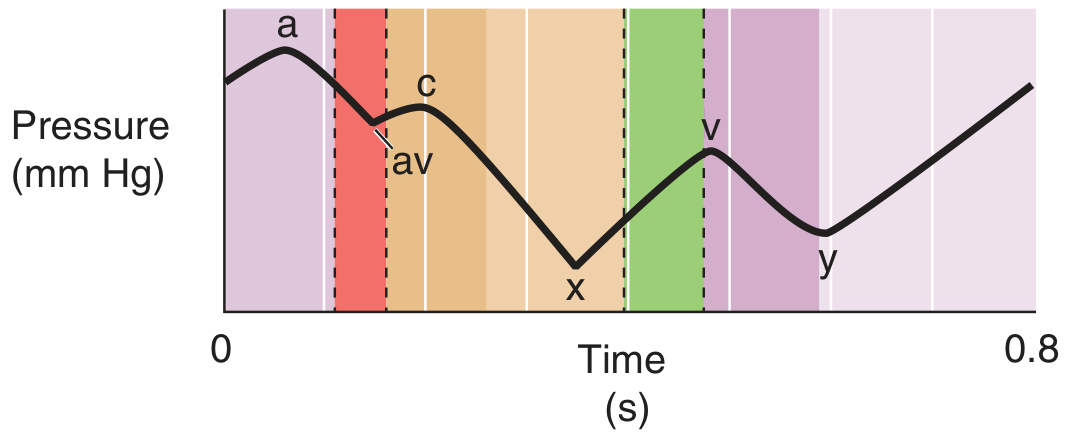
| Component | Physiological Basis | Clinical Significance |
|---|---|---|
| a wave | Right atrial presystolic contraction; just after P wave on ECG, before S1 | Prominent a wave → reduced RV compliance; Cannon a wave → AV dissociation (RA contracts against closed tricuspid valve); Absent a wave → atrial fibrillation |
| c wave | Tricuspid valve pushed into RA during early ventricular systole | Small, often merged with a or x; may also reflect carotid pulsation artifact |
| x descent | Fall in RA pressure after tricuspid valve opening; atrial relaxation | Exaggerated in cardiac tamponade |
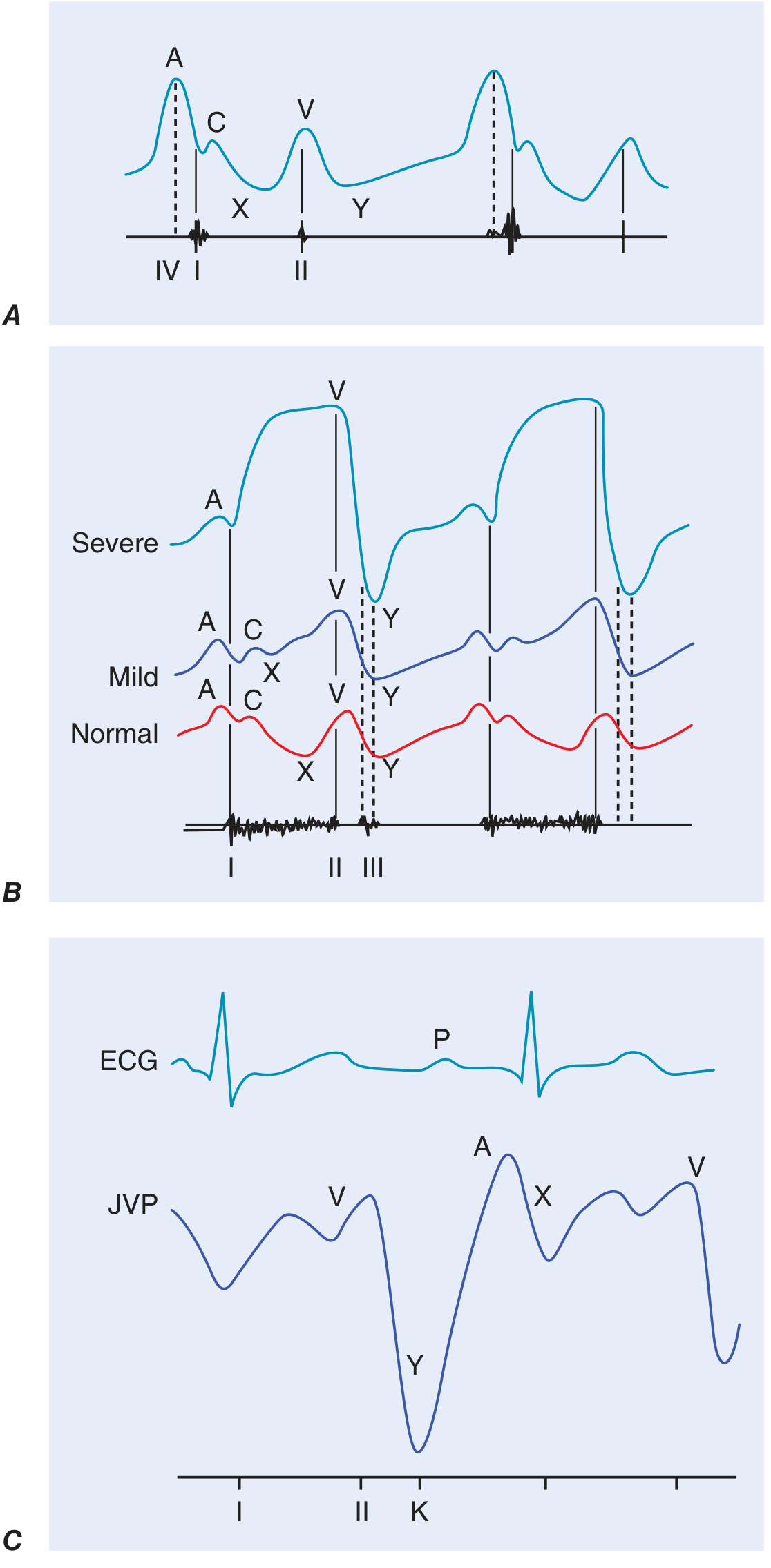
| v wave | Atrial filling during ventricular systole (passive RA filling) | Accentuated in tricuspid regurgitation (TR); with severe TR, v wave merges with c wave — waveform becomes "ventricularized" |
| y descent | Fall in RA pressure after tricuspid valve opening | Rapid y descent → constrictive pericarditis (corresponds to pericardial knock); Blunted/slow y descent → tricuspid stenosis or cardiac tamponade |
JVP vs. carotid pulse distinction: The venous waveform is normally biphasic (in sinus rhythm); the carotid is monophasic. Venous pulsation is obliterated by light pressure; arterial is not. JVP changes with posture and inspiration.
Clinical Significance of JVP Level
Elevated JVP
Indicates raised right atrial pressure / venous hypertension. Key causes:
| Condition | JVP Pattern |
|---|---|
| Right heart failure / biventricular heart failure | Elevated JVP ± peripheral edema |
| Constrictive pericarditis | Elevated JVP + Kussmaul's sign + rapid y descent + pericardial knock |
| Cardiac tamponade | Elevated JVP, blunted y descent, paradoxical pulse |
| Tricuspid stenosis | Elevated JVP, slow y descent, prominent a wave |
| Tricuspid regurgitation | Prominent/giant v wave, ventricularized waveform |
| Superior vena cava obstruction | Elevated JVP without pulsation |
| Pulmonary hypertension/PE | Elevated JVP, prominent a wave |
| RV infarction | Elevated JVP with hypotension |
Prognostic Value
- In patients with heart failure, a right atrial pressure >10 mmHg (estimated at bedside) has an 88% positive predictive value for a pulmonary artery wedge pressure >22 mmHg.
- Elevated JVP is associated with a higher risk of hospitalization for heart failure, death from heart failure, or both — in patients with both symptomatic HF and asymptomatic LV systolic dysfunction.
Edema Interpretation
- Elevated JVP + lower extremity edema = volume overload (suggests CHF, constrictive pericarditis)
- Edema without elevated JVP = hypoalbuminemia (nephrotic syndrome, liver failure), venous insufficiency, lymphedema, or calcium channel blocker use
Dynamic Maneuvers
Abdominojugular (Hepatojugular) Reflux
- Firm sustained pressure over the right upper quadrant for >15 seconds
- Positive response: sustained rise of >3 cm in JVP
- Confirms volume-overloaded state with limited venous compliance
- Predicts a pulmonary artery wedge pressure >15 mmHg in heart failure patients
Kussmaul's Sign
- Definition: Rise or failure of JVP to fall with inspiration (normal JVP falls with inspiration due to decreased intrathoracic pressure)
- Classically associated with constrictive pericarditis
- Also seen in: restrictive cardiomyopathy, massive pulmonary embolism, RV infarction, advanced LV systolic heart failure, and post-cardiac surgery patients
Passive Leg Elevation
- Raising the legs shifts venous blood centrally; a positive response (rise in JVP) suggests limited venous compliance and volume overload
Summary of JVP Significance
| Domain | Significance |
|---|---|
| Volume status | Primary non-invasive bedside marker of central venous pressure |
| RV filling pressure | Reflects right atrial and RV end-diastolic pressure |
| LV filling (indirectly) | Predictable relationship with pulmonary wedge pressure in HF |
| Waveform morphology | Diagnoses specific conditions (TR, tamponade, constriction, AV dissociation) |
| Prognosis | Elevated JVP predicts HF hospitalization and mortality |
| Dynamic tests | Abdominojugular reflux and Kussmaul's sign extend diagnostic value |
Sources: Harrison's Principles of Internal Medicine, 22nd ed. (2025), Chapter 246; Braunwald's Heart Disease, 12th ed., Chapter 13 & 48
JVP wave forms
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.