Hi
Hi there! How can I help you today?

1000077112.jpg
Explain this embryology
Reading File
analyse_media
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Here is a full explanation of the model shown in your image:
Transposition of the Great Vessels (TGV)
What the Model Shows
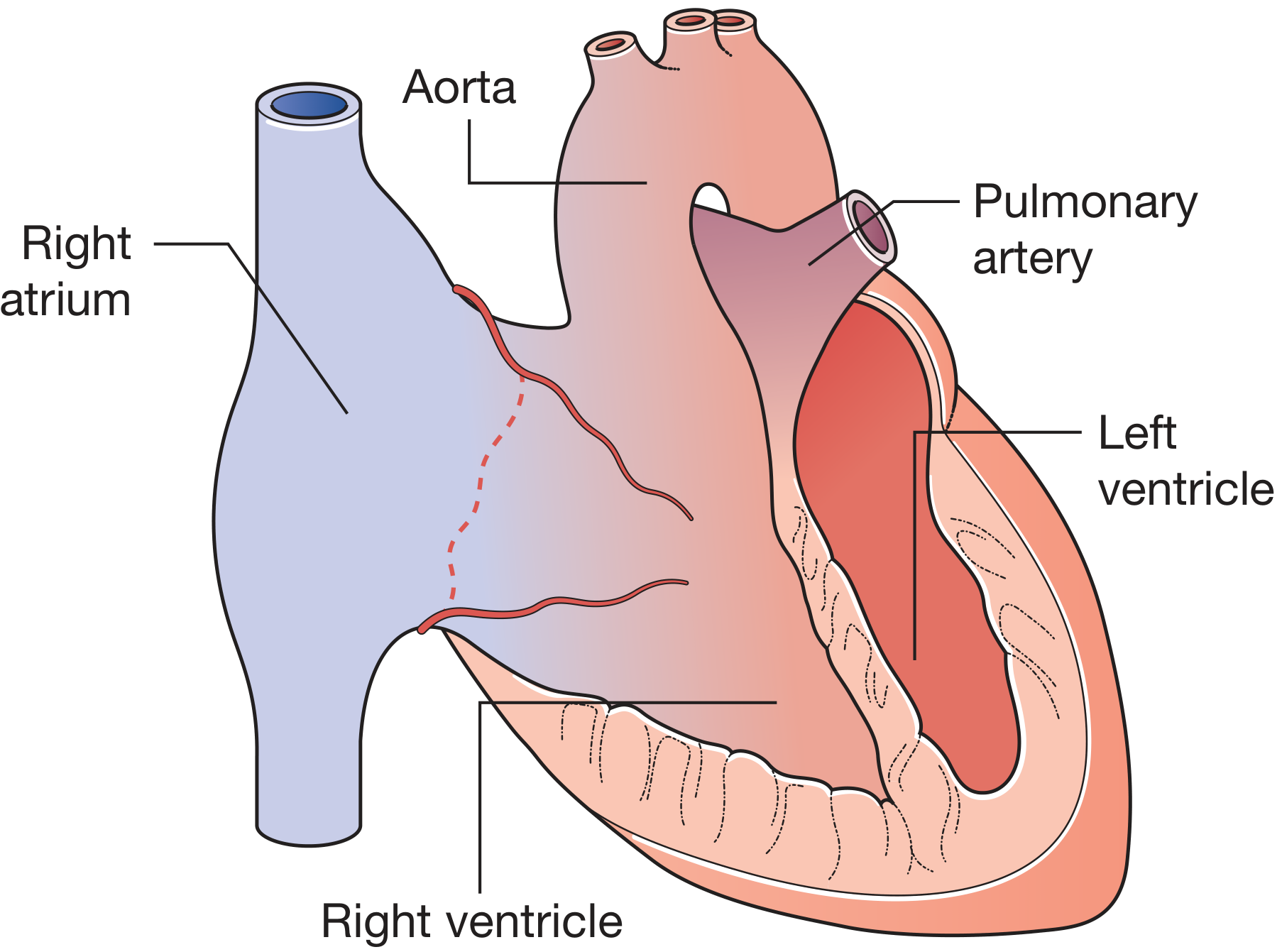
The physical model on the board depicts a heart in which the two great arteries have switched their origins:
- Blue structure (Aorta) arises from the right ventricle - carrying deoxygenated blood to the body
- Red structure (Pulmonary artery) arises from the left ventricle - carrying oxygenated blood back to the lungs
- A small connecting vessel between the two (Patent Ductus Arteriosus / PDA) is visible, allowing minimal blood mixing
Normal Embryology (What Should Happen)
In normal heart development, the truncus arteriosus (a single outflow tube) is divided into the aorta and pulmonary trunk by a spiral partition called the aorticopulmonary (conotruncal) septum. This septum grows in a helical/spiral pattern, which causes the aorta to "cross over" and end up connected to the left ventricle, and the pulmonary artery to connect to the right ventricle.
What Goes Wrong in TGV
TGV results from failure of the conotruncal septum to spiral. Instead of forming in a helix, the septum grows in a straight line, so:
- The aorta stays anterior and connects to the right ventricle (instead of crossing over to the left)
- The pulmonary artery stays posterior and connects to the left ventricle
This is a conotruncal defect - a developmental error involving the bulbus cordis and truncus arteriosus (weeks 5-8 of embryogenesis). Neural crest cells play a critical role in conotruncal septation; abnormal neural crest cell migration is considered a key underlying mechanism.
Why It's Incompatible with Life
The two circulations now run in parallel instead of in series:
| Circuit | What happens |
|---|---|
| Systemic (body) | Deoxygenated blood: Right atrium → Right ventricle → Aorta → Body → back to right side |
| Pulmonary (lungs) | Oxygenated blood: Left atrium → Left ventricle → Pulmonary artery → Lungs → back to left side |
Oxygenated blood never reaches the body. Survival depends entirely on mixing via shunts:
- Patent Foramen Ovale (PFO)
- Ventricular Septal Defect (VSD)
- Patent Ductus Arteriosus (PDA) - shown in the model
Clinical Features
- Most common cause of cyanotic congenital heart disease presenting in the newborn period
- Severe central cyanosis within 24-48 hours of birth
- Chest X-ray shows the classic "egg on its side" appearance (narrow mediastinal pedicle due to aorta lying directly in front of pulmonary artery)
- Echocardiography confirms diagnosis
Management
- Immediate: IV prostaglandin E1 to keep the PDA open; balloon atrial septostomy (Rashkind procedure) to increase mixing
- Definitive: Arterial switch operation (Jatene procedure) - performed within the first 2 weeks of life. Both great arteries are transected and re-anastomosed to the correct ventricles. Long-term outcomes are excellent.
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 987
This is a shared conversation. Sign in to Orris to start your own chat.