Hernia classification
Hernia Classification
1. Broad Classification by Etiology
| Category | Examples |
|---|---|
| Congenital | Omphalocele, gastroschisis, umbilical (infant), indirect inguinal (incomplete obliteration of processus vaginalis) |
| Acquired | Direct inguinal, incisional, femoral (rare de novo), epigastric, umbilical (adult) |
| Traumatic | Penetrating, blunt, auto-penetrating |
- Maingot's Abdominal Operations, Anatomic Classification
- Mulholland and Greenfield's Surgery 7e, p. 3718-3719
2. Classification by Location
A. Groin (Inguinal Region) Hernias
| Type | Location | Key Features |
|---|---|---|
| Indirect inguinal | Lateral to inferior epigastric vessels; through deep inguinal ring | Congenital; follows spermatic cord; most common hernia overall; right > left |
| Direct inguinal | Medial to inferior epigastric vessels; within Hesselbach's triangle | Acquired; weakness of inguinal floor; rare in young |
| Femoral | Below inguinal ligament; through femoral ring | <10% of groin hernias; higher strangulation risk (up to 40%); more common in women and elderly |
| Pantaloon (saddlebag) | Both direct and indirect components simultaneously, straddling the inferior epigastric vessels |
- Maingot's Abdominal Operations
- Schwartz's Principles of Surgery 11e, p. 1629
B. Ventral (Anterior Abdominal Wall) Hernias
| Type | Location/Features |
|---|---|
| Epigastric | Through linea alba above umbilicus; often fat only |
| Umbilical | Through umbilical ring; congenital or acquired in adults |
| Paraumbilical | Adjacent to umbilicus; adult acquired type |
| Incisional | Through a previous surgical scar; most common after midline laparotomy |
| Spigelian | Through the spigelian fascia (lateral edge of rectus sheath, along semilunar line) |
| Interparietal | Between layers of abdominal wall (rare) |
| Parastomal | Adjacent to a stoma |
- Mulholland and Greenfield's Surgery 7e, Table 72.8
C. Hiatus Hernias (Diaphragmatic)
| Type | Description |
|---|---|
| Type I (Sliding) | Esophagogastric junction (EGJ) herniates above diaphragm into mediastinum; predisposes to GORD |
| Type II (Paraesophageal/Rolling) | Fundus herniates alongside a normally positioned EGJ |
| Type III (Mixed) | Both EGJ and gastric fundus herniate - combined sliding + rolling |
| Type IV | Large defect; other organs (colon, spleen, small bowel) also herniate |
- Bailey & Love 28e; Current Surgical Therapy 14e
D. Internal Hernias
3. Classification by Clinical State (Complexity)
| Type | Features |
|---|---|
| Occult | Not detectable clinically; found incidentally |
| Reducible | Contents can be returned to abdomen; uncomplicated; sac remains in place |
| Irreducible | Contents cannot be returned; no vascular compromise; due to adhesions, very large size, or sliding component |
| Obstructed (Incarcerated) | Irreducible + intestinal obstruction, but NO vascular compromise yet |
| Strangulated | Irreducible + obstruction + arterial blood supply arrested = ischemia/gangrene; surgical emergency |
| Inflamed | Contents (appendix, Fallopian tube, Meckel's diverticulum) become inflamed; mimics strangulation but hernia is not tense |
Clinical tip: A small defect with rigid walls is the highest-risk configuration - it traps contents and blocks venous return first, then arterial flow.
- Bailey & Love 28e, Types of hernia by complexity
- S Das Manual of Clinical Surgery 13e
4. Special Named (Eponymous) Types
| Name | Definition |
|---|---|
| Richter's hernia | Only the antimesenteric wall (partial circumference) of bowel herniates - may strangulate without obstruction or vomiting; easy to miss |
| Littre's hernia | Hernia sac contains a Meckel's diverticulum (and sometimes the appendix) |
| Sliding hernia | Part of the hernia sac is formed by the wall of a retroperitoneal organ (colon or bladder); the visceral peritoneum is the sac wall |
| Maydl's hernia | "W" hernia - two loops of bowel in sac, with a loop inside the abdomen strangulating |
| Amyand's hernia | Appendix within inguinal hernia sac |
| Obturator hernia | Through obturator foramen; presents with medial thigh pain (Howship-Romberg sign) |
| Spigelian hernia | Through spigelian fascia along semilunar line; often interparietal |
| Lumbar hernia | Petit's triangle or Grynfeltt's triangle |
- Mulholland 7e; Sabiston; Tintinalli's Emergency Medicine
5. Formal Classification Systems for Groin Hernias
Nyhus Classification (widely used in USA)
| Type | Description |
|---|---|
| I | Indirect; internal ring normal (infant/child) |
| II | Indirect; internal ring enlarged but posterior wall intact |
| IIIa | Direct inguinal |
| IIIb | Indirect; large; posterior wall deficient; includes pantaloon, sliding |
| IIIc | Femoral |
| IV | All recurrent hernias (IVa direct, IVb indirect, IVc femoral, IVd combined) |
- Schwartz's Principles of Surgery 11e, Table 37-2
European Hernia Society (EHS) Groin Classification
-
Location: M (medial/direct), L (lateral/indirect), F (femoral)
-
Size: 1 (≤1 finger width), 2 (1-2 fingers), 3 (≥3 fingers)
-
Status: P (primary), R (recurrent), X (unknown)
-
Mulholland 7e
6. EHS Classification of Incisional Hernias
| Zone | Subsite | Code |
|---|---|---|
| Midline | Subxiphoid / Epigastric / Umbilical / Infraumbilical / Suprapubic | M1-M5 |
| Lateral | Subcostal / Flank / Iliac / Lumbar | L1-L4 |
| Width | <4 cm / 4-10 cm / >10 cm | W1 / W2 / W3 |
| Recurrent? | Yes / No |
Ventral Hernia Working Group (VHWG) Grading (Risk of SSO)
| Grade | Risk Profile |
|---|---|
| 1 | Low risk; no history of wound infection |
| 2 | Comorbid: smoker, obese, diabetic, immunosuppressed, COPD |
| 3 | Potentially contaminated: prior wound infection, stoma present, GI tract violation |
| 4 | Infected: infected mesh, septic dehiscence |
- Mulholland and Greenfield's Surgery 7e, Tables 72.10-72.11
Make a summary document comparing repair techniques (open vs laparoscopic vs robotic)
hernia repair open laparoscopic robotic comparison outcomes
ls /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or not found"
mkdir -p /home/daytona/workspace/hernia-repair-doc
Difference between obstreted and strangulated hernia
Obstructed vs. Strangulated Hernia
Core Conceptual Difference
| Feature | Obstructed Hernia | Strangulated Hernia |
|---|---|---|
| Reducibility | Irreducible | Irreducible |
| Bowel lumen | Occluded (obstructed) | Occluded (usually) |
| Blood supply | INTACT | COMPROMISED / ARRESTED |
| Bowel viability | Viable | Ischaemic → gangrenous |
| Urgency | Urgent | Surgical emergency |
Obstructed (Incarcerated) Hernia
Irreducibility + Intestinal obstruction (no vascular compromise)
- The bowel lumen is blocked, causing classic features of mechanical small bowel obstruction (colicky pain, vomiting, distension, absolute constipation)
- The bowel wall itself is still viable and pink
- No systemic signs of sepsis or peritonitis
- Can potentially be managed with careful attempts at manual reduction under sedation before definitive repair
Critical clinical warning: It is dangerous to diagnose obstruction when strangulation may be the actual state - this wastes valuable time until it is too late to save the patient's life.
- S Das Manual of Clinical Surgery 13e
Strangulated Hernia
Irreducibility + Obstruction + Arrest of blood supply
- The narrow rigid neck of the hernia constricts the contents
- Venous occlusion occurs first - venous return is impeded, causing congestion and swelling of the incarcerated intestine
- Increasing pressure within the sac impedes arterial inflow
- Venous thrombosis develops → venous gangrene of the intestinal wall
- Bowel wall perforates → infected, toxic contents released → peritonitis and sepsis
- Pye's Surgical Handicraft 22e
- Bailey & Love 28e, Common Principles in Abdominal Hernia
- Omentocele (omentum only in sac)
- Richter's hernia (only the antimesenteric wall of bowel herniates - lumen not fully blocked, yet necrosis advances)
- Littre's hernia (Meckel's diverticulum in sac)
Clinical Features - Side by Side
| Feature | Obstructed | Strangulated |
|---|---|---|
| Pain | Colicky, intermittent | Severe, constant, localised to hernia |
| Swelling | Irreducible, non-tender or mildly tender | Irreducible, extremely tense and tender |
| Skin over hernia | Normal | Red, oedematous, warm |
| Cough impulse | Absent | Absent |
| Bowel obstruction signs | Present | Usually present (may be absent - see above) |
| Systemic sepsis / fever | Absent | Present (late) |
| Peritonism | Absent | Present (if perforation) |
| Temperature | Normal / mildly elevated | Elevated |
Sequence of Events (Spectrum)
Reducible → Irreducible → Obstructed → Strangulated → Perforation → Peritonitis → Death
↑
(venous then arterial occlusion)
Management Implications
| Obstructed | Strangulated | |
|---|---|---|
| Reduction attempt | May be attempted with sedation if no signs of vascular compromise | Contraindicated - gangrenous bowel must not be reduced |
| Timing | Urgent surgery (same admission, after stabilisation) | Emergency surgery - no delay |
| Anaesthesia | General preferred | General (epidural/spinal in selected cases) |
| Mesh use | Can use mesh if field is clean | Avoid prosthetic mesh - bacterial translocation risk; use tissue repair |
| Bowel resection | Usually not required | Required if bowel non-viable (no return of colour/peristalsis after release) |
| Incision | Usually inguinal | May need midline laparotomy if non-viable bowel anticipated |
- Maingot's Abdominal Operations
- Bailey & Love 28e
- S Das Manual of Clinical Surgery 13e
- Pye's Surgical Handicraft 22e
Difference between direct and indirect
Direct vs. Indirect Inguinal Hernia
Hesselbach's Triangle - The Reference Point
| Border | Structure |
|---|---|
| Medial | Lateral edge of rectus sheath |
| Inferior | Inguinal (Poupart's) ligament |
| Superolateral | Inferior epigastric vessels |
Comparison Table
| Feature | Indirect Hernia | Direct Hernia |
|---|---|---|
| Relation to epigastric vessels | Lateral to inferior epigastric vessels | Medial to inferior epigastric vessels |
| Site of defect | Deep (internal) inguinal ring | Posterior wall of inguinal canal (Hesselbach's triangle) |
| Direction of herniation | Through inguinal canal (oblique course) - "indirect" path | Directly forward through abdominal wall - perpendicular course |
| Etiology | Congenital (patent processus vaginalis) or acquired | Always acquired (weakness of inguinal floor) |
| Age group | Any age, including infants and children | Middle-aged to elderly; rarely in young |
| Sex predominance | More common overall; M >> F | Men (age-related floor weakness) |
| Side predominance | Right > left (testicular descent later on right in fetal life) | Often bilateral |
| Descent into scrotum | Yes - can extend into scrotum (indirect = "long hernia") | Rarely (sac pushed forward, emerges medial to cord) |
| Hernia sac coverings | Peritoneum + transversalis fascia + cremaster muscle | Peritoneum + transversalis fascia (no cremaster) |
| Neck of sac | Narrow (at deep ring) - higher risk of strangulation | Wide - seldom strangulates |
| Relation to spermatic cord | Within the cord coverings (lateral to cord at deep ring) | Medial to the cord |
Why the Course Differs
- THIEME General Anatomy Atlas: "The hernial sac courses directly through and perpendicular to the abdominal wall without the 'detour' through the inguinal canal - therefore 'direct hernia'."
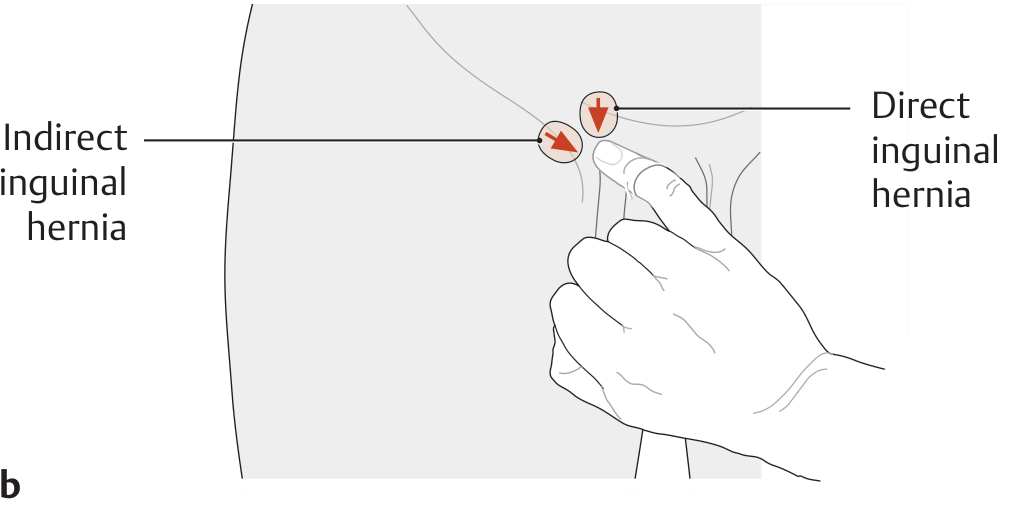
The Invagination Test (Clinical Distinction)
- Indirect hernia - impulse felt at the fingertip (coming down the canal from above-lateral)
- Direct hernia - impulse felt against the pulp (pad) of the finger (pushing straight forward)
Note: Many authorities question the accuracy of this test. Definitive distinction is made intraoperatively by identifying the inferior epigastric vessels.
Strangulation Risk
Memory Aids
- "MDs Don't lie" - Medial = Direct (Don't lie in the canal, push directly forward)
- "Lateral = Indirect" - takes the long route through the canal
- Direct = Degenerative/Dad's hernia (older men, acquired)
- Indirect = Infant/Inherited tendency (congenital, patent processus vaginalis)
Surgical Significance
- Maingot's Abdominal Operations
- Gray's Anatomy for Students
- THIEME General Anatomy Atlas
- Mulholland and Greenfield's Surgery 7e
Clinical difference
Clinical Differences: Direct vs. Indirect Inguinal Hernia
Important caveat upfront: Even experienced surgeons acknowledge it is often difficult to distinguish the two with certainty on clinical examination alone. The definitive distinction is made intraoperatively by identifying the inferior epigastric vessels. All bedside tests are approximate guides, not definitive.
1. History / Patient Profile
| Feature | Indirect | Direct |
|---|---|---|
| Age | Any age - infants, children, young adults, elderly | Middle-aged to elderly |
| Onset | Often since childhood / young adult life | Develops in later life |
| Precipitating history | May follow congenital predisposition (patent processus vaginalis) | Often follows years of raised intra-abdominal pressure (chronic cough, constipation, prostatism, heavy labour) |
| Bilaterality | Usually unilateral (right > left) | More often bilateral |
| Family history | More commonly reported | Less prominent |
2. Inspection
| Feature | Indirect | Direct |
|---|---|---|
| Position of swelling | Appears at the deep ring (above midpoint of inguinal ligament), tracks obliquely toward pubic tubercle | Appears directly above and medial to pubic tubercle |
| Descent into scrotum | Yes - can become inguinoscrotal (large swelling reaching scrotum) | Rarely descends into scrotum - stays in groin |
| Shape | Elongated, pear-shaped ("pyriform"), tubular | Rounded, globular, dome-shaped - pushes straight forward |
| Reducibility on lying | Often reduces spontaneously when patient lies down, with a gurgling sound (if enterocele) | Also reduces on lying, but tends to reduce more readily (wide neck) |
3. Palpation
| Feature | Indirect | Direct |
|---|---|---|
| Spermatic cord | Hernia is within cord coverings - you cannot get above it separately; cord feels thickened at the external ring | Hernia is medial to cord; cord is palpable separately from the swelling |
| Neck of sac | Narrow (at deep ring) - feels tense/tighter | Wide - feels soft, lax, diffuse |
| Consistency | Firmer when tense | Softer, reducible easily with wide base |
| Impulse on coughing | Felt as an expansile impulse directed downward and forward along the canal | Felt as a diffuse forward bulge medial to the cord |
4. Bedside Differentiation Tests
A. Deep Ring Occlusion Test (Ring Control Test) - Most Reliable Clinical Test
| Result | Interpretation |
|---|---|
| Hernia does NOT appear | Indirect - controlled by occluding its entry point at the deep ring |
| Hernia appears medial to the finger | Direct - exits medial to the deep ring, so occlusion there does not block it |
B. Ziemann's Three-Finger Test
- Index finger on the deep inguinal ring (lateral point)
- Middle finger on the superficial inguinal ring
- Ring finger on the saphenous opening
- Impulse at index finger = Indirect inguinal hernia
- Impulse at middle finger = Direct inguinal hernia
- Impulse at ring finger = Femoral hernia
C. Invagination (Finger) Test
| Impulse location | Interpretation |
|---|---|
| Tip of finger (impulse comes down from above-lateral) | Indirect - sac comes down the canal from the deep ring |
| Pulp of finger (impulse pushes straight forward) | Direct - sac bulges directly forward through the posterior wall |
- Goes upward, backward and outward → indirect
- Goes directly backward → direct
D. Percussion
- Resonant note → hernia contains bowel (enterocele)
- Dull note → contains omentum or extraperitoneal fat (omentocele)
5. Summary Comparison Table
| Clinical Feature | Indirect | Direct |
|---|---|---|
| Age | Any (often young) | Middle-aged / elderly |
| Bilateral | Uncommon | More common |
| Scrotal extension | Common | Rare |
| Shape | Pyriform / elongated | Globular / hemispherical |
| Neck | Narrow | Wide |
| Spontaneous reduction on lying | Often, with gurgle | Usually, easily |
| Strangulation risk | Higher (narrow neck) | Low (wide neck, rarely strangulates) |
| Deep ring occlusion | Hernia controlled | Hernia not controlled |
| Invagination test | Impulse at fingertip | Impulse at pulp |
| Relation to spermatic cord | Inside cord coverings | Medial to cord |
| Definitive distinction | Intraoperative - lateral to inferior epigastric vessels | Intraoperative - medial to inferior epigastric vessels |
6. Why the Clinical Distinction Matters Less Surgically
-
Counselling (indirect can appear in children; direct suggests acquired weakness)
-
Predicting strangulation risk
-
Academic/exam purposes
-
Bailey & Love's Surgery 28e
-
S Das Manual of Clinical Surgery 13e
-
Mulholland & Greenfield's Surgery 7e
Create a clinical summary poster comparing all hernia complications
A detailed clinical summary medical poster titled "Hernia Complications: Clinical Comparison" with a clean professional medical education layout on a dark navy blue background with white and colored text. The poster contains 5 major complication sections arranged in a grid, each in a distinct colored card: 1. IRREDUCIBLE HERNIA (orange card): Definition: contents cannot be returned to abdomen. Causes: adhesions, sliding hernia, large scrotal hernia. Features: non-tender, no vascular compromise, no bowel obstruction. Management: elective surgery. 2. OBSTRUCTED HERNIA (yellow card): Formula: Irreducibility + Intestinal Obstruction (NO vascular compromise). Features: colicky pain, vomiting, distension, constipation, hernia not tender or tense, bowel viable and pink. Management: urgent surgery, mesh can be used. 3. STRANGULATED HERNIA (red card): Formula: Irreducibility + Obstruction + Arrest of Blood Supply. Pathophysiology: venous occlusion first → venous congestion → arterial block → ischaemia → gangrene → perforation → peritonitis. Features: extremely tense and tender swelling, red overlying skin, no cough impulse, severe constant pain, systemic sepsis. Note: obstruction may be ABSENT in Richter's, Littre's, omentocele. Management: EMERGENCY surgery, no mesh, may need bowel resection. 4. INFLAMED HERNIA (purple card): Cause: inflamed content (appendix, Fallopian tube, Meckel's diverticulum). Features: red, oedematous, painful, NOT tense, NOT associated with bowel obstruction. Differentiates from strangulation by absence of tenseness. 5. KEY DIFFERENCES TABLE (blue card): A comparison table with rows for Blood Supply, Bowel Obstruction, Tenderness, Tension/Tense, Urgency, Mesh Use comparing Irreducible vs Obstructed vs Strangulated. Bottom section shows a progression arrow: Reducible → Irreducible → Obstructed → Strangulated → Perforation → Peritonitis → Death Footer shows source: Bailey & Love, S Das Manual of Clinical Surgery, Mulholland & Greenfield Surgery. Modern clean medical poster style with icons.
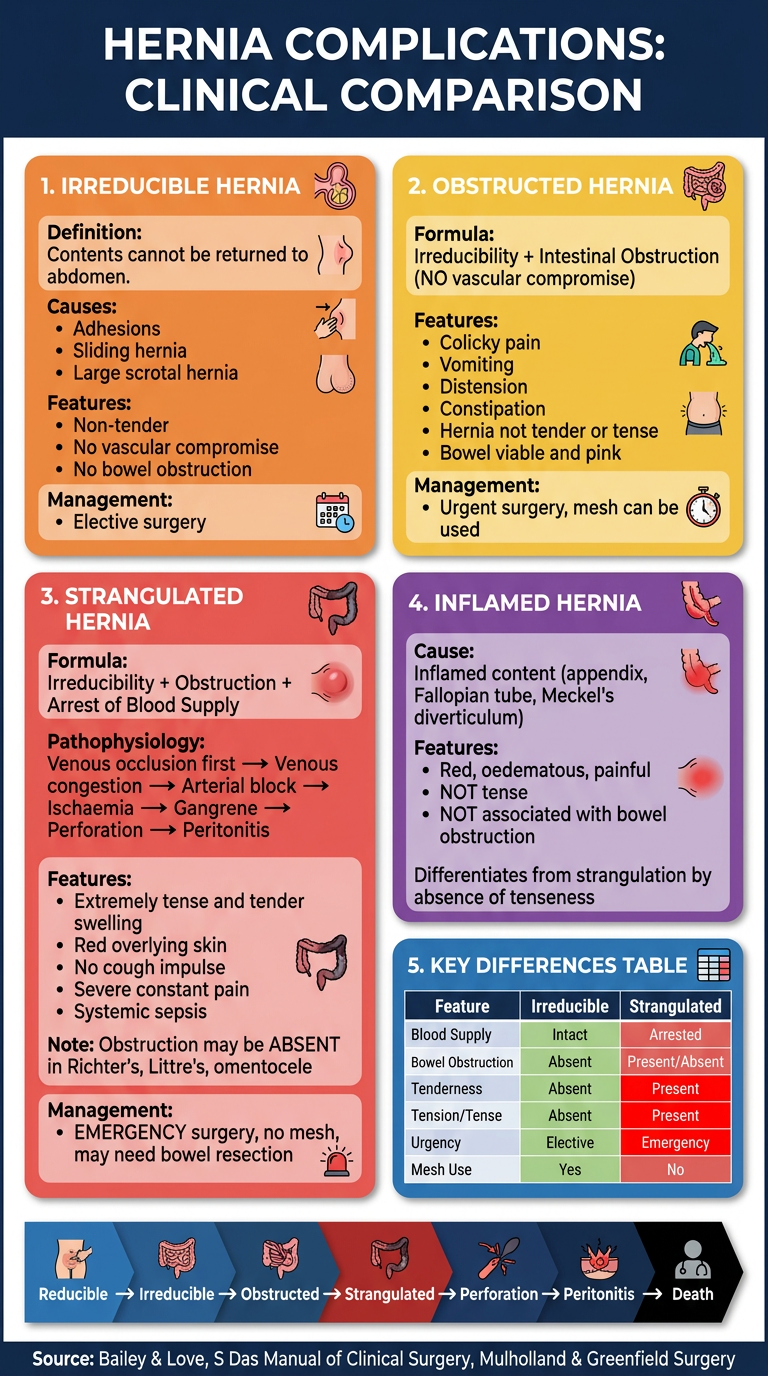
- Irreducible - contents stuck, no vascular issue, elective management
- Obstructed - bowel lumen blocked, blood supply intact, urgent surgery
- Strangulated - blood supply arrested, surgical emergency, no mesh
- Inflamed - content inflamed (appendix/Meckel's), NOT tense, mimics strangulation
- Pantaloon/special types referenced in the comparison
Step wise how to perform Ring invagination Ring occlusion Zimen test
Three Hernia Examination Tests - Stepwise Guide
PRE-REQUISITE FOR ALL THREE TESTS
All three tests require the hernia to be fully reduced first. If the hernia does not reduce spontaneously when the patient lies down, gently reduce it manually (flex, adduct, and internally rotate the thigh; apply gentle pressure on the fundus directed toward the superficial ring).
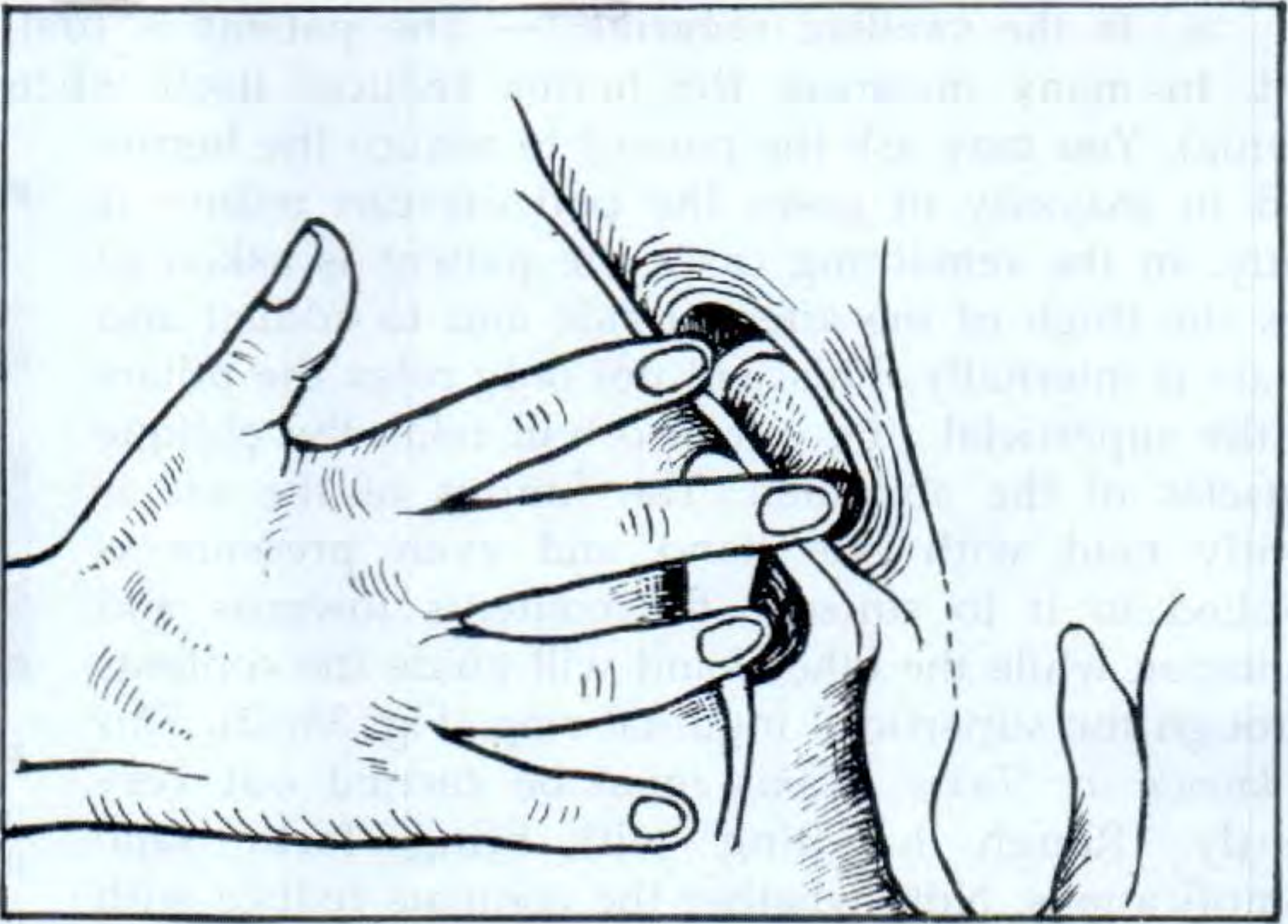
TEST 1 — INVAGINATION TEST (Ring Test / Finger Test)
Landmarks First
- Superficial (external) inguinal ring - triangular slit just above and medial to the pubic tubercle
- Deep (internal) inguinal ring - ½ inch above the midpoint between ASIS and pubic symphysis
Steps
- The nail faces toward the spermatic cord
- The pulp (pad) faces posteriorly (backward)
- Goes upward, backward and outward → canal track of indirect hernia
- Goes directly backward → posterior wall defect of direct hernia
| What you feel | Interpretation |
|---|---|
| Impulse at the tip of finger | Indirect (oblique) hernia - comes down the canal from above-lateral |
| Impulse at the pulp of finger | Direct hernia - pushes straight forward through the posterior wall |
Normal response: The two pillars of the external ring squeeze the examining finger. A palpable impulse at any point confirms a hernia.
- S Das Manual of Clinical Surgery 13e, Figs 38.13-38.16
TEST 2 — RING OCCLUSION TEST (Deep Ring Pressure Test)
Steps
½ inch above the midpoint between ASIS and the pubic symphysis (This is just above the mid-inguinal point, over the deep ring)
| Result | Interpretation |
|---|---|
| No bulge appears - hernia controlled | Indirect hernia - its pathway (deep ring) is blocked |
| Bulge appears medial to the thumb | Direct hernia - exits through the posterior wall medial to your thumb |


- S Das Manual of Clinical Surgery 13e, Figs 38.15 & 38.16
TEST 3 — ZIEMANN'S THREE-FINGER TEST (Zieman's Technique)
Steps
| Finger | Position | Hernia it detects |
|---|---|---|
| Index finger | Over the deep inguinal ring (½ inch above the midpoint between ASIS and pubic symphysis) | Indirect inguinal hernia |
| Middle finger | Over the superficial inguinal ring (just above and medial to the pubic tubercle) | Direct inguinal hernia |
| Ring finger | Over the saphenous opening (4 cm below and lateral to the pubic tubercle) | Femoral hernia |
| Impulse felt at | Diagnosis |
|---|---|
| Index finger | Indirect inguinal hernia |
| Middle finger | Direct inguinal hernia |
| Ring finger | Femoral hernia |
Important limitation: This test is only applicable before a hernia has become visible, or after complete reduction. Once a hernia is obvious on inspection, the test adds little. It is primarily a teaching and diagnostic tool when the hernia is small or occult.
- S Das Manual of Clinical Surgery 13e, Fig 38.11
SUMMARY COMPARISON OF THE THREE TESTS
| Feature | Invagination Test | Ring Occlusion Test | Ziemann's Test |
|---|---|---|---|
| Position | Supine preferred | Standing | Standing |
| Requires reduction? | Yes | Yes | Yes |
| What finger enters | Into inguinal canal via scrotum | Thumb presses over deep ring externally | Three fingers placed on surface |
| Differentiates | Direct vs. indirect | Direct vs. indirect | All three types simultaneously |
| Result | Tip = indirect; Pulp = direct | No bulge = indirect; Medial bulge = direct | Impulse under index/middle/ring |
| Most reliable | Moderate (accuracy questioned) | Most reliable bedside test | Useful for occult hernias |
| Limitation | Uncomfortable; only for males | Does not distinguish femoral | Cannot apply if hernia visible |
- S Das Manual of Clinical Surgery 13e
- Mulholland & Greenfield's Surgery 7e
- Bailey & Love's Short Practice of Surgery 28e
Create a clinical quick reference card (PDF or poster) of these three examination tests for bedside use
mkdir -p /home/daytona/workspace/hernia-ref-card && python3 -c "import reportlab…
Classification of hernia
Classification of Hernia
I. BY ETIOLOGY
A. Congenital
- Omphalocele
- Gastroschisis
- Umbilical hernia (infant) - arrest of normal closure of umbilical ring
- Indirect inguinal hernia - patent processus vaginalis (most common congenital hernia)
B. Acquired
- Direct inguinal - weakness of inguinal floor (always acquired)
- Femoral - always acquired
- Incisional - follows surgical scar
- Epigastric, paraumbilical (adult), Spigelian
- Traumatic - penetrating, blunt
II. BY LOCATION
A. Groin (Inguinal Region)
| Type | Key Feature |
|---|---|
| Indirect inguinal | Lateral to inferior epigastric vessels; through deep ring; follows spermatic cord |
| Direct inguinal | Medial to inferior epigastric vessels; through Hesselbach's triangle |
| Femoral | Below inguinal ligament; through femoral ring; high strangulation risk |
| Pantaloon | Both direct + indirect components together, straddling inferior epigastric vessels |
- Inferior - inguinal ligament
- Medial - lateral edge of rectus sheath
- Superolateral - inferior epigastric vessels
B. Anterior Abdominal Wall (Ventral)
| Type | Location |
|---|---|
| Epigastric | Through linea alba above umbilicus |
| Umbilical | Through umbilical ring; congenital or adult acquired |
| Paraumbilical | Adjacent to umbilicus in adults |
| Incisional | Through previous surgical scar; commonest after midline laparotomy |
| Spigelian | Through spigelian fascia at lateral border of rectus sheath (semilunar line) |
| Interparietal | Between layers of abdominal wall |
| Parastomal | Adjacent to a stoma |
| Diastasis recti | Wide separation of recti with intact but stretched linea alba (not a true hernia - no fascial defect) |
C. Diaphragmatic / Hiatus Hernias
| Type | Description |
|---|---|
| Type I - Sliding | EGJ herniates above diaphragm; predisposes to GORD |
| Type II - Paraesophageal/Rolling | Gastric fundus herniates alongside normally positioned EGJ |
| Type III - Mixed | Both EGJ and fundus herniate |
| Type IV | Large defect; other organs (colon, spleen, small bowel) involved |
D. Internal Hernias
- Paraduodenal (most common internal hernia)
- Pericecal
- Foramen of Winslow
- Transmesenteric
- Intersigmoid
E. Rare/Other Sites
- Obturator hernia - through obturator foramen; Howship-Romberg sign (medial thigh pain)
- Lumbar hernia - Petit's triangle (inferior) or Grynfeltt's triangle (superior)
- Gluteal / sciatic hernia - through greater/lesser sciatic foramen
- Perineal hernia - through pelvic floor
III. BY CLINICAL STATE (Complexity)
| Type | Definition | Blood Supply | Urgency |
|---|---|---|---|
| Occult | Not detectable clinically | Normal | None |
| Reducible | Contents return to abdomen freely | Normal | Elective |
| Irreducible | Contents cannot be returned; no vascular compromise | Normal | Elective/urgent |
| Obstructed (Incarcerated) | Irreducible + bowel lumen obstructed | Intact | Urgent |
| Strangulated | Irreducible + obstructed + blood supply arrested | Compromised | Emergency |
| Inflamed | Contents (appendix, Meckel's, tube) inflamed; not tense; no obstruction | Normal | Urgent |
IV. SPECIAL / EPONYMOUS TYPES
| Name | Definition | Key Point |
|---|---|---|
| Richter's hernia | Only antimesenteric wall of bowel herniates (partial circumference) | Can strangulate WITHOUT obstruction; easy to miss |
| Littre's hernia | Sac contains Meckel's diverticulum | Must resect diverticulum if strangulated |
| Sliding hernia (en glissade) | Part of sac wall IS the visceral peritoneum of a retroperitoneal organ (caecum, sigmoid, bladder) | Cannot ligate sac normally |
| Maydl's hernia | "W" hernia - two loops in sac, central loop inside abdomen strangulates | Bowel inside abdomen necroses - danger if sac contents reduced without checking |
| Amyand's hernia | Appendix within inguinal hernia sac | |
| Pantaloon hernia | Simultaneous direct + indirect components | Straddles inferior epigastric vessels |
V. FORMAL GRADING SYSTEMS
Nyhus Classification (Groin Hernias - popular in USA)
| Type | Description |
|---|---|
| I | Indirect; internal ring normal (infants/children) |
| II | Indirect; ring enlarged; posterior wall intact |
| IIIa | Direct inguinal |
| IIIb | Indirect; large; posterior wall deficient; includes pantaloon/sliding |
| IIIc | Femoral |
| IVa-d | All recurrent hernias (a=direct, b=indirect, c=femoral, d=combined) |
European Hernia Society (EHS) Groin Classification
- Location: M (medial/direct), L (lateral/indirect), F (femoral)
- Size: 1 (≤1 finger), 2 (1-2 fingers), 3 (≥3 fingers)
- Status: P (primary), R (recurrent), X (unknown)
EHS Classification of Incisional Hernias
| Zone | Sites | Code |
|---|---|---|
| Midline | Subxiphoid / Epigastric / Umbilical / Infraumbilical / Suprapubic | M1-M5 |
| Lateral | Subcostal / Flank / Iliac / Lumbar | L1-L4 |
| Width | <4 cm / 4-10 cm / >10 cm | W1 / W2 / W3 |
VHWG Grading (Ventral Hernia Working Group - risk of SSO)
| Grade | Profile |
|---|---|
| 1 | Low risk; no wound infection history |
| 2 | Comorbid: smoker, obese, diabetic, immunosuppressed, COPD |
| 3 | Potentially contaminated: prior wound infection, stoma, GI violation |
| 4 | Infected: infected mesh, septic dehiscence |
QUICK SUMMARY MIND MAP
HERNIA
├── By ETIOLOGY: Congenital / Acquired / Traumatic
├── By LOCATION
│ ├── Groin: Indirect / Direct / Femoral / Pantaloon
│ ├── Ventral: Epigastric / Umbilical / Incisional / Spigelian
│ ├── Diaphragmatic: Type I-IV hiatus
│ └── Internal / Rare: Obturator, Lumbar, Perineal
├── By CLINICAL STATE
│ └── Reducible → Irreducible → Obstructed → Strangulated
├── EPONYMOUS: Richter / Littre / Sliding / Maydl / Amyand
└── FORMAL SYSTEMS: Nyhus / EHS / VHWG
- Maingot's Abdominal Operations
- Mulholland & Greenfield's Surgery 7e
- Bailey & Love's Surgery 28e
- Schwartz's Principles of Surgery 11e
- S Das Manual of Clinical Surgery 13e




Notes
Hernia Classification — E-Note Summary (pp. 609–612)
1. Named Hernias Based on Content ⭐
| Name | Content |
|---|---|
| Enterocele | Bowel (intestinal loop) |
| Omentocele / Epiplocele | Omentum |
| Cystocele | Urinary Bladder |
| Amyand's Hernia ⭐ | Appendix |
| Littre's Hernia ⭐ | Meckel's Diverticulum |
Omentocele vs Enterocele
| Feature | Omentocele/Epiplocele | Enterocele |
|---|---|---|
| Content | Omentum | Intestine |
| Consistency | Doughy, granular | Elastic |
| Reducibility | Easy initially, difficult later | Difficult initially, easier later |
| Peristalsis | Absent | Present |
| Bowel sounds | Absent | Present |
| Percussion | Dull note | Tympanic note |
Exam tip: Tympanic percussion = enterocele (bowel = gas-filled). Dull = omentocele.
2. Types of Hernia Based on Complexity (MCQ) ⭐
A. Occult Hernia
- Not detected clinically at all
B. Reducible Hernia
- Swelling comes and goes
- Contents of hernia sac move freely in and out
- Taxis = gentle forceful manual reduction of hernia sac
- Sac remains even after contents are reduced
- Cough impulse present
- Uncomplicated; chances of complications exist but not yet occurred
C. Irreducible Hernia
- Contents of sac cannot be returned to abdomen
- Higher chance of complications
- Causes of irreducibility:
- Adhesion of contents to each other
- Adhesion of contents to the sac
- Adhesion of one part of sac to another
- Sliding hernia
- Very large scrotal hernia (Scrotal Abdomen)
D. Incarcerated Hernia
- Irreducible hernia with trapped content
- Increased risk of strangulation, especially with a small neck
- Not yet strangulated
- Obstructed Hernia = incarcerated hernia containing bowel → signs/symptoms of intestinal obstruction
- Irreducibility + Intestinal Obstruction
- No interference with blood supply
E. Strangulated Hernia ⭐
- Typically occurs when bowel is present in the sac
- Obstruction may NOT be present in certain cases:
- Omentocele (omentum only)
- Littre's hernia (Meckel's diverticulum)
- Richter's hernia (partial bowel wall)
- Acutely painful swelling
- Absent cough impulse
- Contents become ischaemic due to lack of arterial blood supply
- Overlying skin: red, oedematous (cellulitis)
F. Infarcted Hernia
- Contents of hernia: gangrenous
- High mortality
3. Other Special Types
A. Inflamed Hernia
- Contents inflamed: Appendix, Salpinx, Meckel's Diverticulum
- Very rare
- Local signs of inflammation:
- Overlying skin: red, oedematous
- Swelling: painful, tender, swollen
| Feature | Inflamed | Strangulated |
|---|---|---|
| Tense | Not tense | Tense |
| Bowel obstruction | Not present | Usually present |
| Blood supply | Intact | Arrested |
B. Interstitial (Interparietal) Hernia
- Hernia lies completely between the musculofascial layers of abdominal wall
- No peritoneal sac present
- Example: Spigelian Hernia
C. Internal Hernia
- Bowel gets trapped within the peritoneal cavity in naturally occurring spaces:
- Foramen of Winslow
- Paraduodenal Fossa
- Paracaecal Fossae
D. Richter's Hernia ⭐
- Only a portion of bowel circumference strangulated (not full lumen)
- Often complicates femoral hernia and rarely obturator hernia
- Bowel obstruction may or may not be present
- Bowel can still become necrotic → perforate → life threatening
- Dangerous because obstruction signs can be absent despite advancing necrosis
E. Divarication of Recti (Diastasis Recti)
- Due to stretching and weakening of linea alba
- Two recti muscles part from each other
- Common in elderly multiparas
- Fascia transversalis intact, midline aponeurosis intact - not a true hernia
- Ask supine patient to lift head off pillow → midline bulge becomes visible due to raised intra-abdominal pressure
4. Key Pointers for Examining Hernia
- Reducibility
- Tenderness
- Cough impulse
- Overlying skin changes (cellulitis in strangulated hernia)
- Multiple defects / contralateral side (20% of patients present with hernia on both sides)
QUICK REVISION - Complexity Progression
Reducible
↓
Irreducible (contents stuck, no vascular issue)
↓
Incarcerated (trapped, risk of strangulation, small neck)
↓
Obstructed (+ bowel obstruction, blood supply intact)
↓
Strangulated (+ blood supply arrested → ischaemia)
↓
Infarcted (gangrene → perforation → peritonitis → death)
ADDITIONS to supplement your notes
| Point | Detail |
|---|---|
| Strangulation sequence | Venous occlusion FIRST → congestion → then arterial block → gangrene |
| Most common site of strangulation | Femoral > Umbilical > Inguinal |
| Femoral hernia strangulation risk | 22% at 3 months, 45% at 2 years |
| Mesh in strangulation | Avoid prosthetic mesh - bacterial translocation risk |
| Taxis | Contraindicated in strangulation - may reduce gangrenous bowel into abdomen |
| Maydl's hernia | "W" hernia - central loop inside abdomen strangulates; danger if sac contents reduced without checking inside |
| Amyand's hernia | Must resect appendix if inflamed/strangulated at time of repair |
Based on clinical in difference table
Clinical Differentiation Table — Hernia Types by Complexity
| Feature | Reducible | Irreducible | Obstructed (Incarcerated) | Strangulated | Inflamed | Infarcted |
|---|---|---|---|---|---|---|
| Definition | Contents freely in/out | Contents cannot return | Irreducible + bowel lumen blocked | Irreducible + obstruction + blood supply arrested | Contents inflamed | Contents gangrenous |
| Formula | - | Irreducibility alone | Irreducibility + IO | Irreducibility + IO + Blood supply arrest | Inflammation of content | End stage strangulation |
| Blood supply | ✅ Normal | ✅ Normal | ✅ Intact | ❌ Arrested | ✅ Normal | ❌ ❌ Gangrenous |
| Bowel obstruction | ❌ Absent | ❌ Absent | ✅ Present | Usually present (may be absent) | ❌ Absent | Present/absent |
| Reducibility | ✅ Reduces freely | ❌ Cannot reduce | ❌ Cannot reduce | ❌ Cannot reduce | ❌ Cannot reduce | ❌ Cannot reduce |
| Cough impulse | ✅ Present | ✅ Present | ± May be present | ❌ Absent | ❌ Absent | ❌ Absent |
| Pain | None / mild dragging | Mild discomfort | Colicky, intermittent | Severe, constant | Localised, dull | Severe |
| Tenderness | ❌ None | ❌ None / mild | ± Mild | ✅ Extremely tender | ✅ Tender | ✅ ✅ Extreme |
| Tense/taut swelling | ❌ Soft | ❌ Soft | ± Slightly tense | ✅ Extremely tense | ❌ Not tense ⭐ | ✅ Tense |
| Overlying skin | Normal | Normal | Normal | ❌ Red, oedematous (cellulitis) | Red, oedematous | Dark, discoloured |
| Fever / systemic | ❌ None | ❌ None | ❌ None / mild | ✅ Late feature | ✅ Local signs | ✅ ✅ Sepsis |
| Vomiting | ❌ None | ❌ None | ✅ Present (IO) | ✅ Present | ❌ None | ✅ Present |
| Distension | ❌ None | ❌ None | ✅ Present | ✅ Present | ❌ None | ✅ Present |
| Bowel sounds | Normal | Normal | ✅ ↑ Tinkling | ✅ → ❌ (absent late) | Normal | ❌ Absent |
| Urgency | Elective | Elective/urgent | ⚠️ Urgent | 🚨 Emergency | ⚠️ Urgent | 🚨 Emergency |
| Mesh usable? | ✅ Yes | ✅ Yes | ✅ Yes (if clean) | ❌ No (infection risk) | ❌ Avoid | ❌ No |
| Taxis (manual reduction) | ✅ Safe | Careful | Attempt with sedation | ❌ Contraindicated | ❌ Avoid | ❌ Contraindicated |
| Bowel resection needed? | No | No | Rarely | ✅ If non-viable | No | ✅ Yes |
| Examples | Common inguinal | Sliding hernia, large scrotal | Narrow-neck inguinal | Femoral, umbilical | Appendix in sac, Meckel's | End-stage any hernia |
Key Distinguishing Points (MCQ Favourites) ⭐
1. Strangulated vs. Inflamed — Most Tested Distinction
| Feature | Strangulated | Inflamed |
|---|---|---|
| Tense | ✅ Yes | ❌ No ← key |
| Bowel obstruction | ✅ Usually | ❌ No ← key |
| Blood supply | Arrested | Intact |
| Cause | Constriction at neck | Content itself inflamed |
2. Obstructed vs. Strangulated — Most Dangerous to Confuse
| Feature | Obstructed | Strangulated |
|---|---|---|
| Blood supply | ✅ Intact | ❌ Arrested |
| Tenderness | Mild | Extreme |
| Skin over hernia | Normal | Red, oedematous |
| Tense | Mildly | Extremely |
| Urgency | Urgent | Emergency |
⭐ S Das warning: "It is a dangerous venture to diagnose obstructed hernia when strangulation may be the real state of affairs - valuable time will be wasted until it is too late."
3. Obstruction May Be ABSENT in Strangulation — 3 Exceptions ⭐
| Hernia | Why no obstruction |
|---|---|
| Richter's hernia | Only partial bowel circumference trapped - lumen not fully blocked |
| Littre's hernia | Meckel's diverticulum in sac - not full bowel loop |
| Omentocele | Omentum only in sac - no bowel involved |
4. Cough Impulse Summary
| Type | Cough Impulse |
|---|---|
| Reducible | ✅ Present |
| Irreducible | ✅ Present (usually) |
| Obstructed | ± Variable |
| Strangulated | ❌ Absent |
| Inflamed | ❌ Absent |
| Infarcted | ❌ Absent |
Cough impulse absent = neck blocked by strangulation / adhesions / irreducible content
5. Percussion Note
| Content | Note |
|---|---|
| Bowel (enterocele) | Tympanic / Resonant |
| Omentum (omentocele) | Dull |
| Bladder (cystocele) | Dull |
Progression Flowchart
REDUCIBLE
↓ (adhesions form / small neck)
IRREDUCIBLE
↓ (bowel enters sac, lumen blocked)
OBSTRUCTED ──→ Signs of intestinal obstruction
↓ (venous occlusion → arterial arrest)
STRANGULATED ──→ Absent cough impulse, tense, red skin
↓ (arterial supply gone completely)
INFARCTED ──→ Gangrene → Perforation → Peritonitis → DEATH
IRREDUCIBLE + inflamed content → INFLAMED HERNIA
(NOT tense, NO bowel obstruction)
Occult
Occult Hernia
Definition
From your notes: "Occult hernia = Not detected clinically" — this is the simplest and most exam-relevant definition.
Why It Occurs
- Too small to produce a visible or palpable bulge
- Intermittent - reduces completely at rest; only appears on prolonged standing, straining, or exercise
- Deep/interparietal - lies between fascial layers with no external bulge (e.g. Spigelian hernia)
- Contralateral patent processus vaginalis in children - the ring is open but no hernia has yet herniated through it
Clinical Scenario
Bailey & Love: "Confirmation of the diagnosis may not be possible when the patient describes an intermittent swelling but nothing is found on examination. Surgeons will often accept the diagnosis on history alone but re-examination at a later date or investigation by ultrasound scan may be requested."
How to Unmask / Detect
| Method | Detail |
|---|---|
| Re-examination standing | Always examine upright, not supine - hernias reduce in lying position |
| Valsalva / coughing | Ask patient to strain, cough, or hold nose and blow - raises IAP, may make hernia appear |
| Repeated examination | Re-examine at a later date when hernia may be present |
| Ultrasonography | First-line imaging; dynamic USS (patient straining) best for groin hernias |
| CT scan | Good anatomical detail but may miss hernia if patient is supine (hernia reduces spontaneously) |
| MRI | Excellent for soft tissue but same limitation as CT in supine position |
| Laparoscopy | Gold standard - directly visualises the defect; also detects contralateral occult hernia simultaneously |
| In children | Ask child to jolt/jump from table or cry; palpate spermatic cord - thicker cord = hernial sac present (Gornall's test) |
The Contralateral Occult Hernia — Clinically Important ⭐
| Finding | Figure |
|---|---|
| Patent contralateral processus vaginalis found at open exploration (children) | 57–68% |
| Patent contralateral ring found at laparoscopy (children) | 39–61% |
| Incidence of open contralateral ring in adults at autopsy | 20% |
| Risk of metachronous contralateral hernia developing | ~7% within 5 years |
- Campbell Walsh Wein Urology
- Bailey & Love 28e
Occult Hernia vs. Asymptomatic Hernia
| Occult Hernia | Asymptomatic (Silent) Hernia | |
|---|---|---|
| Detectable on exam? | ❌ No | ✅ Yes, on examination |
| Symptoms? | None or intermittent | None |
| Management | Investigate to confirm | Watchful waiting acceptable (esp. elderly with direct hernia) |
Bailey & Love: "It is safe to recommend no active treatment in cases of early asymptomatic direct hernia, particularly in elderly patients who do not wish for surgical intervention. These patients should be warned to seek early advice if the hernia increases in size or becomes symptomatic."
Management of Occult Hernia
- History alone is often sufficient to plan surgery for intermittent swellings
- Dynamic ultrasound - imaging of choice to confirm
- If confirmed → elective repair (same as any inguinal hernia)
- During laparoscopic repair of a known hernia → inspect contralateral ring and repair simultaneously if open
MCQ Points ⭐
- Occult = not detected clinically - the shortest, most testable definition
- Best investigation = dynamic ultrasound (patient straining)
- CT/MRI may miss the hernia because patient is supine
- 20% of hernia patients have a contralateral occult hernia
- Laparoscopy is gold standard for detection - especially of contralateral ring in children
- Spigelian hernia is a classic interparietal occult hernia - lies between muscle layers, no visible external bulge
Reducible and non Reducible difference
Reducible vs. Non-Reducible Hernia
Key Principle
Main Comparison Table
| Feature | Reducible | Irreducible | Obstructed | Strangulated |
|---|---|---|---|---|
| Contents return to abdomen? | ✅ Yes, freely | ❌ No | ❌ No | ❌ No |
| Bowel obstruction | ❌ No | ❌ No | ✅ Yes | ✅ Usually yes |
| Blood supply | ✅ Normal | ✅ Normal | ✅ Intact | ❌ Arrested |
| Cough impulse | ✅ Present | ✅ Usually present | ± Variable | ❌ Absent |
| Pain | None / dragging | Mild | Colicky, cramps | Severe, constant |
| Tenderness | ❌ None | ❌ None/mild | ± Mild | ✅ Extreme |
| Tense/taut | ❌ Soft | ❌ Soft | ± Slightly | ✅ Extremely tense |
| Overlying skin | Normal | Normal | Normal | ❌ Red, oedematous |
| Bowel sounds | Normal | Normal | ✅ ↑ Tinkling (early) | ↓ / Absent (late) |
| Vomiting | ❌ No | ❌ No | ✅ Yes | ✅ Yes |
| Fever/sepsis | ❌ No | ❌ No | ❌ No | ✅ Late |
| Taxis (manual reduction) | ✅ Safe | Careful | Attempt with sedation | ❌ Contraindicated |
| Risk of complications | Low | Higher | High | Emergency |
| Urgency | Elective | Elective/urgent | ⚠️ Urgent | 🚨 Emergency |
| Mesh | ✅ Yes | ✅ Yes | ✅ Yes (clean field) | ❌ Avoid |
REDUCIBLE HERNIA — Detail
Characteristics:
- Swelling appears on standing/straining, disappears on lying down
- Two classical signs:
- ✅ Impulse on coughing
- ✅ Reducibility
- Sac remains in position even after contents reduce
- Complications are possible but have not occurred yet
How it Reduces:
- Spontaneously - patient lies down, hernia disappears
- Taxis - gentle manual reduction:
- Flex, adduct, internally rotate the thigh (relaxes inguinal muscles)
- Apply gentle pressure on fundus, direct contents toward ring
- Enterocele: first part difficult, last part slips in easily (gurgling sound)
- Omentocele: first part goes in easily, last part resists
Contents and Percussion:
| Content | Sign |
|---|---|
| Bowel (enterocele) | Tympanic/resonant percussion, gurgling on reduction, peristalsis visible/audible |
| Omentum (omentocele) | Dull percussion, doughy feel, no peristalsis |
NON-REDUCIBLE HERNIA — The Spectrum
A. Irreducible (Simple)
- Adhesion of contents to each other
- Adhesion of contents to the sac
- Adhesion of one part of sac to another part
- Sliding hernia (retroperitoneal organ forms part of sac wall)
- Very large scrotal hernia (scrotal abdomen - contents too large to reduce through ring)
- Swelling present all the time, does not reduce
- Non-tender, not tense
- Cough impulse usually still present
- No systemic symptoms
B. Obstructed (Incarcerated)
- Colicky abdominal pain
- Vomiting (may be faeculent late)
- Abdominal distension
- Absolute constipation (no flatus or faeces)
- Hernia swelling: firm, mildly tense
- Tinkling bowel sounds early → silent late
⭐ Key: Blood supply intact - bowel is viable and pink at operation.
C. Strangulated
Neck constricts contents
↓
Venous occlusion FIRST → venous congestion, swelling
↓
Rising pressure → Arterial blood cannot enter
↓
Ischaemia → Gangrene → Perforation → Peritonitis
- Sudden severe, constant pain at hernia site
- Hernia extremely tense and tender
- No cough impulse
- Overlying skin: red, warm, oedematous (cellulitis)
- Systemic: fever, tachycardia, sepsis (later)
- Features of intestinal obstruction (usually)
⭐ Exception - obstruction may be ABSENT in:
- Richter's hernia (partial bowel wall only)
- Littre's hernia (Meckel's diverticulum)
- Omentocele (no bowel)
The ONE Most Important Distinguishing Feature
OBSTRUCTED vs STRANGULATED
= Blood Supply STATUS
Obstructed → Blood supply INTACT → Urgent
Strangulated → Blood supply ARRESTED → Emergency
Causes of Non-Reducibility — Summary
| Cause | Type |
|---|---|
| Adhesions (content-to-content, content-to-sac) | Simple irreducible |
| Sliding hernia | Simple irreducible |
| Large scrotal hernia | Simple irreducible |
| Narrow neck with trapped bowel | Obstructed / Strangulated |
| Richter's hernia (partial wall) | Strangulated without obstruction |
| Inflamed content (appendix, Meckel's) | Inflamed hernia |
Taxis — When to Attempt, When NOT to
| Situation | Taxis |
|---|---|
| Reducible hernia | ✅ Freely |
| Irreducible (no signs of compromise) | ✅ Careful, with sedation |
| Obstructed (no vascular signs) | ✅ Attempt with sedation before surgery |
| Strangulated | ❌ Absolutely contraindicated - risk of reducing gangrenous bowel into abdomen |
Quick Revision Formula
Reducible = Contents in AND out freely
Irreducible = Contents STUCK (no vascular issue)
Obstructed = Stuck + Bowel LUMEN blocked (blood supply OK)
Strangulated = Stuck + Lumen blocked + BLOOD SUPPLY GONE
Infarcted = Strangulated → Gangrene (end stage)
- S Das Manual of Clinical Surgery 13e
- Bailey & Love's Surgery 28e
- Mulholland & Greenfield's Surgery 7e
Incarcerated hernia vs Obstructed hernia
Incarcerated Hernia vs. Obstructed Hernia
The Core Issue — Terminology Confusion
USAGE 1 — S Das / Indian Surgery Textbooks ⭐ (Your Notes)
"Obstructed or Incarcerated Hernia (irreducibility + Intestinal Obstruction)" — S Das Manual of Clinical Surgery 13e
| Term | Meaning |
|---|---|
| Incarcerated | = Obstructed (irreducible + bowel lumen blocked, blood supply intact) |
| Obstructed | = Incarcerated (same thing) |
Incarcerated = Obstructed = Irreducibility + Intestinal Obstruction
(NO blood supply compromise)
USAGE 2 — Bailey & Love / Western Textbooks ⭐⭐
| Term | Bailey & Love Definition |
|---|---|
| Irreducible | Contents cannot return to abdomen; no vascular or bowel issue |
| Incarcerated | Irreducible + trapped + at risk of strangulation (not yet strangulated) |
| Obstructed | Irreducible + bowel lumen blocked (a specific consequence when bowel is in sac) |
| Strangulated | Irreducible + obstructed + blood supply arrested |
"The term 'incarcerated', literally 'in prison', means that a hernia is not only irreducible but also potentially developing strangulation." — Bailey & Love 28e
- Incarcerated = danger zone (irreducible, trapped, heading toward strangulation)
- Obstructed = specific complication when the sac contains bowel and the lumen is blocked
INCARCERATED (Bailey)
= Irreducible + Trapped + Risk of strangulation
↙ ↘
contains BOWEL contains OMENTUM only
↓ ↓
OBSTRUCTED May strangulate
(lumen blocked) without obstruction
Side-by-Side Comparison of Both Schools
| Feature | S Das (Indian texts) | Bailey & Love (Western) |
|---|---|---|
| Incarcerated = | Obstructed (same term) | Irreducible + trapped + at risk of strangulation |
| Obstructed = | Incarcerated (same term) | Specific complication - bowel lumen blocked |
| Are they the same? | ✅ Yes, synonyms | ❌ No, distinct stages |
| Blood supply in incarceration | Intact | Intact (but threatened) |
| Bowel obstruction in incarceration | ✅ Present (by definition) | ± May or may not be present |
What They Agree On
| Point | Both texts agree |
|---|---|
| Both are irreducible | ✅ |
| Blood supply is intact (not yet strangulated) | ✅ |
| Risk of progression to strangulation is HIGH | ✅ |
| Management: attempt reduction with sedation, then urgent repair | ✅ |
| Do NOT confuse with strangulation | ✅ |
Spectrum Diagram — Both Terminologies
Reducible → Irreducible → Obstructed/Incarcerated → Strangulated → Infarcted
(same stage)
Reducible → Irreducible → Incarcerated → Obstructed → Strangulated → Infarcted
(trapped, (bowel
at risk) lumen
blocked)
Clinical Features Comparison
| Feature | Incarcerated (Bailey) | Obstructed (S Das = Incarcerated) |
|---|---|---|
| Reducibility | ❌ Cannot reduce | ❌ Cannot reduce |
| Bowel lumen | May or may not be blocked | ✅ Blocked |
| Blood supply | Intact (threatened) | ✅ Intact |
| Colicky pain | ± | ✅ Present |
| Vomiting | ± | ✅ Present |
| Distension | ± | ✅ Present |
| Cough impulse | ± | ± Variable |
| Tenderness | Mild | Mild |
| Tense | Mildly | Mildly |
| Systemic signs | None | None |
| Urgency | ⚠️ Urgent | ⚠️ Urgent |
| Mesh | ✅ Yes | ✅ Yes |
Maingot's / Fischer's — Third View
"Patients presenting with acutely incarcerated, obstructed, or strangulated hernia contents usually require urgent or emergent repair."
For Your Exams — What to Write ⭐
Incarcerated = Obstructed = Irreducibility + Intestinal Obstruction, blood supply intact
- Incarcerated = irreducible + trapped + at risk (not yet strangulated, may or may not have obstruction)
- Obstructed = incarcerated hernia specifically containing bowel with lumen blocked
"Incarcerated hernia refers to an irreducible hernia with trapped contents. When this contains bowel and the lumen becomes blocked, it is called an obstructed hernia. In both states, blood supply remains intact, distinguishing them from strangulation."
- S Das Manual of Clinical Surgery 13e
- Bailey & Love's Surgery 28e
- Fischer's Mastery of Surgery 8e
Richter's Hernia