Explain me neurophysiology of urinary bladder
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
I now have everything needed for a comprehensive answer. Let me compile the full neurophysiology explanation.
Neurophysiology of the Urinary Bladder
The bladder has one fundamental job: store urine at low pressure, then expel it completely and voluntarily. Achieving this requires a sophisticated three-tier neural control system - peripheral nerves, spinal cord reflexes, and supraspinal (brain) centers - all working in coordination.
1. Anatomy of Innervation
The lower urinary tract (LUT) receives three sets of nerves:
| Nerve | Origin | Type | Function |
|---|---|---|---|
| Pelvic nerve | S2-S4 | Parasympathetic | Detrusor contraction, urethral relaxation (voiding) |
| Hypogastric nerve | T10-L2 | Sympathetic | Detrusor relaxation, bladder neck contraction (storage) |
| Pudendal nerve | S2-S4 (Onuf's nucleus) | Somatic | External urethral sphincter contraction (voluntary continence) |
Parasympathetic Pathway
Preganglionic neurons originate in the sacral parasympathetic nucleus (SPN) at S2-S4. Their axons pass through the pelvic nerve and synapse in the pelvic plexus, on vesical ganglia, or within intramural ganglia of the bladder wall. Postganglionic neurons release acetylcholine acting on muscarinic (M2/M3) receptors on the detrusor, causing contraction. Ganglionic transmission itself is via acetylcholine on nicotinic receptors. There is also a small NANC (non-adrenergic, non-cholinergic) component mediated by ATP acting on purinergic receptors. The pelvic nerve also carries parasympathetic fibers to the urethra, where they release nitric oxide to cause smooth muscle relaxation during voiding. - Smith and Tanagho's General Urology, 19th Ed.
Sympathetic Pathway
Preganglionic neurons arise in the intermediolateral nuclei of T10-L2. Axons travel via splanchnic nerves to the inferior mesenteric ganglia, then through the hypogastric nerve (or via the paravertebral chain into the pelvic nerve) to reach the bladder. Postganglionic neurons release noradrenaline:
- Beta-3 (β3) adrenoceptors on the detrusor → relaxation (enabling filling)
- Alpha-1 (α1) adrenoceptors on the bladder neck and urethra → contraction (maintaining continence)
The sympathetic pathway also inhibits parasympathetic ganglionic transmission at the ganglionic level, reinforcing the storage state. - Smith and Tanagho's General Urology, 19th Ed.
Somatic Pathway
The external urethral sphincter (rhabdosphincter) is skeletal muscle innervated by motor neurons in Onuf's nucleus (S2-S4) via the pudendal nerve. Acetylcholine acts on nicotinic receptors. This pathway is tonically active during storage and under voluntary control. - Costanzo Physiology, 7th Ed.
2. Afferent Pathways (Sensory)
Two main afferent fiber types carry information from the bladder wall to the spinal cord:
- Aδ fibers (myelinated): Respond to bladder distension and wall tension during normal filling. These are the primary afferents of the normal adult micturition reflex. They travel in the pelvic nerve to the sacral cord and ascend to the brain.
- C-fibers (unmyelinated): Normally "silent" mechanoreceptors, activated mainly by noxious stimuli (chemical irritants, inflammation, very cold saline - the "ice-water test"). After spinal cord injury, C-fibers become the dominant afferents mediating a hyperactive vesicospinovesical reflex. - Smith and Tanagho's General Urology, 19th Ed.
The urothelium (bladder lining) also plays a signaling role - it releases ATP and acetylcholine in response to stretch, which activates submucosal afferent nerve endings and contributes to the sensation of fullness.
3. The Cystometrogram: Bladder Compliance
The cystometrogram (CMG) below shows how intravesical pressure changes with filling volume:
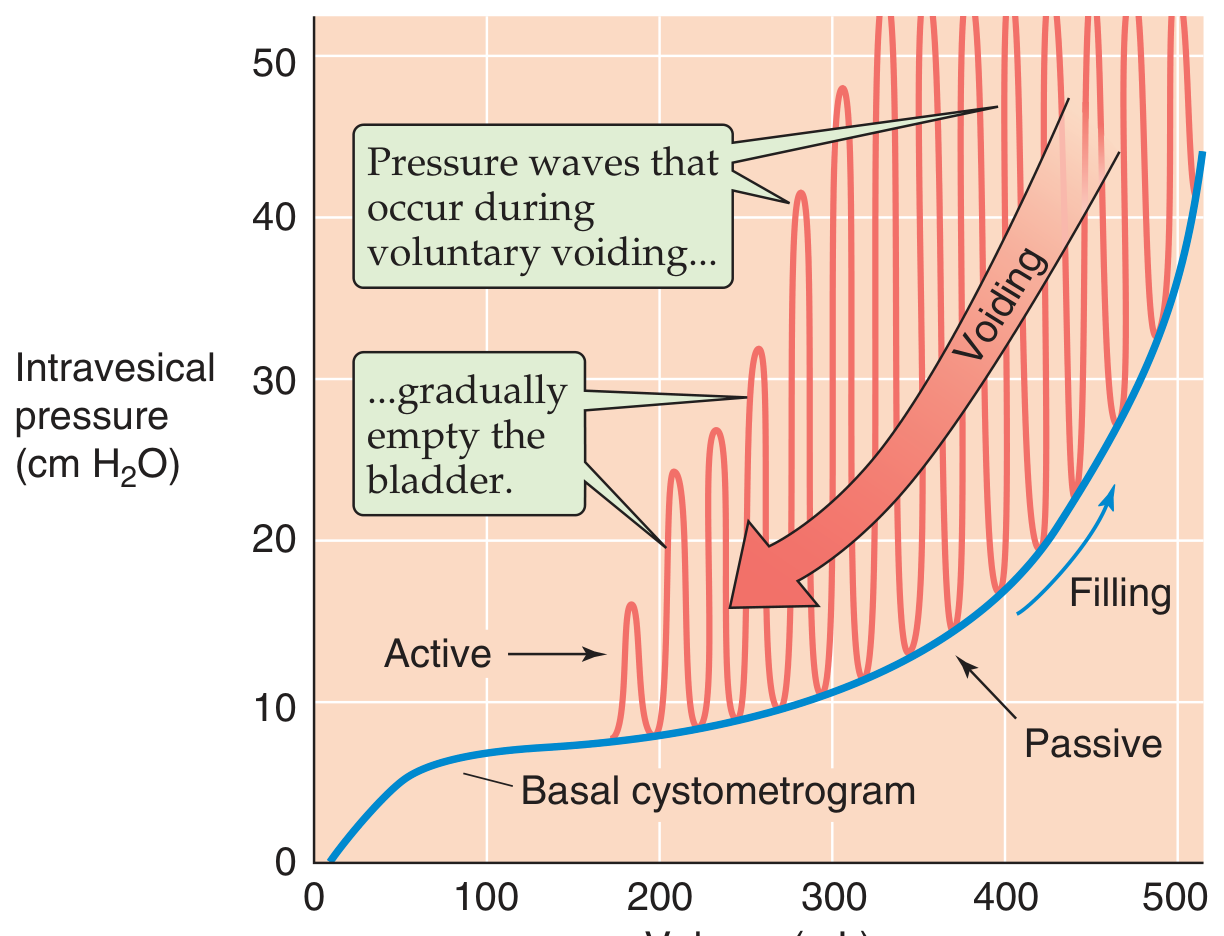
- 0-50 mL: Moderate pressure rise
- 50-300 mL: Near-flat (high compliance) due to smooth muscle relaxation - this is passive viscoelastic behavior, independent of extrinsic innervation
- >400 mL: Steep passive pressure rise
- First urge to void: ~150 mL
- Sensation of fullness: ~400-500 mL
Active pressure waves (the oscillations shown in pink) represent voluntary voiding contractions. - Medical Physiology (Boron & Boulpaep)
4. Spinal Cord Integration
Storage Reflexes (two pathways)
a. Sympathetic storage reflex (vesicospinovesical)
- Bladder distension → Aδ afferents in pelvic nerve → sacral cord → ascend to lumbar cord → sympathetic efferents (T10-L2) activate
- Result: β3-mediated detrusor relaxation + α1-mediated bladder neck contraction + inhibition of parasympathetic ganglia
- This keeps the bladder in fill mode at low pressure. - Smith and Tanagho's General Urology, 19th Ed.
b. Somatic storage reflex (guarding/continence reflex)
- Sudden rise in abdominal pressure (cough, sneeze) → Aδ afferents → sacral cord → Onuf's nucleus → pudendal nerve → rhabdosphincter contracts
- This reflex is tonically active during storage and dynamically activated during stress. - Smith and Tanagho's General Urology, 19th Ed.
Voiding Reflex (vesicobulbovesical pathway)
- When afferent input exceeds a threshold → ascending spinal tract neurons relay to the periaqueductal gray (PAG) → PMC activates → descending pathways simultaneously:
- Excite sacral parasympathetics → detrusor contraction
- Inhibit Onuf's nucleus → sphincter relaxation (detrusor-sphincter synergy)
5. Supraspinal Control - The Brain's Role
Pontine Micturition Center (PMC / Barrington's nucleus / M-region)
The PMC is the key "on/off switch" for voiding. It coordinates:
- Descending excitation to sacral parasympathetics (detrusor contraction)
- Descending inhibition to Onuf's nucleus (sphincter relaxation)
This ensures detrusor-sphincter synergy - the bladder contracts as the sphincter relaxes, which is critical for complete, efficient voiding. Without intact pontine-sacral connectivity (as in spinal cord injury), this coordination breaks down, producing detrusor-sphincter dyssynergia. - Bradley and Daroff's Neurology in Clinical Practice
A separate Pontine Storage Center (L-region) has been identified in animal studies, acting via PAG and Onuf's nucleus to maintain sphincter tone during storage.
Periaqueductal Gray (PAG)
The PAG acts as a relay and integration hub:
- Receives ascending afferents from the bladder (sensing fullness)
- Receives descending input from the cortex and hypothalamus (social appropriateness, anxiety, voluntary control)
- Integrates these signals and, at threshold, releases tonic inhibition of the PMC → voiding begins
Cortical and Higher Centers
Functional neuroimaging (PET/fMRI) has identified several key cortical regions:
- Medial prefrontal cortex: Evaluates social appropriateness of voiding; tonic inhibition of PMC during the filling phase
- Anterior cingulate gyrus: Active during voiding, involved in attentional/motivational aspects
- Right inferior frontal gyrus: Active during voiding
- Hypothalamus: Influences PMC via PAG; emotional and autonomic modulation
- Cerebellum: Active during voiding (coordination of pelvic floor muscles)
In healthy adults, cortical centers maintain tonic inhibition of the micturition reflex until a conscious decision to void is made. This explains why infants void reflexively, while adults can suppress the urge voluntarily. Supraspinal injury (stroke, frontal lobe disease) removes this inhibition, leading to detrusor overactivity (OAB). - Bradley and Daroff's Neurology in Clinical Practice
6. The Micturition Reflex - Step by Step
| Phase | What happens |
|---|---|
| Filling | Bladder fills; Aδ afferents fire at low frequency → sympathetic storage reflex active → detrusor relaxed, sphincters contracted; cortex inhibits PMC |
| Urge sensation | ~150 mL; afferent signals reach PAG and cortex; first conscious awareness |
| Threshold reached | ~400-500 mL; PAG integrates cortical/subcortical "permission to void" → releases PMC inhibition |
| Voiding initiation | Voluntary relaxation of external sphincter → urine enters proximal urethra → urethral afferents reinforce the reflex |
| Active voiding | PMC activates sacral parasympathetics → detrusor contraction; PMC inhibits Onuf's nucleus → sphincter relaxation; sympathetic pathway inhibited supraspinally |
| Completion | Detrusor relaxes; sphincters close; storage phase resumes |
7. Key Neurotransmitters Summary
| Pathway | Neurotransmitter | Receptor | Effect |
|---|---|---|---|
| Parasympathetic (postganglionic) | Acetylcholine | M2/M3 (muscarinic) | Detrusor contraction |
| Sympathetic (postganglionic) | Noradrenaline | β3 (detrusor) | Relaxation |
| Sympathetic (postganglionic) | Noradrenaline | α1 (bladder neck) | Contraction |
| Somatic (pudendal) | Acetylcholine | Nicotinic | Sphincter contraction |
| Urothelium | ATP | P2X3 (afferents) | Afferent activation |
| PMC interneurons | GABA | GABA-A/B | Inhibit micturition reflex |
| Urethral smooth muscle (para) | Nitric oxide | sGC | Relaxation during voiding |
8. Effects of Neural Lesions
| Lesion Site | Immediate Effect | Chronic Effect |
|---|---|---|
| Complete spinal cord injury above lumbosacral level | Areflexic bladder, urinary retention | Vesicospinovesical reflex via C-fibers; detrusor-sphincter dyssynergia |
| Sacral dorsal roots (afferents only) | Reflex contractions abolished | Atonic, distended bladder with residual urine |
| Both afferent and efferent sacral nerves | Flaccid, distended bladder | Small uncoordinated contractions; persistent residual urine |
| Supraspinal/cortical lesion (e.g., stroke) | Loss of voluntary inhibition | Detrusor overactivity, urgency incontinence (OAB) |
Sources: Medical Physiology (Boron & Boulpaep), Smith and Tanagho's General Urology 19th Ed., Costanzo Physiology 7th Ed., Bradley and Daroff's Neurology in Clinical Practice
Key clinical takeaway: The bladder is under 98% of its life in storage mode, and this requires active neural suppression of the voiding reflex by higher brain centers. Disruption at any level - peripheral nerve, spinal cord, or brain - produces predictable patterns of dysfunction, making an understanding of this neuroanatomy essential for diagnosing and managing neurogenic bladder disorders.
Did periaqueductal grey have inhibitory or excitation effect on PMC
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have a clear and detailed textbook answer. Here is the precise explanation:
PAG's Effect on the PMC: It's a Gate, Not a Simple Switch
The relationship is neither purely inhibitory nor purely excitatory - it depends entirely on the phase (storage vs. voiding). The PAG functions as a conditional relay/gate that changes its output based on integrated input from the bladder and higher brain centers.
During the Storage Phase - PAG Gates/Withholds Excitation to PMC
Bladder afferent signals (Aδ fibers) ascend the spinal cord and reach the PAG continuously during filling. However, the PAG does not forward this signal to the PMC because the medial prefrontal cortex sends tonic descending inhibition to the PAG (via the anterior thalamic radiation). This cortical inhibition keeps the PAG from activating the PMC.
In other words: Cortex → inhibits PAG → PAG withholds excitation from PMC → PMC stays quiet → bladder stays in storage mode.
This is described in Campbell Walsh Wein Urology as the "normal continence mechanism": "It depends on tonic inhibition of the brainstem switch via a long return pathway from the medial prefrontal cortex to the brainstem switch (probably via the anterior thalamic radiation... to the periaqueductal gray [PAG]). The inhibition is switched off for voiding."
During the Voiding Phase - PAG Excites / Disinhibits the PMC
When two conditions are met simultaneously:
- Bladder afferents signal sufficient fullness (threshold reached)
- Cortical "permission" is granted (appropriate time/place to void)
...the prefrontal cortex releases its tonic inhibition of the PAG. The PAG then activates the PMC (M-region / Barrington's nucleus), which fires descending commands:
- Excite sacral parasympathetics → detrusor contraction
- Inhibit Onuf's nucleus → sphincter relaxation
So during voiding: Cortex releases inhibition → PAG activates PMC → voiding occurs.
Summary Table
| Phase | Cortex → PAG | PAG → PMC | PMC Activity | Bladder State |
|---|---|---|---|---|
| Storage | Tonic inhibition | Withholds activation (gates signal) | Quiet | Filling, continent |
| Voiding | Inhibition withdrawn | Excites / disinhibits PMC | Active | Contracts, sphincter relaxes |
Key Conceptual Point
The PAG's primary role is integrative gating - it collects ascending bladder fullness signals from below and descending volitional/emotional signals from above (prefrontal cortex, hypothalamus, insula), then decides whether to activate the PMC. This is why:
- Anxiety or urgency can lower the threshold (hypothalamic/limbic input to PAG → easier PMC activation → frequency/urgency)
- Frontal lobe damage (stroke) removes the cortical inhibition on PAG → PAG disinhibits PMC tonically → detrusor overactivity (OAB)
- Spinal cord injury (above sacral level) breaks the spinal-to-PAG afferent loop → PAG never gets the signal to activate PMC properly → vesicospinovesical C-fiber reflex takes over
Sources: Campbell Walsh Wein Urology (Fig. 110.40 working model), Bradley and Daroff's Neurology in Clinical Practice, Smith and Tanagho's General Urology 19th Ed.
A-delta afferent from bladder passes vial dorsal column or spinothalamic tract
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
This is a direct and detailed answer from the textbook. Here is a precise, well-sourced response:
Bladder Aδ Afferents: Spinal Cord Pathway
The answer requires separating two different ascending pathways, because they serve two different purposes.
The Core Answer
Bladder Aδ afferents ultimately use both pathways for different functions, but the spinothalamic tract is the route for conscious bladder sensation, while a dedicated spino-bulbar (spinopontine) ascending tract carries the micturition reflex signal to the PAG/PMC.
Step-by-Step Pathway
1. Entry into the spinal cord
Aδ fibers from the urothelium, suburothelium, and detrusor muscle travel via the pelvic nerve (and partly hypogastric nerve) to the lumbosacral cord (S2-S4). They terminate on interneurons in the lateral aspect of the dorsal horn and the intermediate zone of the lumbosacral cord. - Campbell Walsh Wein Urology
2. From dorsal horn - two separate ascending streams:
| Stream | Tract | Destination | Function |
|---|---|---|---|
| Micturition reflex arc | Spinopontine / spino-bulbar ascending tract (lateral funiculus) | PAG → PMC (pons) | Triggers the micturition reflex |
| Conscious awareness | Spinothalamic tract (anterolateral system) | Thalamus → sensory cortex | Sensation of fullness, pain, temperature, touch |
As stated directly in Campbell Walsh Wein:
"The spinothalamic and spinohypothalamic tracts are thought not to play a specific role in the basic micturition reflex but are involved in sensory processes such as sensation of urogenital pain, temperature, touch, and conscious awareness of bladder filling and voiding. The sensory cortex is constantly informed about the fullness of the urinary bladder via the spinothalamic tract."
"Sacral spinal interneurons and their ascending sensory pathway to the PAG and the PMC... [carry] bladder filling information."
So What About the Dorsal Columns?
The dorsal columns are NOT the pathway for bladder afferents. Dorsal columns carry fine touch, vibration, and proprioception from the limbs. Bladder sensation runs in the anterolateral system (spinothalamic) for conscious sensation, not the dorsal columns.
This is confirmed clinically:
- Dorsal column lesions (e.g., tabes dorsalis, subacute combined degeneration) → lose proprioception and vibration sense, but bladder sensation is relatively preserved initially
- Anterior/lateral cord lesions → can impair bladder sensation and the micturition reflex
Important Clinical Nuance: The Micturition Reflex Tract
The ascending limb of the micturition reflex itself (bladder → PAG → PMC) travels in the dorsolateral funiculus (lateral white matter), not the spinothalamic tract per se. This is why:
- Spinal cord injury above the sacral level but with intact lateral funiculi can sometimes preserve a spinal micturition reflex via C-fibers
- The reflex and the sensation use parallel but distinct ascending routes
Summary
| Pathway | Tract | Role |
|---|---|---|
| Aδ → dorsal horn interneurons → spinothalamic tract | Anterolateral | Conscious sensation of fullness, pain, temperature |
| Aδ → dorsal horn interneurons → spinopontine/dorsolateral funiculus | Lateral white matter | Micturition reflex (to PAG → PMC) |
| Dorsal columns | Posterior | NOT involved in bladder afferent signaling |
Source: Campbell Walsh Wein Urology - Neurophysiology Relevant to Electrical Stimulation for Storage and Voiding Disorders
This is a shared conversation. Sign in to Orris to start your own chat.