chest pain (gastrointestinal, coronary artery diseases musculoskeletal, psychogenic). definition, epidemiology,etiology, pathogenesis, histopathology, clinical features, diagnosis, management,prognosis, complications,and differential diagnosis (table). along with images
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Chest Pain: A Comprehensive Review
Overview
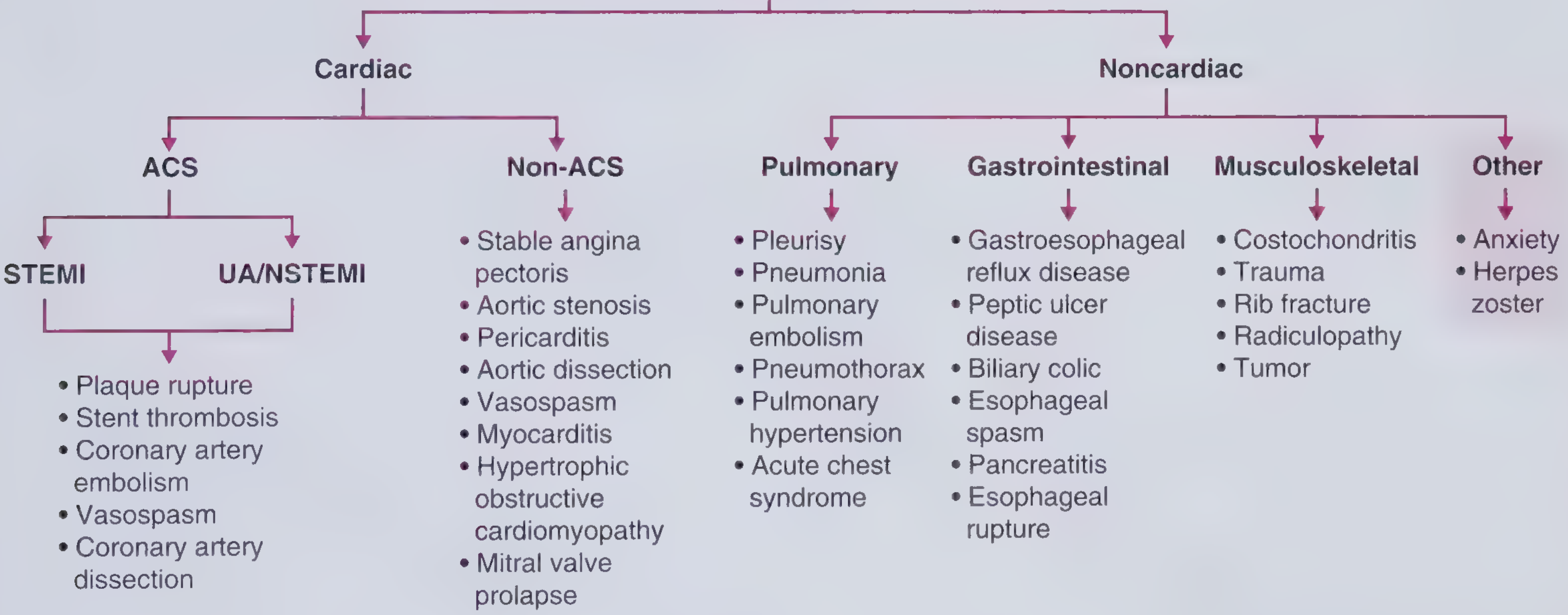
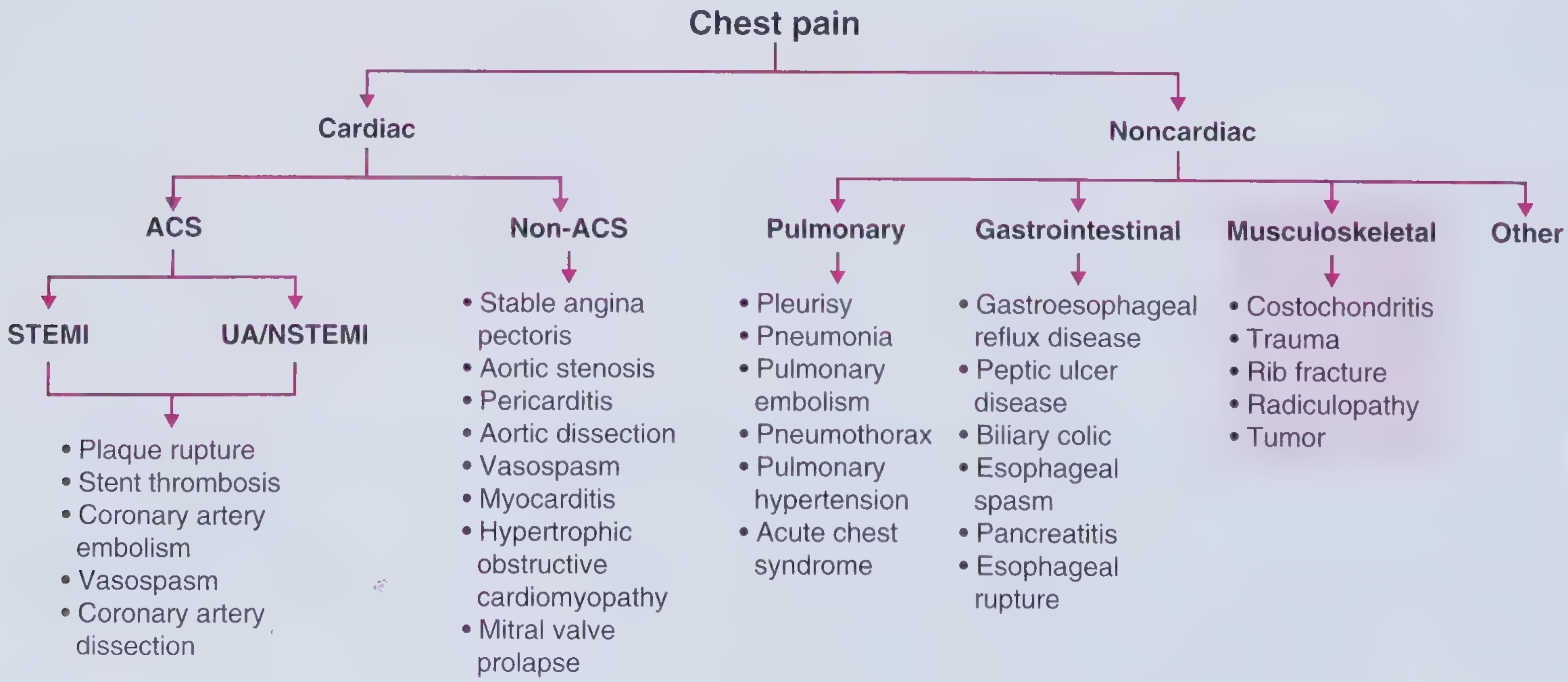
Chest pain is the cardinal manifestation of a wide spectrum of disorders. The clinician's primary task is to distinguish imminently life-threatening causes (acute coronary syndrome, aortic dissection, pulmonary embolism) from benign ones. The four major non-pulmonary categories are: gastrointestinal, coronary artery disease (CAD)/cardiac, musculoskeletal, and psychogenic.
PART 1: CORONARY ARTERY DISEASE (CAD) / ANGINA PECTORIS
1.1 Definition
Angina pectoris is characterized by paroxysmal, recurrent attacks of substernal or precordial chest discomfort caused by transient (15 seconds to 15 minutes) myocardial ischemia that is insufficient to induce myocyte necrosis. Angina pectoris is generally defined as a discomfort in the chest or adjacent areas that occurs predictably and reproducibly at a certain level of exertion and is relieved with rest or nitroglycerin.
Three overlapping patterns are recognized:
- Stable (typical) angina - the most common form; imbalance between chronic atherosclerotic coronary stenosis and increased myocardial demand. Does not occur at rest.
- Prinzmetal (variant) angina - episodic coronary artery spasm, unrelated to physical activity; can occur at rest; responds to vasodilators.
- Unstable angina - increasingly frequent, prolonged (>20 min), or severe angina at progressively lower activity levels or at rest; associated with plaque disruption, thrombosis, and distal embolization; a harbinger of MI.
(Robbins & Cotran Pathologic Basis of Disease)
1.2 Epidemiology
- More than 17 million Americans have coronary heart disease; nearly 10 million have angina pectoris.
- Among adults aged 60-79 years: ~25% of men and ~16% of women have coronary heart disease; these percentages rise to 37% and 23%, respectively, in those >80 years.
- Males constitute ~70% of all patients with angina pectoris, with an even greater proportion in those <50 years.
- Globally, cardiovascular disease accounts for an estimated 18 million deaths per year (32% of all global deaths, 2019 Global Burden of Disease data).
- Coronary heart disease accounted for 365,000 of ~650,000 U.S. heart disease deaths in 2019.
(Goldman-Cecil Medicine)
1.3 Etiology
| Type | Primary Mechanism |
|---|---|
| Stable angina | Fixed atherosclerotic coronary stenosis + increased oxygen demand |
| Unstable angina | Plaque rupture/erosion + superimposed thrombosis + vasospasm |
| Prinzmetal angina | Coronary artery vasospasm (with or without atherosclerosis) |
| Microvascular angina | Microvascular dysfunction (more common in women) |
Other precipitants include: tachycardia, anemia, thyrotoxicosis, fever, hypertension, aortic stenosis, hypertrophic cardiomyopathy, and cocaine use.
1.4 Pathogenesis
The ischemia-supply/demand mismatch operates through two main mechanisms:
- Demand angina - increased myocardial oxygen requirements (exertion, emotion, heavy meals, cold exposure) exceed what stenotic coronary arteries can deliver.
- Supply angina - diminished oxygen delivery due to vasospasm, plaque disruption, or microvascular disease.
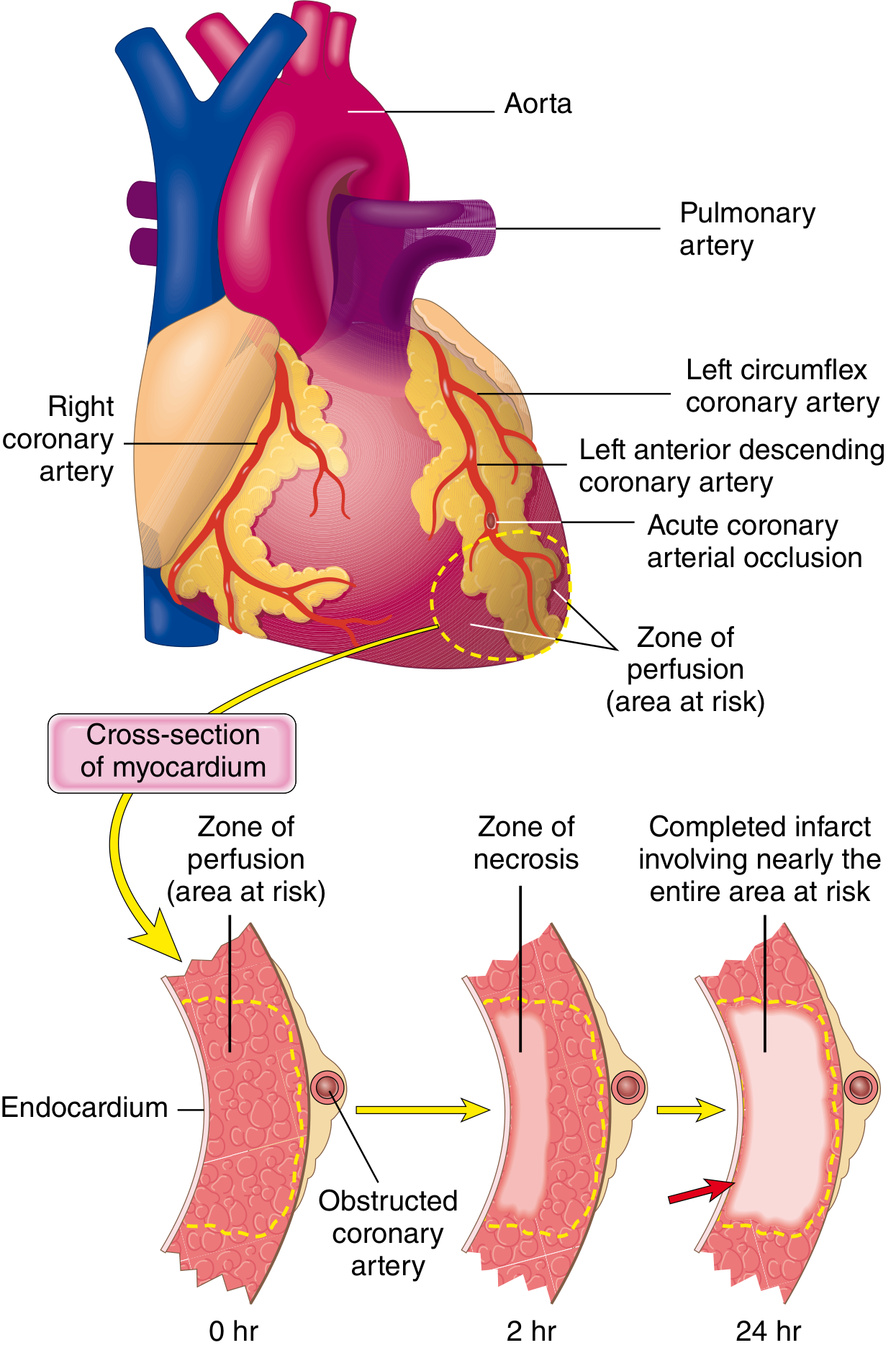
Sequence of MI pathogenesis:
- An atheromatous plaque is eroded or suddenly disrupted by endothelial injury or mechanical forces, exposing subendothelial collagen.
- Platelets adhere, aggregate, and are activated, releasing thromboxane A2, ADP, and serotonin - causing further platelet aggregation and vasospasm.
- Activation of coagulation via tissue factor adds to the growing thrombus.
- Within minutes, the thrombus can completely occlude the coronary lumen.
Anginal pain arises from ischemia-induced release of adenosine, bradykinin, and other molecules that stimulate sympathetic and vagal afferent nerves.
1.5 Histopathology
Atherosclerotic plaque: Fibrous cap overlying a lipid-rich necrotic core with foam cells, cholesterol clefts, calcification, and inflammatory infiltrate (macrophages, T lymphocytes). Plaque rupture exposes the thrombogenic core.
Temporal progression of myocardial necrosis:
| Feature | Time |
|---|---|
| Onset of ATP depletion | Seconds |
| Loss of contractility | <2 minutes |
| ATP reduced to 50% of normal | 10 minutes |
| Irreversible cell injury (necrosis) | 20-40 minutes |
| Microvascular injury | >1 hour |
| Complete necrosis of at-risk zone | 6-12 hours |
Early (reversible): glycogen depletion, myofibrillar relaxation, mitochondrial swelling.
Irreversible: sarcolemmal disruption, release of intracellular proteins (troponin, CK-MB) into the circulation.
(Robbins & Cotran Pathologic Basis of Disease)
1.6 Clinical Features
- Quality: Heaviness, pressure, squeezing, smothering, choking - rarely described as frank "pain"; patients may say "pressure, ache, discomfort, uneasy feelings."
- Location: Substernal; the classic Levine's sign - clenched fist placed over the sternum.
- Radiation: Left arm (especially ulnar aspect), left jaw, neck, back, interscapular region, epigastrium. Does NOT radiate to the trapezius (which suggests pericarditis instead).
- Duration: Stable angina: 2-5 minutes; relieved by rest or sublingual nitroglycerin. Unstable angina: >20 minutes; often occurs at rest.
- Precipitants: Exertion, emotion, cold temperature, heavy meals, sexual activity.
- Atypical presentations: Women, elderly, and diabetics may present with dyspnea, nausea, diaphoresis, fatigue, or jaw pain without classic chest discomfort.
Canadian Cardiovascular Society (CCS) Grading:
| Class | Description |
|---|---|
| I | Angina only with strenuous/prolonged activity |
| II | Angina with moderate exertion (walking >2 flights) |
| III | Angina with mild exertion (walking 1-2 flights); marked limitation |
| IV | Angina at rest or any activity; inability to perform any activity without symptoms |
1.7 Diagnosis
- ECG: ST depression (stable angina, NSTEMI), ST elevation (STEMI), T-wave inversions; Prinzmetal: transient ST elevation during spasm.
- Cardiac biomarkers: Troponin I/T (preferred), CK-MB - elevated in MI (not in stable angina alone).
- Stress testing: Exercise ECG, nuclear perfusion imaging, or stress echocardiography to provoke reversible ischemia.
- Coronary angiography: Gold standard for defining coronary anatomy and stenosis severity.
- CT coronary angiography (CTCA): Non-invasive alternative; excellent for ruling out obstructive CAD.
- Diamond-Forrester Classification: Typical angina (all 3): (1) substernal pressure-like pain, (2) precipitated by exertion/emotion, (3) relieved by rest or nitroglycerin <30 min. Atypical: 2 of 3. Noncardiac: ≤1 of 3.
1.8 Management
Anti-anginal therapy:
- Sublingual nitroglycerin - immediate relief of acute angina episodes
- Beta-blockers - reduce heart rate and contractility (decrease demand); first-line
- Calcium channel blockers - vasodilation and rate control; especially useful in Prinzmetal (vasospasm)
- Long-acting nitrates - adjunctive; tolerance may develop
- Ranolazine - late Na+ channel blocker; useful add-on
Risk factor modification (secondary prevention):
- Antiplatelet therapy (aspirin ± clopidogrel)
- Statins (LDL-lowering + plaque stabilization)
- ACE inhibitors/ARBs
- Control of hypertension, diabetes, smoking cessation
Revascularization:
- PCI (percutaneous coronary intervention) - for significant single-vessel or multi-vessel CAD
- CABG (coronary artery bypass grafting) - for left main disease, 3-vessel disease, or diabetics with multi-vessel disease
1.9 Prognosis
- Stable angina: generally benign with good medical management; annual mortality ~1-2% with modern therapy.
- Unstable angina/NSTEMI: significant risk of progression to STEMI or sudden cardiac death without intervention.
- STEMI: in-hospital mortality ~5-10% with modern reperfusion; higher without.
1.10 Complications
- Myocardial infarction
- Heart failure (systolic or diastolic)
- Cardiogenic shock
- Arrhythmias (ventricular fibrillation, complete heart block)
- Papillary muscle rupture / mitral regurgitation
- Ventricular septal defect (in MI)
- Sudden cardiac death
- Left ventricular aneurysm
- Dressler's syndrome (post-MI pericarditis)
PART 2: GASTROINTESTINAL CHEST PAIN
2.1 Definition
Gastrointestinal chest pain (also called noncardiac chest pain of GI origin) is retrosternal or epigastric discomfort arising from the esophagus or other GI structures that closely mimics cardiac angina. The adjective "noncardiac" should only be used when a cardiac origin has been excluded or made highly unlikely by cardiac evaluation.
The principal GI causes include:
- Gastroesophageal reflux disease (GERD) - the most common GI cause of chest pain
- Esophageal spasm (diffuse esophageal spasm, nutcracker esophagus)
- Peptic ulcer disease
- Biliary colic
- Esophageal rupture (Boerhaave syndrome)
(Yamada's Textbook of Gastroenterology; Sleisenger & Fordtran)
2.2 Epidemiology
- GERD affects ~20% of the Western population; it is one of the most common causes of noncardiac chest pain.
- Up to 30-50% of patients presenting to the ER with chest pain eventually have a non-cardiac (often GI) etiology identified.
- Esophageal causes account for up to 30-60% of noncardiac chest pain cases.
- GERD prevalence in asthmatics is estimated at 34-89%.
2.3 Etiology
| GI Cause | Key Etiologic Factor |
|---|---|
| GERD | Lower esophageal sphincter (LES) incompetence; hiatal hernia; delayed gastric emptying |
| Esophageal spasm | Abnormal esophageal motor function; visceral hypersensitivity |
| Peptic ulcer | H. pylori infection; NSAID use; acid hypersecretion |
| Biliary colic | Gallstones obstructing the cystic/common bile duct |
| Esophageal rupture | Forceful vomiting (Boerhaave); iatrogenic (endoscopy) |
| Functional chest pain | Visceral hypersensitivity; no structural cause (Rome IV criteria) |
2.4 Pathogenesis
GERD-related chest pain is multifactorial and poorly understood. Contributing mechanisms include:
- H+ concentration, volume, and duration of acid exposure on esophageal mucosa
- Secondary esophageal spasm triggered by acid reflux
- Prolonged contractions of longitudinal esophageal muscles
- Activation of pain-sensitive chemoreceptors and mechanoreceptors in the esophageal wall
- Referred pain through shared sensory afferents with the heart (explaining the angina-like quality)
Esophageal spasm: Abnormal, simultaneous, high-amplitude esophageal contractions cause both dysphagia and chest pain. Loss of neurons in the myenteric plexus (as in achalasia) or abnormal motor coordination may be involved.
2.5 Histopathology
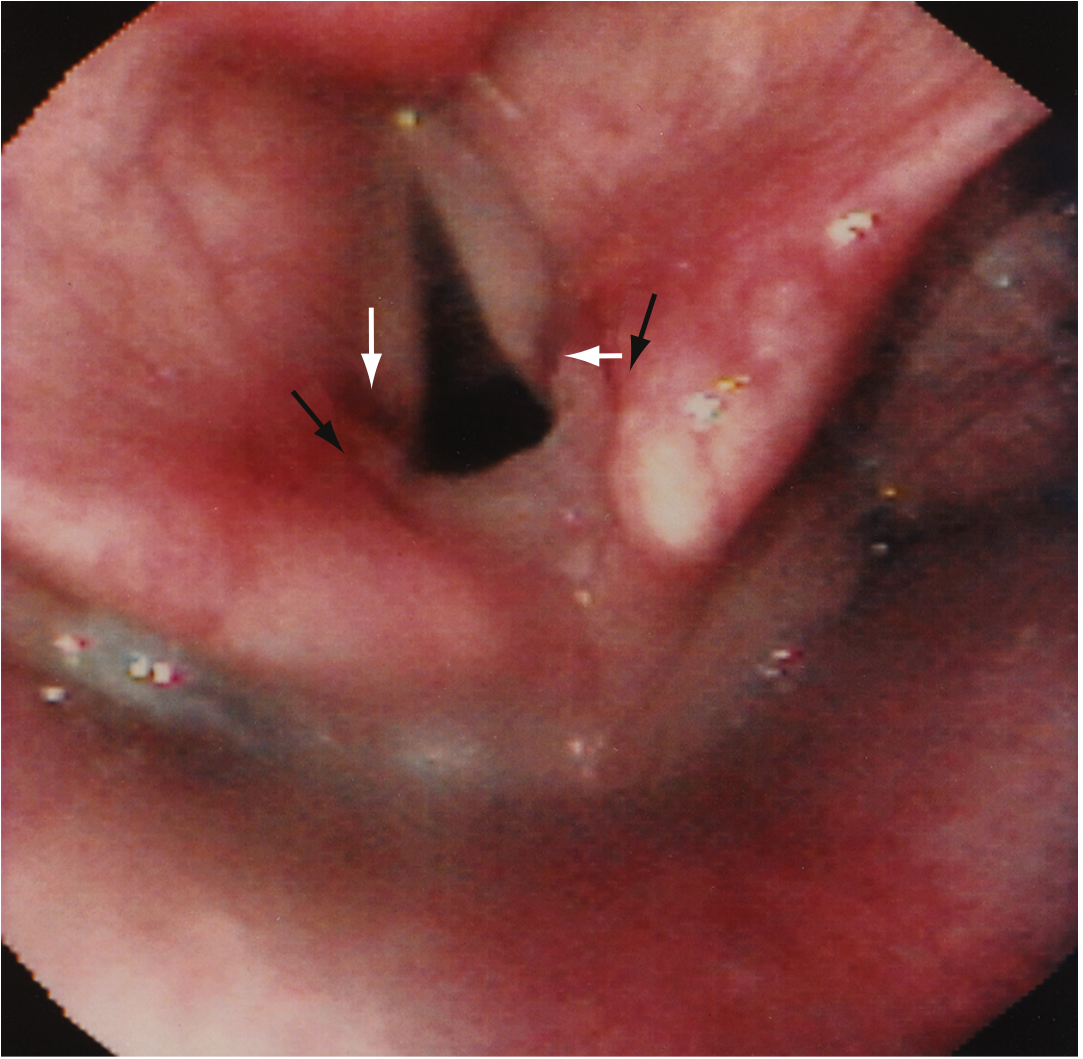
- GERD: Esophageal mucosa shows basal zone hyperplasia, elongated papillae, intraepithelial eosinophils, and dilated intercellular spaces. Chronic exposure leads to Barrett's esophagus (intestinal metaplasia with goblet cells).
- Peptic ulcer: Mucosal defect extending through the muscularis mucosae; active ulcers show neutrophilic infiltrate; chronic ulcers show fibrous base with granulation tissue.
- Esophageal spasm: No specific histologic changes; diagnosis is manometric.
2.6 Clinical Features
- GERD chest pain: Substernal burning or squeezing, often after meals, lying down, or bending over; may radiate to the back, neck, jaw, or arm - closely mimicking angina. Worsened by emotional stress. Lasts minutes to hours; often resolves spontaneously; may be eased by antacids.
- Associated features: Heartburn, regurgitation, sour taste, waterbrash, hoarseness, chronic cough, globus sensation.
- Esophageal spasm: Severe, intermittent substernal pain; may be associated with dysphagia; responds to nitroglycerin (mimicking angina even in its response to treatment).
- Biliary colic: Severe right upper quadrant or epigastric/chest pain, typically post-prandial (especially fatty meals); radiates to the right shoulder or scapula; nausea and vomiting.
2.7 Diagnosis
- Upper endoscopy (EGD): Identifies esophagitis, Barrett's mucosa, peptic ulcer, malignancy.
- 24-hour esophageal pH monitoring / pH-impedance testing: Gold standard for diagnosing GERD; correlates symptoms with acid reflux events.
- Esophageal manometry: Diagnoses esophageal motility disorders (spasm, achalasia, nutcracker esophagus).
- PPI (proton pump inhibitor) trial: A clinical diagnostic test - chest pain episodes associated with documented reflux typically respond to acid antisecretory therapy.
- Ultrasound abdomen: For gallstones and biliary pathology.
- Esophagram (barium swallow): Useful for structural abnormalities.
- Cardiac workup first: Cardiac origin must be excluded before attributing chest pain to GI cause.
2.8 Management
- GERD: Lifestyle modification (weight loss, head-of-bed elevation, avoiding precipitants); PPI therapy (first-line); H2 blockers; antacids for breakthrough. Fundoplication (Nissen) for refractory GERD.
- Esophageal spasm: Calcium channel blockers, nitrates, PPIs (if co-existing GERD), low-dose tricyclic antidepressants; botulinum toxin injection for severe cases.
- Peptic ulcer: H. pylori eradication (triple therapy); PPI therapy; stop NSAIDs.
- Biliary colic: Laparoscopic cholecystectomy (definitive); analgesics for acute episodes.
- Functional chest pain: CBT; low-dose antidepressants (TCAs, SSRIs); visceral analgesics.
2.9 Prognosis
- GERD: excellent with PPI therapy; risk of Barrett's esophagus (~10-15% of chronic GERD) and esophageal adenocarcinoma with untreated long-standing disease.
- Esophageal spasm: benign but recurrent; rarely progressive.
- Esophageal rupture: life-threatening; requires urgent surgical intervention.
2.10 Complications
- Barrett's esophagus → esophageal adenocarcinoma
- Esophageal stricture (peptic)
- Aspiration pneumonia, pulmonary fibrosis (from GERD)
- Obstructive sleep apnea worsening
- Boerhaave syndrome (esophageal rupture) - fatal if untreated
PART 3: MUSCULOSKELETAL CHEST PAIN
3.1 Definition
Musculoskeletal chest pain arises from disorders of the chest wall, ribs, costal cartilages, thoracic spine, or shoulder girdle. It is one of the most common causes of chest pain in primary care and emergency settings, and is generally benign and self-limiting.
Principal causes:
- Costochondritis - inflammation of costal cartilages (Tietze syndrome if visible swelling is present)
- Chest wall trauma / rib fracture
- Cervical angina (radiculopathy) - chest pain from cervical nerve root compression (C4-C8)
- Chest wall tumors (rare)
- Precordial catch syndrome (Texidor's twinge) - benign, especially in young people
3.2 Epidemiology
- Musculoskeletal disorders account for 20-40% of chest pain presentations in primary care and emergency settings.
- Costochondritis is particularly common in young adults and adolescents.
- In pediatric chest pain, musculoskeletal causes (including costochondritis and precordial catch syndrome) are the leading identifiable cause.
- Rib fractures are more common in the elderly (osteoporosis) and in those with trauma or malignancy.
3.3 Etiology
| Condition | Etiology |
|---|---|
| Costochondritis | Idiopathic inflammation of costal cartilages; may follow upper respiratory infection or physical strain |
| Tietze syndrome | Costochondritis WITH visible/palpable swelling at the costochondral junction |
| Rib fracture | Trauma, osteoporosis, pathological (malignancy, infection) |
| Cervical angina | Cervical nerve root compression (C4-C8) - most commonly degenerative disc disease |
| Precordial catch syndrome | Unknown; thought to involve parietal pleura or intercostal muscles; benign |
| Chest wall tumor | Soft tissue sarcoma (most common primary malignant chest wall tumor); also chondrosarcoma, osteosarcoma, plasmacytoma |
3.4 Pathogenesis
- Costochondritis: Inflammation (likely mechanical or post-infectious) of the costal cartilages at the costochondral or sternocostal junctions. Typically affects the 2nd-5th costal cartilages.
- Cervical angina: Compression of cervical nerve roots (C4-C8) - by herniated disc, osteophytes, or foraminal stenosis - produces referred pain to the chest, mimicking angina. The dermatomal distribution of these roots overlaps with the precordial region.
- Rib fractures: Periosteal pain receptors are activated; breathing and movement aggravate pain due to chest wall motion.
3.5 Histopathology
- Costochondritis: Non-specific perichondral and cartilaginous inflammation with edema and neutrophilic or lymphocytic infiltrate in acute stages. No specific histologic criteria required (clinical diagnosis).
- Tietze syndrome: Swelling due to hypertrophy of costal cartilage ± inflammatory changes.
- Chest wall tumors: Vary by type - chondrosarcoma shows chondroid matrix; soft tissue sarcoma shows pleomorphic spindle cells.
3.6 Clinical Features
- Location: Usually well-localized, anterior chest wall; often unilateral.
- Quality: Sharp, aching, or pleuritic.
- Key diagnostic feature: Pain reproducible on direct palpation of the chest wall - this is the hallmark that distinguishes musculoskeletal pain from angina.
- Costochondritis: Tenderness at costochondral or sternocostal junctions (2nd-5th ribs most commonly). No visible swelling (distinguishes from Tietze syndrome).
- Precordial catch syndrome: Sudden, sharp, focal pain - usually left peri-apical area; worsened by inspiration; resolves within minutes; not associated with dyspnea or dysrhythmias. Patients may say pain "took my breath away."
- Cervical angina: Chest pain associated with neck pain; often associated with arm/shoulder symptoms; may worsen with neck movement.
- Rib fracture: Localized tenderness over a rib; worsened by deep inspiration, coughing, or direct pressure.
3.7 Diagnosis
- Clinical examination: Reproduced by chest wall palpation - the most important test.
- Chest X-ray: To exclude rib fractures, pneumothorax, pleural disease; may miss non-displaced fractures.
- CT thorax: More sensitive for rib fractures and chest wall masses.
- MRI/cervical spine: For suspected cervical radiculopathy.
- Bone scan: For occult fractures or metastatic disease.
- ECG and cardiac workup: Should be performed first to rule out cardiac cause, especially in those with risk factors.
3.8 Management
- Costochondritis and rib fracture: NSAIDs (first-line), acetaminophen, local ice/heat; rest; intercostal nerve block for severe rib fracture pain; adequate analgesia to allow deep breathing.
- Cervical angina: Physical therapy, cervical traction, NSAIDs; surgical decompression for refractory cases.
- Precordial catch syndrome: Reassurance; self-limited; NSAIDs rarely needed.
- Tietze syndrome: NSAIDs; local corticosteroid injection for refractory cases.
- Chest wall tumors: Surgical resection is the primary treatment; adjuvant therapy depends on histology.
3.9 Prognosis
- Costochondritis and precordial catch syndrome: benign, self-limiting; excellent prognosis.
- Rib fractures: good with conservative management; complications more common in elderly or with multiple fractures (flail chest).
- Cervical angina: good with appropriate treatment; may recur if underlying disc disease progresses.
3.10 Complications
- Multiple rib fractures: flail chest, pneumothorax, hemothorax
- Untreated chest wall malignancy: local extension, metastasis
- Chronic pain syndromes (costochondritis can rarely become chronic)
PART 4: PSYCHOGENIC CHEST PAIN
4.1 Definition
Psychogenic chest pain (also called functional chest pain or cardiac neurosis) is chest pain in which no structural cardiac, pulmonary, gastrointestinal, or musculoskeletal cause can be identified. The most common psychogenic cause is panic disorder / anxiety. It is classified under "functional chest pain of presumed esophageal origin" by Rome IV criteria if esophageal hypersensitivity is the mechanism, or as a somatic symptom disorder / panic disorder under DSM-5.
4.2 Epidemiology
- Psychogenic causes account for approximately 10-30% of all noncardiac chest pain presentations.
- Panic disorder is the most frequently identified psychiatric condition associated with unexplained chest pain; up to 30-60% of patients with recurrent noncardiac chest pain meet criteria for panic disorder.
- Psychogenic chest pain is more common in young women and in patients with a history of anxiety, depression, or prior physical abuse.
- Patients with panic disorder also have higher rates of agoraphobia, major depression, and substance abuse.
4.3 Etiology
- Panic disorder / panic attacks - the most common cause
- Generalized anxiety disorder (GAD)
- Major depressive disorder
- Somatization disorder / somatic symptom disorder
- Hyperventilation syndrome - lowered PCO2 causes cerebral vasoconstriction, alkalosis, and peripheral paresthesias
- Functional/visceral hypersensitivity - lowered pain thresholds in the esophagus or chest wall
- da Costa's syndrome (soldier's heart) - historically described in wartime; functional cardiac disorder
4.4 Pathogenesis
- Autonomic dysregulation: Anxiety and panic trigger sympathetic hyperactivation, causing tachycardia, palpitations, and chest tightness - symptoms that are interpreted catastrophically by the patient.
- Hyperventilation: Leads to hypocapnia and respiratory alkalosis, causing coronary artery spasm, chest tightness, paresthesias, dizziness, and dyspnea.
- Central sensitization: Altered pain perception in the central nervous system lowers visceral pain thresholds.
- Cognitive amplification: Catastrophic misinterpretation of benign bodily sensations (e.g., palpitations from anxiety misread as heart attack) triggers a feedback cycle.
- The chest pain of panic disorder can be explained by increased wall tension of the esophagus, intercostal muscle spasm, and autonomic activation.
4.5 Histopathology
There are no specific histopathologic findings in psychogenic chest pain. The condition is defined by the absence of structural or organic pathology. Relevant psychiatric pathology exists at the level of central nervous system neurotransmitter dysregulation (serotonin, norepinephrine, GABA) rather than in any tissue biopsy.
4.6 Clinical Features
- Quality: Typically sharp, stabbing, or vague; sometimes pressure-like (can mimic angina)
- Location: Variable; often left precordial or diffuse
- Duration: Can last seconds to hours; often prolonged compared with angina
- Associated features: Palpitations, dyspnea, diaphoresis, trembling, nausea, dizziness, depersonalization, fear of dying - classic panic attack features (4+ symptoms, peaking within 10 minutes)
- Triggers: Stress, anxiety-provoking situations; may occur without obvious trigger
- Response to treatment: Responds poorly to nitroglycerin and antacids; responds well to anxiolytics, breathing techniques, and CBT
- No reproducibility on palpation (unlike musculoskeletal pain)
- Normal cardiac workup despite often recurrent presentations
4.7 Diagnosis
- Diagnosis of exclusion - cardiac, pulmonary, GI, and musculoskeletal causes must be ruled out first.
- DSM-5 criteria for panic disorder: recurrent unexpected panic attacks + persistent concern about future attacks or maladaptive behavior changes.
- Psychiatric evaluation: PHQ-9 (depression screening), GAD-7 (anxiety screening).
- Hyperventilation provocation test: Voluntary hyperventilation for 2-3 minutes reproducing symptoms.
- Cardiac workup: ECG, troponin, exercise stress test - all normal.
- Normal endoscopy and pH studies (distinguishes from GERD).
4.8 Management
- The majority of patients with panic disorder can be effectively treated with either nonpharmacologic or pharmacologic modalities:
- Cognitive Behavioral Therapy (CBT) - first-line, most effective long-term treatment; addresses catastrophic thinking and avoidance
- SSRIs (e.g., paroxetine, sertraline, escitalopram) - first-line pharmacotherapy; takes 4-6 weeks for full effect
- SNRIs (venlafaxine) - alternative first-line pharmacotherapy
- Benzodiazepines - short-term relief; risk of dependence; not for long-term use
- Tricyclic antidepressants (TCAs) - imipramine; effective but side-effect profile limits use
- Breathing retraining: Diaphragmatic breathing to prevent hyperventilation
- Patient education and reassurance: Critical to break the fear-symptom-fear cycle
4.9 Prognosis
- With appropriate treatment, the majority of patients with panic disorder have good outcomes.
- Untreated panic disorder tends to be chronic and disabling.
- Risk of developing agoraphobia and major depression if untreated.
- Recurrent ER visits for chest pain are common, with high healthcare utilization.
4.10 Complications
- Agoraphobia
- Major depressive disorder
- Substance abuse
- Social and occupational disability
- Increased cardiovascular risk (chronic anxiety is an independent cardiovascular risk factor)
- Iatrogenic harm from repeated unnecessary cardiac investigations
DIFFERENTIAL DIAGNOSIS TABLE
| Feature | CAD/Angina | GI (GERD/Esophageal) | Musculoskeletal | Psychogenic/Panic |
|---|---|---|---|---|
| Pain quality | Squeezing, pressure, heaviness; rarely "pain" | Burning, squeezing; heartburn | Sharp, aching, localized | Sharp, stabbing, or vague pressure |
| Location | Substernal, diffuse | Substernal, epigastric | Anterior chest wall, focal | Left precordial or diffuse |
| Radiation | Left arm, jaw, neck, back | Back, neck, jaw, arm | Neck, shoulder, arm (in radiculopathy) | Variable; may not radiate |
| Duration | 2-5 min (stable); >20 min (unstable) | Minutes to hours | Hours to days | Seconds to hours; often prolonged |
| Onset | Exertion, emotion, cold, meals | After meals, lying down, bending | Movement, inspiration, palpation | Stress, anxiety, or spontaneous |
| Relieved by | Rest, nitroglycerin | Antacids, PPIs, sitting upright | Rest, NSAIDs, heat/ice | Anxiolytics, deep breathing, reassurance |
| Worsened by | Exertion, cold, stress, meals | Meals, supine, bending, alcohol | Chest wall movement, palpation, deep breath | Anxiety-provoking situations; hyperventilation |
| Reproducible on palpation | NO | NO | YES (hallmark) | NO |
| Response to nitroglycerin | Yes (also esophageal spasm!) | Sometimes (esophageal spasm) | No | No |
| Associated symptoms | Dyspnea, diaphoresis, nausea | Heartburn, regurgitation, hoarseness, cough | Neck pain, shoulder pain | Palpitations, dyspnea, dizziness, paresthesias, fear of death |
| Age/sex | Men >50 yrs; women >60 yrs | Any age; common in obese/GERD patients | Any age; young adults for costochondritis | Young adults; women |
| ECG | ST depression/elevation, T-wave changes | Normal | Normal | Normal (sinus tachycardia during panic) |
| Troponin | Elevated in MI/NSTEMI | Normal | Normal | Normal |
| CXR | Cardiomegaly, pulmonary edema (in HF) | Normal | May show rib fracture or mass | Normal |
| Endoscopy | Normal | Esophagitis, peptic ulcer | Normal | Normal |
| Key diagnostic test | ECG, troponin, stress test, angiography | 24-hr pH monitoring, manometry, EGD | Chest wall palpation, X-ray | Psychiatric evaluation, exclusion of organic cause |
| Histopathology | Atherosclerosis, myocyte necrosis | Mucosal inflammation, Barrett's | Cartilage/perichondral inflammation | No pathologic findings |
| Management | Beta-blockers, nitrates, CCBs, antiplatelet, statins, PCI/CABG | PPIs, H2 blockers, lifestyle; fundoplication | NSAIDs, rest, nerve block | SSRIs, CBT, breathing retraining |
| Prognosis | Variable; good with revascularization; MI risk | Excellent with treatment; Barrett's risk | Excellent (usually) | Good with treatment; chronic if untreated |
Key Clinical Pearls
- Always exclude cardiac causes first - especially in those with risk factors (hypertension, diabetes, smoking, family history, hyperlipidemia, age >45 men / >55 women).
- The Levine sign (clenched fist over sternum) is classic for angina. A finger pointing to a small, focal spot is less likely to be ischemic.
- Reproducible chest wall tenderness on palpation strongly favors a musculoskeletal cause - but does NOT fully exclude cardiac pathology.
- Nitroglycerin responsiveness is not specific for CAD - esophageal spasm also responds to nitroglycerin.
- Women, elderly, and diabetics often present atypically with CAD - dyspnea, jaw pain, nausea, or fatigue may be the dominant symptom.
- Panic disorder is extremely common in the emergency department chest pain population; a good psychiatric history after cardiac workup is essential.
- GI chest pain is the most common noncardiac mimic of angina; a therapeutic PPI trial is both diagnostic and therapeutic.
Sources:
- Robbins & Cotran Pathologic Basis of Disease (9780443264528)
- Goldman-Cecil Medicine International Edition (9780323930345)
- Harrison's Principles of Internal Medicine, 22nd Ed. (9781265977061)
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease (9780323609623)
- Yamada's Textbook of Gastroenterology, 7th Ed. (9781119600169)
- Fuster & Hurst's The Heart, 15th Ed. (9781264257560)
- Frameworks for Internal Medicine (9781496359308)
This is a shared conversation. Sign in to Orris to start your own chat.