Pancreatitis cause
Reading File
Finding Sources
Searching PubMed
"pancreatitis"[MeSH Terms] AND "etiology"[MeSH Terms]
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a detailed breakdown of the causes of pancreatitis, drawn from Harrison's Principles of Internal Medicine 22E (2025) and Robbins Pathologic Basis of Disease.
Causes of Pancreatitis
Common Causes (account for 80-90% of cases)
| Cause | Details |
|---|---|
| Gallstones | Leading cause overall (30-60% of cases). Small stones <5 mm carry 4x the risk of larger ones. Cause pancreatitis by obstructing the common bile duct or pancreatic duct. |
| Alcohol | Second most common (15-30% of U.S. cases). Heavy/chronic use. Interestingly, actual incidence of pancreatitis in heavy drinkers is only ~5/100,000 - other cofactors (genetics, smoking) influence susceptibility. |
| Hypertriglyceridemia | Causes 1-4% of cases; triglycerides usually >1,000 mg/dL. Often seen in uncontrolled diabetes. Any drug or factor that abruptly raises triglycerides (e.g., oral contraceptives, alcohol) can precipitate it. |
| Post-ERCP | Occurs in 5-10% of ERCP procedures. Risk is reduced with pancreatic duct stents and rectal indomethacin. |
| Idiopathic | No cause found in a significant proportion of cases (up to 13-34% in children). |
Uncommon Causes
Drugs (<2% of all cases; cause pancreatitis via hypersensitivity or toxic metabolite):
- Azathioprine, 6-mercaptopurine
- Sulfonamides, tetracycline
- Valproic acid (most frequent drug cause in children)
- L-asparaginase, prednisone
- Estrogens, 5-ASA
- DPP4 inhibitors (gliptins) - evidence supports increased risk; GLP-1 receptor agonists do NOT appear to increase risk per recent meta-analysis of cardiovascular outcome trials
Metabolic:
- Hypercalcemia (e.g., hyperparathyroidism)
- Deficiency of apolipoprotein CII (impairs triglyceride clearance)
Anatomic/Structural:
- Pancreas divisum (most common congenital anomaly of the pancreas)
- Periampullary diverticulum
- Choledochocele
Genetic/Hereditary:
- Hereditary pancreatitis
- Cystic fibrosis
- SPINK1 and CFTR mutations (especially in recurrent childhood pancreatitis)
Infections:
- Viruses: mumps, coxsackievirus, CMV, EBV, echovirus, enteroviruses
- Parasites: Ascaris lumbricoides, Clonorchis sinensis
Neoplastic:
- Pancreatic cancer
- Intraductal papillary mucinous neoplasm (IPMN) - must be excluded in recurrent unexplained pancreatitis
Autoimmune:
- Autoimmune pancreatitis (type 1 and type 2)
- Connective tissue disorders, SLE, TTP
Other:
- Trauma (especially blunt abdominal trauma)
- Renal failure/uremia
- Postoperative (abdominal and non-abdominal surgery)
- Ischemia
- Kawasaki disease, hemolytic uremic syndrome (in children)
Pathogenic Mechanisms - Three Pathways
The diagram below from Robbins Pathology illustrates how these diverse causes all converge on one final pathway - acinar cell injury and inappropriate enzyme activation:
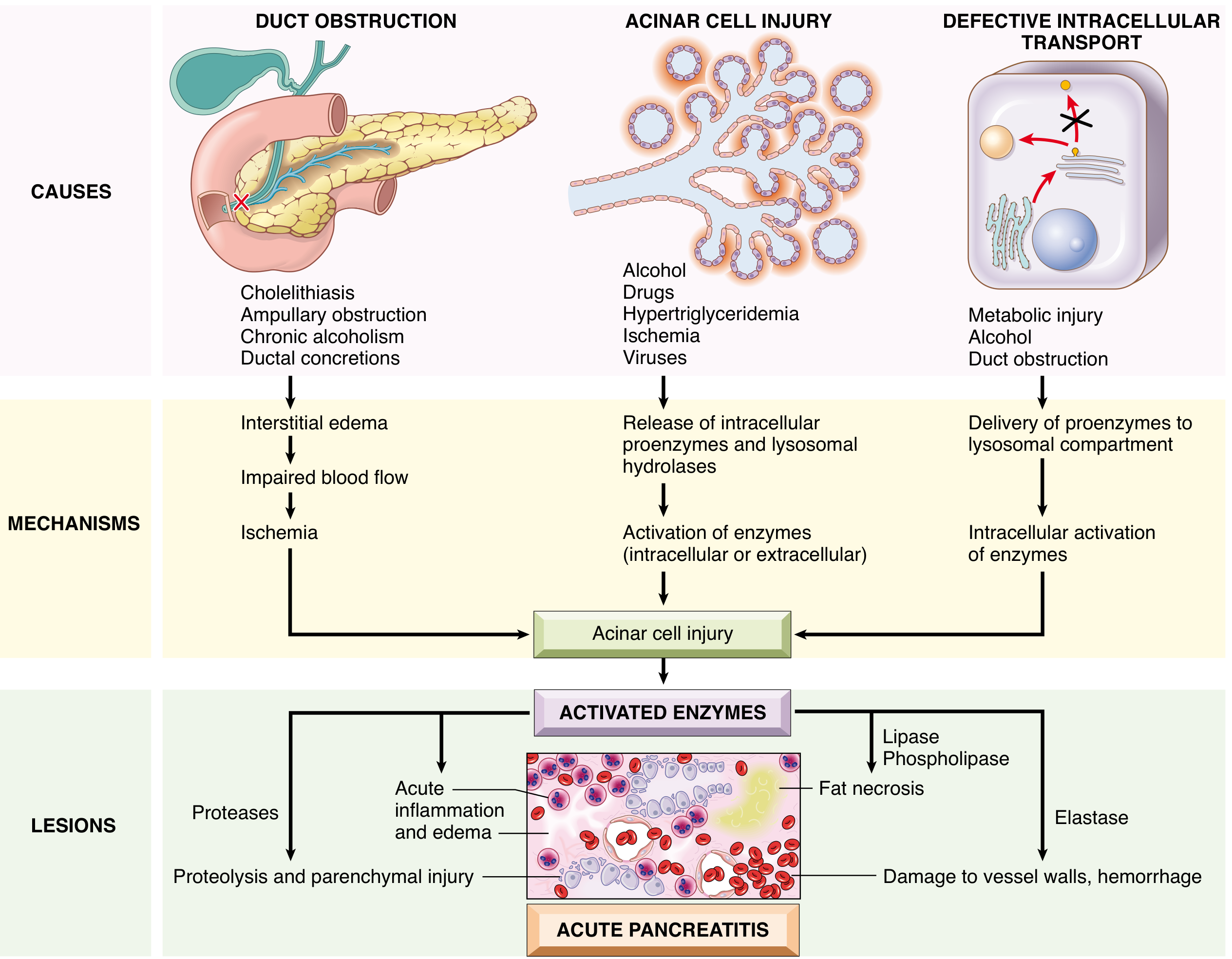
- Duct obstruction (gallstones, strictures, tumors): raises ductal pressure → interstitial edema → ischemia → acinar injury
- Direct acinar cell injury (alcohol, drugs, hypertriglyceridemia, viruses, ischemia): releases proenzymes and lysosomal hydrolases → intracellular/extracellular enzyme activation
- Defective intracellular transport (metabolic injury, alcohol, duct obstruction): proenzymes delivered to lysosomal compartment → intracellular enzyme activation
All three pathways converge on activated trypsin, which then activates other proteases (causing proteolysis), lipase/phospholipase (causing fat necrosis), and elastase (damaging vessel walls and causing hemorrhage).
Sources: Harrison's Principles of Internal Medicine 22E (2025), p. 2787 | Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 818 | Sleisenger and Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.